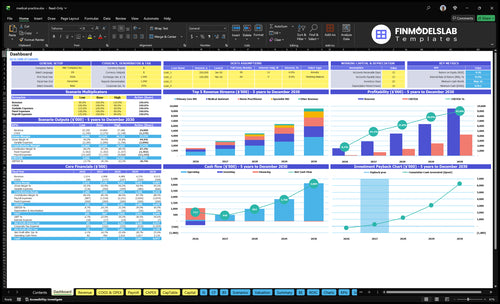
How Much Does a Medical Practice Owner Make? $151M Year 1 Model
Medical Practice Bundle
A US medical practice owner can make clinical salary plus profit distributions, but revenue is not take-home pay In the first year, modeled collections are $151M from 1,214 monthly visits after 155% variable costs, $2604k fixed overhead, and $550k of provided physician and nurse practitioner payroll, the pre-tax profit pool is about $469k If the owner is one paid primary care physician, total pre-tax take-home could reach about $689k before debt, reserves, taxes, reinvestment, and wage lines not provided By the mature year, modeled collections reach $951M, so utilization and staffing discipline drive the upside
Owner income$132k–$4.3MNet margin5.7%–38.2%Revenue for target pay$2.3M–$11.2MBusiness difficultyHard
Want to test your own clinic income case?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, staffing, overhead, reserves, and owner pay target. Use monthly patient collections by folding visits, reimbursement, and collection rate into revenue.
!
Planning note: This is a researched planning estimate, not guaranteed salary, tax advice, or owner distribution advice.
How does adding providers affect medical practice owner income?
Adding providers can raise Medical Practice owner income, but only if utilization, reimbursement, billing, and rooms scale with headcount. In this model, staffing grows from 2 primary care physicians and 1 nurse practitioner in year 1 to 6 primary care physicians, 4 nurse practitioners, 2 specialist physicians, and 2 behavioral health providers in the mature year, while collections rise from $151M to $951M. The catch is simple: added payroll, supervision, compliance, working capital, and management time can absorb profit if capacity stays tight.
Revenue grows only with capacity
More providers can lift collections
$151M to $951M is the scale path
Visits must stay booked
Rooms and billing must keep up
Profit gets pressured fast
Payroll rises with each hire
Supervision and compliance add cost
Working capital needs increase
Management time becomes a real expense
How much revenue does a medical practice need to pay the owner?
If you want the owner paid, start with the pay target and then gross up for the full cost stack. In this Medical Practice model, $1.51M in collections, 15% variable costs, $260.4k fixed overhead, and $550k in physician and nurse practitioner payroll leave about $469k before taxes, debt, reserves, and reinvestment. The real revenue target moves with specialty mix, reimbursement per visit, capacity, staffing, and fixed costs.
Cost stack first
$1.51M collections
15% variable costs
$260.4k overhead
$550k provider payroll
Revenue drivers
Specialty mix changes rate
Visit volume drives cash
Capacity caps collections
Staffing shifts break-even
Do private practice owners make more than employed doctors?
Yes, Medical Practice owners can make more than employed doctors, but only after collections cover payroll, staffing, rent, malpractice insurance, billing, debt, reserves, and reinvestment; start with What Is The Main Goal You Aim To Achieve With Your Medical Practice? because the first-year model shows a $469k pre-tax profit pool after provider payroll, plus a possible $220k clinical salary if the owner also works as a paid primary care physician.
Upside Math
$469k pre-tax profit pool
$220k possible clinical salary
Profit comes after provider payroll
Collections must clear overhead first
Owner Risk
Payer delays strain cash reserves
Hiring pressure cuts owner margin
Management time reduces clinic time
Debt and reinvestment come first
Medical Practice Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
Want to see the six income drivers?
1
Collected Revenue
$1.4M
At about $1.4M in first-year collections, every extra visit and better collection rate feeds the owner pool before costs hit.
2
Visit Volume
1.05K/mo
About 1.05K monthly visits set the ceiling, so higher fill rates and fewer empty slots raise income fast.
3
Provider Payroll
$768K
Year-one payroll runs about $768K, so each added clinician or assistant must lift collected revenue more than it costs.
4
Payer Mix
$60-$300
Service prices range from $60 to $300, and a better mix of higher-value care lifts average reimbursement without more rooms.
5
Overhead Load
$21.7K/mo
Fixed overhead is about $21.7K a month, so rent, insurance, software, and admin discipline protect margin.
6
Owner Draw
$469K
The $469K pre-tax pool only becomes take-home if the owner keeps reinvestment tight and avoids overstaffing.
Medical Practice Core Six Income Drivers
Collected Revenue Per Provider
Collected Revenue Per Provider
Collected revenue per provider is the cash that actually lands, not billed charges. In this model, first-year collections are $151M, built from $160 primary care physician visits, $130 nurse practitioner visits, and $60 medical assistant visits at stated utilization.
That matters because owner pay comes from what is collected after payroll and fixed costs. By mature year, collections reach $951M as provider count, visit volume, pricing, and capacity rise. If coding accuracy, reimbursement rates, or collection rate slip, cash flow falls even when schedules look full.
Track cash, not charges
Measure collections by provider type and payer mix each month. Here’s the quick math: visits × reimbursement × collection rate, adjusted for service mix. The owner should watch denials, under-coding, and delayed payment first, because those cut profit before staffing or rent can move.
Track collections by visit type
Compare paid vs billed amounts
Test coding accuracy each month
Forecast mix shifts before hiring
1
Patient Volume And Provider Utilization
Visit Volume and Provider Utilization
Patient volume and provider utilization decide how much of the schedule turns into cash. The model moves from 1,214 monthly visits in year one to 5,942 monthly visits in the mature year, about 4.9x more. Utilization rises from 65% to 85% for primary care physicians, 60% to 83% for nurse practitioners, and 70% to 90% for medical assistants, so empty slots and room limits cut income.
This driver includes scheduled visits, kept visits, room capacity, and staffed hours. If demand is there but patients no-show, rooms back up, or support staff are short, collections miss the plan and owner pay falls with them. More booked visits only help when the clinic can actually deliver and bill them.
Protect the Kept-Visit Rate
Track booked visits, kept visits, no-show rate, room count, and provider hours by role. The gap between scheduled and completed visits is the leakage that lowers revenue and cash flow, even when the calendar looks full. Use the year-one baseline of 1,214 monthly visits and the mature target of 5,942 to forecast staffing and owner draws.
Measure kept visits by provider.
Set room limits by peak hour.
Review no-shows weekly.
Match staffing to utilization targets.
When utilization lifts toward 85%, 83%, and 90%, more of each fixed month turns into profit, but only if scheduling stays tight and rooms do not sit empty. If the clinic grows volume before flow is stable, the extra visits can disappear into missed appointments and underused staff time.
2
Payer Mix And Reimbursement
Payer Mix and Reimbursement per Visit
Reimbursement per visit is the cash you collect, not the charge you bill. This model starts at $160 for primary care physician visits, $130 for nurse practitioner visits, and $60 for medical assistant visits, then rises to $300 for specialist physician visits and $220 for behavioral health visits in the mature year. Commercial pay usually supports higher collections than Medicare, Medicaid, self-pay, or cash-pay.
Here’s the quick math: if visit volume stays flat but reimbursement drops 10%, collected revenue drops about 10% too. That hits gross margin first, then cash for payroll, rent, and owner pay. The key inputs are payer mix, service mix, coding accuracy, and collection rate. A lower-yield mix can shrink take-home even when the schedule looks full.
Track Yield by Payer and Visit Type
Measure collected dollars per visit each month by payer and provider type. Compare actual collections with the model rates, and split out commercial, Medicare, Medicaid, self-pay, and cash-pay. That shows whether low-yield visits, denials, or write-offs are cutting owner income.
Track collections per visit.
Review payer mix monthly.
Check denial rates fast.
Test contracts before scaling.
If specialist and behavioral health visits reach $300 and $220, protect those rates with clean coding and quick claim follow-up. If collections slip, trim forecasted owner draws before cash gets tight.
3
Staffing And Provider Payroll
Provider Payroll
$550k in first-year payroll, built from 2 primary care physicians at $220k each and 1 nurse practitioner at $110k, is a fixed cost that only works if visits are filled and collected. Payroll creates capacity, but empty schedule slots turn it into a cash drain. The real test is whether added clinicians lift collected revenue faster than wage cost.
By the mature year, staffing rises to 6 primary care physicians and 4 nurse practitioners, plus specialists and behavioral health providers in the operating plan. That can grow income, but only if billing, coding, and room flow keep pace. If cost control cuts too deep, care quality, compliance, and patient experience slip, and owner take-home falls with them.
Track Payroll Payback
Measure payroll per collected visit, provider utilization, and collections by role each month. Use the schedule to test whether each added clinician brings in enough billed, collected visits to cover salary before you hire again.
Track collected visits by provider.
Watch no-shows and open slots.
Check coding and denial rates.
Protect billing, compliance, and care quality.
Here’s the quick math: if payroll rises before utilization does, margin shrinks fast. Add staff only when scheduling, room capacity, and payer mix can support the higher wage load and still leave cash for owner pay.
4
Fixed Overhead And Regulated Costs
Fixed Overhead Pressure
This line is the cash floor the practice must cover before the owner sees a draw. Monthly fixed overhead is $217k: $12k rent, $25k malpractice insurance, $2k software, $15k utilities, $1k fixed marketing, $800 general liability insurance, $700 supplies, and $12k cleaning.
Annualized, that is $2.604M, or about 1.7% of the modeled $151M first-year collections. What this estimate hides is timing: if collections lag, the owner still pays the fixed bills first, so cash can tighten even when profit looks fine on paper.
Protect the Non-Negotiables
Track each fixed line monthly and flag any step-up over 5%. The inputs are simple: lease, premium notices, software fees, utility bills, cleaning contract, and marketing retainer. Don’t cut malpractice, general liability, or cleaning just to improve margin; those costs support compliance, risk control, and clinical quality.
Review fixed costs every month.
Separate safe cuts from protected costs.
Check cash before owner draws.
A $10k monthly cut adds the same $10k to pre-tax owner cash, but only if service quality and billing stay intact.
5
Owner Role, Reserves, And Debt
Owner Pay Mix
Owner income changes with role: clinician, manager, or investor. The first-year profit pool is about $469k before taxes, reserves, debt, reinvestment, and any missing wage lines. If the owner also works as one paid primary care physician, add a $220k clinical salary. So the key question is whether pay comes from salary, distributions, or both.
Accounting profit is not the same as cash in the owner’s pocket. Debt service, reserve targets, and new hires can cut take-home even when the practice looks profitable on paper.
Track Cash Before Owner Draw
Build the owner forecast from three lines: clinical pay, management pay, and distributable profit. Then subtract debt payments and the reserve amount you want to keep in the bank. That shows what the owner can safely take home without starving the practice.
$469k profit pool
$220k physician salary
Debt service and reserves
Management wages, if hired
If the owner manages the practice instead of hiring management, cash stays higher; if the owner hires management, take-home drops but time opens up for patient care or growth.
6
Medical Practice Business Plan
30+ Business Plan Pages
Investor/Bank Ready
Pre-Written Business Plan
Customizable in Minutes
Immediate Access
Compare lean, base, and mature medical practice income scenarios
Owner income scenarios
Owner income scales with provider count, visit volume, and billing efficiency. Fixed overhead is high from day one, so early cash is tight until utilization improves.
Low, base, and high cases show how staffing and volume change owner take-home potential.
Scenario
Low CaseLow Case
Base CaseBase Case
High CaseHigh Case
Launch model
Owner income stays modest while the clinic is still ramping and collections are limited.
Owner income reflects a mid-ramp clinic with stronger utilization and a broader provider mix.
Owner income peaks when the clinic reaches mature volume and a full multi-provider schedule.
Typical setup
Owner stays hands-on in Year 1, with 2 primary care MDs, 1 nurse practitioner, 2 medical assistants, no specialist or behavioral health, and heavy fixed overhead on a small collections base.
Owner shifts toward oversight in Year 3, with 4 primary care MDs, 2 nurse practitioners, 4 medical assistants, 1 specialist MD, and 1 behavioral health clinician, plus better collections spread over fixed costs.
Owner runs a larger platform in Year 5, with 6 primary care MDs, 4 nurse practitioners, 6 medical assistants, 2 specialist MDs, and 2 behavioral health clinicians, so fixed costs are spread across more visits but payroll is much larger.
Cost drivers
provider payroll
billing and collections fees
rent and utilities
medical supplies and lab fees
patient acquisition
provider payroll
billing and collections fees
specialist and behavioral staffing
rent and software
referral spend
provider payroll
billing and collections fees
specialist and behavioral staffing
rent and maintenance
supply and diagnostic spend
Owner income rangeBefore owner reserves
$132kLow Case
$1.391MBase Case
$4.279MHigh Case
Best fit
Use this to test whether launch cash and reserves can hold if ramp is slow or collections lag.
Use this as the working plan if you expect steady growth and a realistic owner draw path.
Use this to test upside if recruiting, utilization, and collections all run well, while debt service still needs coverage.
!
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
A medical practice owner can make clinical salary plus distributions, but only after expenses In the first-year model, collections are $151M and the pre-tax profit pool is about $469k after provided payroll, variable costs, and fixed overhead If the owner is one paid primary care physician, add $220k before taxes, debt, reserves, and reinvestment
Owner income usually stabilizes after utilization, billing, and staffing settle This model ramps from 1,214 monthly visits in the first year to 5,942 monthly visits in the mature year That growth depends on provider hiring, schedule fill, reimbursement timing, and cash reserves If onboarding or credentialing slows collections, owner distributions should stay conservative
You need enough collected revenue, not just billed charges The first-year model shows $151M in collections, 155% variable costs, and $217k monthly fixed overhead High revenue can still produce weak take-home if payroll, billing leakage, rent, malpractice insurance, debt service, or reinvestment consume the margin
The biggest drivers are collections per provider, visit utilization, reimbursement per visit, payroll, fixed overhead, and reserve policy In this model, primary care physician utilization rises from 65% to 85% over the period, while mature-year collections reach $951M Small changes in reimbursement or staffing can move owner income fast
Build owner pay from cash flow, not hope Start with monthly visits, reimbursement, collection rate, staffing, rent, malpractice insurance, billing fees, debt, and reserves Then split owner compensation into clinical salary, management pay, distributions, and retained cash The first-year model’s $469k pre-tax profit pool is not automatically distributable
About the author
Patrick Hughes
Small Business Writer
Patrick Hughes is a small business writer who focuses on business affordability analysis for side-hustle builders planning with limited capital. He researches how small businesses launch, operate, and earn money, with a practical eye on business idea evaluation. His writing highlights common costs new founders often miss, helping readers make clearer, more realistic decisions before they start.
Choosing a selection results in a full page refresh.