How Much a Cardiac Resynchronization Therapy Owner Can Make at $938M
Cardiac Resynchronization Therapy Services
You’re modeling owner income from a cardiac resynchronization therapy service, not a guaranteed cardiologist salary In the provided first-year plan, cardiac resynchronization therapy, or CRT, revenue is $938M, with $713M left after listed device, lab, referral, billing, and collection cost percentages Owner take-home comes after payroll, fixed overhead, debt service, reserves, taxes, and reinvestment
Owner income$6.7M EBITDANet margin71%Revenue for target pay$9.4MBusiness difficultyHard
Want to test your CRT owner take-home?
Owner income calculator
Estimate owner take-home from revenue, margin, operating costs, reserves, and your target pay for a cardiac resynchronization practice.
!
Planning note This is a researched planning estimate, not guaranteed salary, tax advice, or owner distribution advice.
How do you check owner income in the Cardiac Resynchronization Therapy Services model?
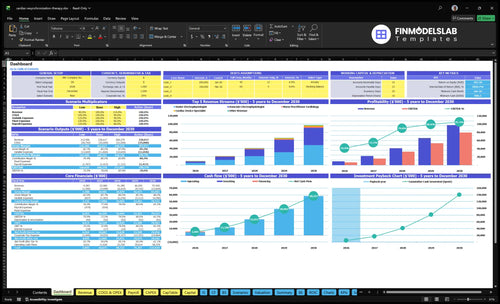
Open the Cardiac Resynchronization Therapy Services Financial Model Template to review the dashboard tab for revenue, contribution margin, implant cases, monitoring volume, costs, reserves, and owner income. The assumptions tab covers senior electrophysiologists, associate electrophysiologists, cardiac device specialists, nurse practitioners, and remote monitoring technicians, with charts and tables for volume, payer mix, device costs, overhead, debt, and owner pay.
Owner-income model highlights
Owner income output
$938M to $9,756M
760% to 805% margin
550% to 900% capacity
240% to 195% costs
What affects CRT service profit margin?
For Cardiac Resynchronization Therapy Services, margin is most sensitive to reimbursement, payer mix, and device and lead kit cost; if you need the setup context, see How To Write A Business Plan For Cardiac Resynchronization Therapy Services?. The quick math is simple: first-year listed costs load to 240%, then ease to 195% in a mature year, which raises contribution margin from 760% to 805%.
Big margin drivers
120% device and lead kits
50% catheterization lab fees
40% billing and collection fees
30% referral outreach costs
Risks to model
Payer validation changes cash timing
Prior auth delays slow revenue
Denials hit collection rates
Complications and revisions add cost
Can a CRT service scale owner income?
Yes—Cardiac Resynchronization Therapy Services can raise owner income when volume, staffing, quality, credentialing, and payer access grow together. In the model, staffing expands from 1 senior electrophysiologist, 1 associate electrophysiologist, 2 cardiac device specialists, 2 nurse practitioners, and 1 remote monitoring technician in year 1 to 5, 6, 8, 10, and 5 in the mature year, while revenue rises from $938M to $9,756M. Owner income is stronger if the founder is the implanting physician, because a manager of employed clinicians captures a smaller share.
Income scale
More volume lifts the income pool.
More staff supports more procedures.
More quality helps keep referrals coming.
More payer access widens patient flow.
Main limits
Hospital privileges can cap growth.
Specialist hiring can slow expansion.
Referral depth drives case volume.
Compliant remote monitoring is required.
Is a cardiac resynchronization therapy service profitable?
Yes, Cardiac Resynchronization Therapy Services can be profitable under the provided assumptions, but contribution is not owner pay; for planning structure, see How To Write A Business Plan For Cardiac Resynchronization Therapy Services?. The model shows $938M in first-year revenue and $713M contribution before payroll and fixed overhead, so distributions depend on referral access, payer mix, implant capacity, and site economics.
Profit Signals
$938M first-year revenue
$713M pre-overhead contribution
Referral volume drives capacity use
Payer mix controls collections
Watch-outs
240% listed cost percentages need review
Payroll can absorb contribution
Malpractice, rent, and debt matter
Facility margin beats professional fees
Cardiac Resynchronization Therapy Services Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
Want the six CRT income drivers?
1
Implant Volume
196 cases
More implant cases and tighter referral flow lift revenue fastest, and the model starts at 196 first-year cases.
2
Payer Mix
$9.4M
Better payer mix and cleaner collections raise realized revenue per case, so the same volume turns into more owner cash.
3
Site Economics
76%
Lower lab fees keep more of each implant after the site cut, which protects margin on every procedure.
4
Supply Control
24%
Device and lead kit savings move straight into EBITDA because they hit every implant case.
5
Lab Utilization
$97.6M
Higher lab use spreads the salaried team across more cases, which drops cost per procedure as volume rises.
6
Follow-up Retention
81%
Better follow-up keeps remote monitoring volume recurring and feeds repeat referrals, which supports future income.
Cardiac Resynchronization Therapy Services Core Six Income Drivers
CRT Implant Case Volume
Volume Drives Income
The model’s first-year volume uses the supplied 15 senior and 12 associate monthly treatment assumptions, landing near 196 annual cases. In a mature year, the service can reach about 1,890 cases with 5 senior and 6 associate electrophysiologists. More cases matter because fixed lab and billing costs get spread over a larger base.
Referral Flow
Steady qualified referrals are the real engine here. The main sources are cardiologists, heart failure clinics, primary care physicians, and hospital discharge pathways. One line says it best: referrals first, capacity second. CRT volume should follow clinical need, not sales pressure.
Stage Staffing Slowly
Do not build staff to the mature-year case count on day one. If hiring outruns eligible patient flow, overhead rises before revenue does, and owner take-home gets squeezed. Start around the 196-case pace, then add labor only when referral conversion and scheduling stay stable. That keeps growth tied to real volume.
Keep It Clinical
Do not try to create demand without a clinical indication. The business works when appropriate patients are identified, evaluated, and referred through the right pathways. That protects quality, keeps the pipeline credible, and avoids spending against cases that should never have been pursued.
CRT Reimbursement and Payer Mix
Cash per Case
CRT reimbursement is a cash question, not a sticker-price question. The main drivers are net collections per case, collection timing, payer mix, and denials. A practice can quote a price, but realized revenue only shows up after payer contracts and local collection history prove what actually lands.
First-Year Price
In the model, first-year implant planning prices are $45,000 for senior electrophysiologist cases and $42,000 for associate electrophysiologist cases. That is gross planning revenue, not collectible cash. Use local payer contracts, payer mix, and prior collections to convert that estimate into expected cash.
Mature-Year Price
In the mature-year model, prices rise to $50,000 for senior cases and $46,000 for associate cases. The lift only matters if collections keep pace. Medicare, Medicare Advantage, and commercial insurance can change realized revenue materially, especially when authorization slows payment.
Planning Rule
Plan from local payer contracts and collection history, not from billed price alone. If denials or authorization delays stretch cash, reported revenue can look fine while operating cash stays tight. Here’s the quick math: price minus write-offs, slow pays, and denials tells you the cash you can actually use.
CRT Site-of-Service Economics
Who Gets Paid
CRT owner income is not one number. It changes with who keeps the facility margin. If the owner earns professional fees only, take-home is much thinner; if the owner also participates in the catheterization lab, the same case volume can pay very differently.
Fee Split
Here’s the quick math: in the model, catheterization lab facility fees are 50% of revenue in year one, then 40% in the mature year. That means the facility share is a major driver of owner profit, not just case count.
Site Mix
Hospital privileges, co-management, ambulatory surgery center participation where permitted, and practice-owned service-line economics can all change the split. The same CRT implant can create different take-home depending on whether the owner captures only professional fees or also the site-of-service margin.
Compliance Check
Any ownership setup needs a professional review of Stark Law, anti-kickback, credentialing, and payer rules. Don’t assume a profitable structure is a compliant one; site-of-service economics can change fast when those rules limit who may bill, own, or share facility revenue.
CRT Device and Supply Costs
Device mix
CRT device cost is driven by device type, lead complexity, and generator price. The model starts with 120% of revenue in year one, then falls to 100% in the mature year. On $938M of first-year revenue, each basis point of device cost moves contribution by about $93,834.
Cost build
Build the estimate from case mix, vendor quotes, lead count, generator type, and months of inventory on hand. Add pass-through rules and who owns stock. One line item can hide a lot, so separate device and lead kits from clinical labor and overhead.
Quote generators and leads separately
Track consigned versus owned stock
Count waste, returns, and credits
Control waste
Tight vendor terms, lean stocking, and clear ownership can cut cash tied up in inventory and reduce expiry loss. Validate local pass-through treatment before relying on savings. Keep the clinical choice separate from the cost choice; don’t pick a device only because it protects margin.
Use fewer rush orders
Reconcile stock monthly
Audit expired items fast
Vendor terms
Validate vendor agreements, inventory ownership, and pass-through treatment locally before you book savings. The biggest swing comes from supply discipline: fewer unused kits, cleaner credit terms, and no surprise write-offs from expired or opened items.
CRT Staffing and EP Lab Utilization
First-Year Coverage
Income starts with staffing, not just implants. Year one assumes 1 senior electrophysiologist, 1 associate electrophysiologist, 2 cardiac device specialists, 2 nurse practitioners, and 1 remote monitoring technician. That mix supports physician time, device work, monitoring, scheduling, billing, anesthesia support, malpractice, and admin overhead.
Model the Labor Load
To estimate this cost, use headcount × months of coverage × loaded pay for each role. Add anesthesia support, billing, and administrative overhead as separate lines. The key inputs are role count, credentialed coverage hours, and whether the team is built for startup ramp or steady-state volume. One simple rule: if a role touches the implant path, it belongs in the model.
Count each credentialed role separately
Include support labor, too
Model months, not just hires
Use Utilization to Spread Cost
Capacity runs from 550% to 700% by role in year one, then rises toward 850% to 900% in a mature year. Better EP lab utilization spreads fixed payroll over more cases, so margin improves without cutting care. Do not chase savings by understaffing; safe operations need credentialed roles in place.
Fill the schedule before adding overhead
Track cases per staffed day
Avoid uncredentialed shortcuts
Fixed Cost First
Physician time, nurses, device specialists, remote monitoring, anesthesia, scheduling, billing, malpractice, and admin overhead hit income before the first extra case helps. The fastest path to better take-home is higher utilization across the same credentialed team, not thinner staffing. If utilization stays low, the fixed base stays heavy.
CRT Follow-Up and Remote Monitoring
Year-one follow-up
Non-implant revenue matters because it smooths cash between procedures. Here’s the quick math: 56 monthly cardiac device specialist visits at $450, 84 nurse practitioner visits at $350, and 120 remote-monitoring activities at $95 total about $66,000 a month, or $792,000 in year one.
Clean collections
Protect this revenue by matching staff time to visit volume and billing only when documentation and payer rules support it. The key inputs are monthly visits, remote activities, collections per event, and no-show rates; if patient engagement slips, recurring revenue falls before implant volume does.
Track missed-visit leakage
Review payer rules often
Separate monitoring workflows
Recurring lift
By mature year, remote monitoring can reach 1,125 monthly activities at $115 each, or about $129,375 a month. That recurring revenue stays strongest when battery and lead follow-up are built into the workflow, referrals stay steady, and billing stays compliant.
Retention engine
Post-implant visits, device checks, remote monitoring, and battery or lead follow-up create the income base after the implant. If referral retention weakens or staffing cannot keep up, the service loses the very volume that makes this line predictable.
Cardiac Resynchronization Therapy Services Business Plan
30+ Business Plan Pages
Investor/Bank Ready
Pre-Written Business Plan
Customizable in Minutes
Immediate Access
Scenario objective for low, base, and high CRT owner income sensitivity
Owner income scenarios
Owner income changes fast with case count, utilization, and fee mix. Ramp, base, and mature cases show how much take-home can swing before payroll, rent, malpractice, and taxes.
Scenario view of take-home potential across ramp, scale, and mature service levels.
Scenario
Low CaseRamp Case
Base CaseScale Case
High CaseMature Upside
Launch model
This is the lower earnings path with a first-year ramp and tighter case flow.
This is the modeled earnings path with steady scale and normal utilization.
This is the stronger earnings path with mature volume and tighter capacity use.
Typical setup
The model uses 196 implant cases, about $9.383M revenue, a 24.0% listed cost load, and a 76.0% pre-payroll contribution margin.
The model uses 839 implant cases, about $41.385M revenue, a 21.5% listed cost load, and a 78.5% pre-payroll contribution margin.
The model uses 1,890 implant cases, about $97.565M revenue, a 19.5% listed cost load, and an 80.5% pre-payroll contribution margin.
Cost drivers
implant case count
device and lead kits
lab fees
referral outreach
billing fees
case mix
kit cost
lab fees
staffing utilization
billing fees
higher volume
better capacity use
lower kit share
outreach efficiency
billing scale
Owner income rangeBefore owner reserves
$7.13MRamp band
$32.49MCore band
$78.54MMature band
Best fit
Use this to stress-test a slow launch and weaker referral flow.
Use this as the main planning case for a stable operating cadence.
Use this to test mature-service throughput and upside at full scale.
!
Planning note: Scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
The provided data supports a contribution pool, not final owner take-home First-year revenue is $938M, listed cost percentages total 240%, and contribution is about $713M Actual distributions come after payroll, fixed overhead, malpractice, debt service, taxes, reserves, and reinvestment
Break-even timing cannot be calculated from the provided data because fixed payroll, rent, malpractice, equipment debt, and working capital are missing The first-year model has 196 implant cases and $938M in revenue, with a 760% contribution margin before those fixed costs Add monthly overhead to find the case volume needed
No, but facility economics can change owner income a lot A professional-fee-only model may earn less per case than a structure with compliant facility participation The model includes catheterization lab facility fees at 50% of first-year revenue and 40% in the mature year, so site-of-service terms need local review
Implant volume, payer mix, device costs, staffing, lab utilization, and follow-up retention drive most of the income swing In the first year, device and lead kits are 120% of revenue, lab fees are 50%, referral outreach is 30%, and billing fees are 40% A one-point cost shift matters at this revenue level
Start with annual implant cases, then test contribution margin The first-year plan shows about 196 implant cases, $859M of implant-related revenue, and $938M of total revenue including follow-up and monitoring If those cases are delayed, denied, or understaffed, owner distributions can fall even when headline revenue looks strong
About the author
Jack Bennett
Business Model Writer
Jack Bennett is a business model writer at Financial Models Lab, where he explains startup planning and business model economics in clear, practical language. He focuses on the money questions new founders ask when comparing business ideas, with an eye on how small businesses operate day to day. Jack’s writing helps readers understand the numbers behind real business operations without heavy finance jargon, making complex decisions feel more manageable and grounded.
Choosing a selection results in a full page refresh.