7 Factors Influencing Medical Practice Owner Income
Medical Practice Bundle
Factors Influencing Medical Practice Owners’ Income
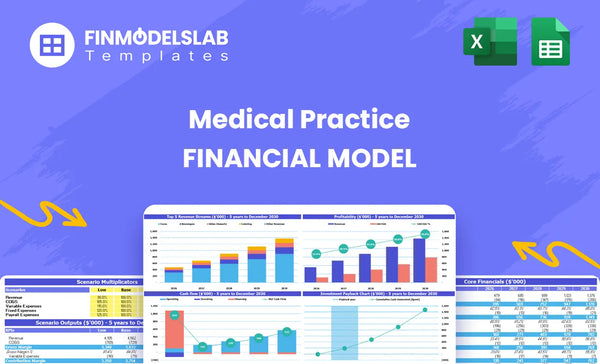
Medical Practice owners see highly variable income, often starting low ($132k EBITDA in Year 1) but scaling rapidly to over $4 million EBITDA by Year 5, driven by capacity utilization and staff expansion Breakeven occurs quickly, in just 2 months, but the minimum cash requirement is substantial at $670,000 This guide breaks down the seven critical financial drivers, focusing on staff productivity, payer mix, and controlling high fixed overhead like the $12,000 monthly rent
7 Factors That Influence Medical Practice Owner’s Income
#
Factor Name
Factor Type
Impact on Owner Income
1
Provider Scaling and Revenue Mix
Revenue
Adding high-revenue staff, like Specialist MDs, directly increases total monthly revenue from the $192,800 baseline.
2
Provider Capacity Utilization
Revenue
Increasing Primary Care MD utilization from 650% toward 850% boosts income because every unused appointment represents lost contribution margin.
3
Service Pricing and Mix
Revenue
Shifting focus to higher Average Treatment Prices, like the $280-$300 Specialist MD rate, improves revenue per patient visit significantly.
4
Variable Cost Control
Cost
Reducing total variable costs from 155% to 105% of revenue by 2030 defintely increases the contribution margin available to the owner.
5
Fixed Overhead Absorption
Cost
Absorbing the $21,700 monthly fixed overhead through high utilization ensures marginal revenue flows straight to the bottom line after break-even.
6
Wage Structure and Staffing Ratio
Cost
Efficiently using lower-paid Medical Assistants to support high-salary Primary Care Physicians maximizes MD efficiency and controls labor costs.
7
Initial Capital Expenditure (CapEx)
Capital
Debt service required for the $303,000 initial CapEx directly reduces owner payout, even when EBITDA is growing well.
Medical Practice Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
What is the realistic owner compensation potential for this Medical Practice?
Owner compensation potential for this Medical Practice is directly proportional to scaling operational capacity, moving from a minimal initial profitability to massive enterprise value capture.
Year 1 Profit Reality
Year 1 EBITDA projection sits at $132,000, setting a defintely low initial benchmark for owner earnings.
To grow beyond this, the practice must aggressively add provider capacity to capture more fee-for-service revenue.
If onboarding takes 14+ days, churn risk rises, slowing down the path to positive cash flow.
Scaling to Owner Wealth
Owner income scales directly with EBITDA growth, targeting $428 million by Year 5.
This requires maximizing practitioner utilization rates across diagnosis and treatment services.
The key lever is scheduling optimization to reduce patient wait times and increase patient throughput.
Owner draw is tied to net profit after reinvestment, so EBITDA is the metric that matters most.
Which operational levers most significantly drive profitability and owner income?
The core profitability driver for your Medical Practice is maximizing the utilization of your high-value providers, specifically aiming for treatment volumes that keep capacity utilization above 85%. If you want to see the startup costs associated with this model, check out How Much Does It Cost To Open And Launch Your Medical Practice Clinic?
Maximize Provider Throughput
Treatments must hit 85% utilization for peak efficiency.
If an MD has 40 billable slots weekly, 85% utilization means 34 treatments.
At a $250 average service price, this yields $8,500 revenue per provider weekly.
Fixed labor costs crush margins if utilization dips below 75%.
Provider Mix Drives Margin
Add specialists delivering higher Average Service Value (ASV).
A specialist might command a $400 ASV versus $150 for routine care.
Hiring more MDs directly scales revenue potential, but only if demand exists.
If onboarding takes 14+ days, churn risk rises defintely among scheduled patients.
How stable are the revenue streams, and what is the risk of high fixed costs?
Revenue stability for your Medical Practice is tied directly to securing reliable payer contracts and ensuring patient volume stays high enough to cover significant overhead, defintely. If patient flow dips, that fixed cost structure bites hard, so you must focus on throughput; Have You Considered The Best Strategies To Launch Your Medical Practice Clinic Successfully?
Revenue Stability Drivers
Fee-for-service revenue depends on treatments delivered daily.
Payer contracts set the reimbursement rate per service.
Volume consistency is the primary stability lever.
Inconsistent scheduling means immediate revenue fluctuation.
Fixed Cost Pressure Point
Monthly rent is a high fixed cost of $12,000.
Provider utilization must exceed 70% to cover overhead.
If utilization falls below 70%, operating losses accumulate fast.
This requires precise scheduling optimization to maintain margin.
What is the minimum capital commitment and time required to achieve cash flow stability?
Projected time to achieve cash payback is 20 months.
The goal is rapid patient acquisition to fund operations.
Drivers of Stability
Stability hinges on practitioner utilization rates.
Revenue comes strictly from fee-for-service treatments.
Watch patient no-show rates; they defintely impact flow.
Capacity management directly translates to monthly cash flow.
Medical Practice Business Plan
30+ Business Plan Pages
Investor/Bank Ready
Pre-Written Business Plan
Customizable in Minutes
Immediate Access
Key Takeaways
Owner income potential scales rapidly from an initial $132,000 EBITDA in Year 1 toward $4 million by Year 5 through strategic provider expansion and utilization growth.
Maximizing provider capacity utilization, ideally exceeding 85%, is the single most critical operational lever for driving profitability and owner compensation.
The business demands a significant minimum cash commitment of $670,000 upfront to cover initial capital expenditures and working capital needs.
High fixed overhead, including substantial rent and insurance costs, creates immediate pressure requiring quick absorption of patient volume to ensure revenue translates directly to profit.
Factor 1
: Provider Scaling and Revenue Mix
Provider Mix Impact
Adding high-revenue Specialist MDs starting in 2028 is the critical step to scale revenue well beyond the $192,800 monthly estimate for 2026. This move changes the revenue mix, trading volume based on lower-tier providers for higher yield per patient encounter. That's how you move the needle.
Capacity Utilization Inputs
To support this scaling, you need to nail provider capacity utilization targets. Initial Primary Care MD utilization is set at 650% in 2026, but profitability requires pushing that toward 850% by 2030. Every unused appointment slot is pure lost contribution margin, so track daily availability closely.
Utilization drives fixed cost absorption.
Unused time means lost revenue potential.
Target utilization must be modeled per provider type.
Optimizing Service Pricing
The revenue jump comes from the Average Treatment Price (ATP) difference between staff tiers. A Specialist MD service runs between $280 and $300, while a Medical Assistant service nets only $60 to $68. Your scheduling system must prioritize filling specialist slots first to maximize revenue per hour.
The planned introduction of Specialist MDs directly attacks revenue ceiling limits. While initial volume might be $192,800 monthly, the ability to bill at the $300 rate versus the $68 rate means revenue scales non-linearly with provider headcount additions post-2028.
Factor 2
: Provider Capacity Utilization
Utilization Drives Profit
Your practice makes money when the Primary Care MDs are seeing patients, not waiting for them. Moving utilization from the initial 650% in 2026 up to the 850% goal for 2030 is the main driver for profit. Every empty slot means you lose the contribution margin from that potential visit. That’s pure lost revenue potential, plain and simple.
Measuring MD Capacity
Estimate MD capacity by tracking scheduled versus available appointment slots daily. You need the total planned MD hours versus actual patient encounter hours logged. This utilization rate directly impacts how fast you absorb the $21,700 monthly fixed overhead, including the $12,000 rent payment. Honestly, utilization is your primary absorption lever.
Total available MD hours per month
Actual patient encounter hours logged
Target utilization percentage (e.g., 850%)
Maximizing MD Time
To push utilization past 650%, you must optimize the MD’s schedule, ensuring Medical Assistants handle lower-cost tasks. Don't let high-salary MDs spend time on administrative work; that kills margin. If onboarding takes 14+ days, churn risk rises and utilization suffers.
Delegate non-MD tasks immediately
Minimize patient no-shows via reminders
Schedule follow-ups proactively
The Cost of Downtime
If you miss the 850% utilization target by 2030, your fixed costs remain a burden. Remember, the Primary Care Physician salary is $220,000 annually; inefficient scheduling means paying top dollar for downtime. You need volume to cover that cost structure, defintely.
Factor 3
: Service Pricing and Mix
Revenue Mix Impact
Revenue per patient visit hinges on service mix, not just volume. Pushing for higher Average Treatment Prices (ATPs) is critical. A Specialist MD visit commanding $280-$300 dramatically outperforms a Medical Assistant service priced between $60-$68. This pricing difference directly impacts the top line fast.
MD Cost Input
Specialist MDs drive the high ATPs, but their input cost is substantial. Their $220,000 annual salary demands high utilization to justify the rate. You need to model the required patient load to cover this fixed wage component while ensuring the $280-$300 service fee generates sufficient contribution margin after variable costs.
MD Annual Salary: $220,000
Target ATP Range: $280 to $300
Utilization Goal: Target 850% capacity
Service Mix Optimization
To improve revenue per visit, aggressively shift scheduling toward Specialist MD services. Avoid letting Medical Assistants handle complex cases that justify the higher rate. If onboarding takes 14+ days, churn risk rises, defintely delaying access to these high-value treatments. Focus on scheduling efficiency to maximize MD time slots.
Prioritize MD slots for complex cases.
Train MAs to handle routine intake tasks.
Track ATP variance daily.
ATP Leverage
The difference between the $60-$68 Medical Assistant rate and the $280-$300 Specialist MD rate is the single biggest lever for immediate revenue improvement. Every visit shifted from the low end to the high end multiplies the financial impact across the entire patient base.
Factor 4
: Variable Cost Control
Variable Cost Leverage
Your initial variable costs are unsustainable at 155% of revenue, driven by high COGS and OpEx. Scaling volume allows you to cut billing fees from 60% to 50%, dropping total variable costs toward a manageable 105% by 2030, which is critical for margin improvement.
Initial Cost Structure
The starting variable cost load is 155% of revenue, split between 65% COGS (supplies, pharmaceuticals) and 90% variable OpEx (transaction fees, direct billing costs). If you generate $100 in revenue, you spend $155 just covering these direct costs. Honsetly, this structure means you are losing money on every treatment until scale hits.
Calculate direct labor allocation per service line.
Cutting Variable Drag
The primary lever to improve contribution margin is negotiating or switching payment processors to reduce the 60% billing fee component of OpEx. Reducing this fee to 50% directly flows to the bottom line as volume increases. If you hit 105% total VC by 2030, your margin profile changes significantly.
Bundle low-cost services to improve utilization efficiency.
Ensure Medical Assistants handle intake to reduce MD time costs.
Margin Impact
Because fixed overhead is high at $21,700 monthly, every percentage point you cut from variable costs accelerates hitting profitability. If billing fees stay stuck at 60%, you will struggle to absorb rent and insurance costs, even with good utilization numbers.
Factor 5
: Fixed Overhead Absorption
Absorbing Fixed Costs
Your $21,700 monthly fixed costs require high utilization to cover rent and insurance. Once you pass break-even, every dollar of marginal revenue flows directly to profit because fixed costs are already covered. This structure means utilization is the single biggest driver of owner income.
Fixed Cost Components
This $21,700 monthly fixed overhead is largely composed of facility and compliance costs. The $12,000 rent payment and $2,500 for malpractice insurance are sunk costs that don't change if you see 10 or 100 patients. You need utilization data to calculate the fixed cost per visit, defintely.
Rent: $12,000 monthly
Insurance: $2,500 monthly
Other overhead: $7,200
Driving Cost Absorption
You can't easily cut rent, so managing this overhead means maximizing revenue generation per hour. The goal is hitting utilization targets, like the 850% target for Primary Care MDs by 2030, to spread that $21,700 burden thinly. Every service delivered above break-even is pure margin.
Focus on MD utilization rates
Prioritize high ATP services
Avoid adding fixed staff too early
Profit Leverage Point
Because fixed costs are high, profitability scales aggressively once you cover the $21,700 hurdle. If your contribution margin is 40% after variable costs, every dollar of revenue above the break-even point adds 40 cents directly to operating profit. This leverage is why utilization matters so much.
Factor 6
: Wage Structure and Staffing Ratio
Staff Cost Leverage
Your Primary Care Physician salary clocks in at $220,000 annually, making staff efficiency critical. You must structure roles so Medical Assistants, earning only $45,000, handle routine work to keep the MD focused on high-value diagnosis. That ratio is your main lever.
PCP Cost Input
The PCP wage is a major fixed labor cost that must be justified by patient throughput. This estimate relies on the $220,000 annual salary figure, which translates to about $18,333 monthly before benefits. If utilization lags, this high fixed cost eats margin fast. You need to know the exact tasks transferred to MAs.
MA Efficiency Gains
To optimize, clearly define the scope of work for the $45,000 MA role. They should manage intake, vitals, and follow-up scheduling—tasks that don't require an MD license. If an MA can handle 30% of the typical MD workflow, you effectively increase the MD's capacity without hiring another $220k provider.
Ratio Management
Managing the staff-to-patient ratio isn't just about headcount; it's about revenue protection. Every minute an MD spends on paperwork that an MA could do costs you thousands annually in opportunity loss. Defintely track MD time allocation weekly.
Factor 7
: Initial Capital Expenditure (CapEx)
CapEx Debt Drain
The $303,000 initial capital expenditure for the medical practice build-out is a significant hurdle. Debt payments required to finance this investment will directly cut into the cash available for owners, even if the clinic generates solid operating profits (EBITDA).
CapEx Cost Inputs
This $303,000 covers the physical setup and necessary tools for the practice. Think about leasehold improvements, like exam room construction, plus medical devices such as diagnostic tools and electronic health record systems. This large upfront spend must be covered by equity or debt before the first patient visit. Here’s the quick math on what drives this number:
Leasehold improvement quotes.
Equipment procurement costs.
Permitting and compliance fees.
Managing Build Costs
You can manage this large fixed cost by phasing the facility opening or negotiating equipment financing instead of outright purchase. Avoid over-specifying non-essential office finishes; focus capital strictly on clinical functionality. A common mistake is assuming all equipment must be purchased new; used, certified diagnostic gear saves cash. If you manage this well, you defintely lower the initial debt load.
Phase build-out over 18 months.
Lease high-cost imaging gear.
Negotiate tenant improvement allowances.
Payout Barrier
Servicing the debt taken on for the $303,000 investment means that every dollar used for principal and interest payments is a dollar not paid to the owners. Even if monthly EBITDA grows strongly, high required debt service acts as a mandatory fixed drain, delaying the return on invested capital for the founders.
Owner earnings vary widely, starting around $132,000 EBITDA in Year 1 and scaling rapidly to over $42 million by Year 5, depending on staff count and utilization rates;
This model suggests a very fast breakeven in just 2 months, but requires a significant upfront cash investment of $670,000 to cover initial CapEx and working capital;
Maximizing provider capacity is key; moving a Primary Care MD from 65% utilization to 85% utilization creates substantial marginal revenue that converts directly to profit due to high fixed overhead
Initial capital expenditures total $303,000 for equipment and build-out, plus working capital, leading to a minimum cash requirement of $670,000;
Average prices range significantly, from $60 for Medical Assistant services up to $280-$300 for Specialist MD treatments, emphasizing the need for a high-value service mix;
Yes, efficient staffing, where lower-cost staff like NPs ($110k salary) and MAs ($45k salary) support higher-cost MDs ($220k salary), is essential for margin preservation
Choosing a selection results in a full page refresh.