Stem Cell Therapy Clinic Owner Income: $18M Year 1 Model
Stem Cell Therapy Clinic
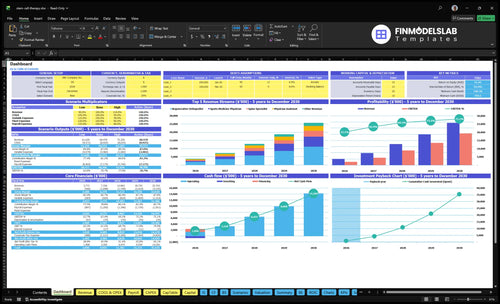
A stem cell therapy clinic owner can make meaningful pre-tax income, but revenue is not owner pay Using the researched first-year assumptions, the clinic completes about 162 monthly treatment lines, collects about $314k per month, and generates about $177M in annual operating cash flow after listed payroll, supplies, marketing, and overhead That equals a modeled operating margin of about 470% before taxes, debt service, reserves, reinvestment, and owner distributions If the owner also serves as the Medical Director, the modeled $320k annual Medical Director salary is a separate compensation line already included in payroll
Owner income$2.62MNet margin69.4%Revenue for target pay$3.77MBusiness difficultyHard
Want to test your owner pay target?
Owner income calculator
Estimate monthly owner take-home from revenue, gross margin, payroll, overhead, reserves, and a target pay goal.
!
Planning note This is a researched planning estimate, not guaranteed income, tax advice, legal advice, clinical efficacy claims, or owner distribution advice.
How does the clinic model turn capacity into owner income?
Open the Stem Cell Therapy Clinic Financial Model Template to see how provider capacity becomes owner income. It covers dashboard, revenue assumptions, treatment mix, staffing, wages, direct costs, fixed overhead, marketing, cash flow, owner income, and scenario testing. First-year output: $377M revenue, $177M operating cash flow, 470% margin, $819k payroll, $3,324k fixed overhead, and 225% variable cost load.
Owner-income model highlights
Owner take-home is explicit
$377M revenue, 470% margin
Scenarios test capacity swings
How does physician owner stem cell therapy clinic income differ?
For a Stem Cell Therapy Clinic, owner income is usually highest when the physician-owner actually fills the Medical Director role, because the $320k can be part of owner pay. If the owner hires that role, the clinic has to earn enough to cover that salary before any distributions. Here’s the quick math: the first-year team cost is $819k for the Medical Director, manager, coordinator, two RNs, two MAs, and two front desk staff. Ownership and scope rules are state-sensitive, so this is cost planning, not legal advice.
Physician-owner model
$320k can be owner pay
Distributions still need cash flow
Lower payroll pressure, better margin
Scope rules still matter by state
Hire-and-manage model
Medical Director salary becomes overhead
First-year staffing totals $819k
Management team adds fixed cost
Owner income depends on volume
How many stem cell treatments per month to pay the owner?
About 81 treatment lines a month are needed to pay the owner $25,000 monthly after variable costs, payroll, fixed overhead, and reserves. The clinic’s first-year weighted average collected revenue is $1,943 per treatment line, and contribution is about $1,506 after 22.5% direct and variable costs. Here’s the quick math: $95,950 of payroll plus fixed overhead breaks even at about 64 lines per month, and the model’s 162-line base case leaves room only if utilization and collections hold.
Payowner math
64 lines covers overhead.
81 lines funds owner pay.
$1,506 contribution per line.
$1,943 collected per line.
What to watch
Keep utilization near 162 lines.
Protect collections on every case.
Watch payroll and fixed overhead.
Reserve cash before owner draws.
What is the stem cell therapy clinic profit margin?
If you’re pricing a Stem Cell Therapy Clinic, the model shows a first-year operating margin of about 470%, with $177M operating cash flow on $377M revenue. The gross contribution margin is 775% before $819k payroll and $3,324k fixed overhead, and it reaches 757% in the scaled fifth year; see What 5 KPIs Matter For Stem Cell Therapy Clinic? for the KPI set. Keep gross margin separate from net operating income and owner distributions.
Margin drivers
120% biologic kits
30% lab processing
60% patient acquisition marketing
15% clinical supplies
Scale effect
Utilization rises in later years
Cost percentages fall over time
757% fifth-year operating margin
Separate margin from owner draws
Stem Cell Therapy Clinic Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
Want the six levers that move owner income most?
1
Patient Demand
162/mo
More qualified patients fill the schedule and support the jump from $3.8M in year 1 to $25.8M by year 5.
2
Consult Conversion
Compounding
Better consult-to-treatment conversion turns the same lead flow into more paid procedures, so income rises without matching cost.
3
Collected Price
$1,943
The $1,943 weighted average collected revenue per treatment is the cleanest price lever, and small gains lift every case.
4
Provider Capacity
$95.9K/mo
With $95,950 a month in payroll and fixed overhead, room use and provider mix decide how much revenue reaches the owner.
5
Procedure Costs
225%
A 225% variable cost load cuts contribution hard, so kit, lab, and supply discipline protect take-home.
6
Overhead Efficiency
470%
Keeping acquisition spend and fixed overhead tight is what makes the model's 470% operating margin hold.
Stem Cell Therapy Clinic Core Six Income Drivers
Qualified patient demand
Qualified demand
Demand sets the top of the funnel, but qualified demand is what pays the bills. If year one needs 162 completed monthly treatment lines, weak lead quality leaves provider time idle and pushes break-even out. Track consult volume, referral share, local search, and paid inquiry cost against medically suitable candidates.
Track the funnel
Use five inputs: monthly consult volume, lead source mix, referral share, local search volume, and paid inquiry cost. The key filter is not raw leads; it’s how many patients are medically suitable and ready to complete a plan. Here’s the quick math: more consults only help if qualification and conversion hold.
Protect capacity
Orthopedic referrals, sports injury networks, and strong local search visibility usually improve fit and shorten the path to treatment. Paying for leads that do not qualify or do not convert raises acquisition cost and can hurt reputation. Better demand quality lifts utilization first, so you can delay adding fixed overhead until the schedule stays full.
Qualified mix
What this estimate hides is the spread between inquiries and completed lines. A clinic can look busy on paper and still miss the 162-line target if the source mix is weak. The practical move is to favor referral and local search channels that bring medically suitable patients, then watch paid inquiry cost against completed treatment lines.
Consult-to-treatment conversion
Consults must convert
Revenue starts when a consult turns into a collected plan. Track consult-to-treatment conversion rate, show rate, financing approval rate, treatment plan acceptance, and time from consult to procedure. If those steps slip, marketing spend buys fewer paid treatments, even when lead volume looks healthy.
Track the funnel
Here’s the quick math: every consult has to move through the funnel before cash shows up. Use the numbers below to spot where demand is leaking.
Show rate for kept visits
Acceptance for plan sign-off
Approval for financed plans
Days to procedure for speed
Lift acceptance
Improve conversion with clear pricing, physician trust, patient education, documented screening, and clean scheduling. That keeps the consult honest and easier to accept. Avoid pressure-based selling or unsupported claims; those tactics can hurt trust and raise waste instead of raising collected revenue.
What the model says
The model output of 162 monthly treatment lines depends on both patient demand and acceptance, not staffing alone. Tightening conversion usually lifts revenue per marketing dollar and cuts patient acquisition waste, because more consults become paid treatment plans instead of ending at the first visit.
Average collected revenue per treatment plan
Collected revenue
Owner income tracks cash collected, not the sticker price. In year one, the weighted average collected revenue is $1,943 per treatment line, based on $314,325 monthly revenue divided by 16,175 treatment lines. That range runs from $200 physical therapy visits to $8,500 spine specialist procedures, so mix matters more than volume alone.
Billed vs. cash
Build the model from billed price, collection rate, bundled visits, follow-up care, and refund policy. A $5,000 treatment plan can land much lower in cash if discounts, denials, or refunds hit. One clean rule: separate list price from collected dollars on every service line.
Price by condition
Track collection rate
Reserve for refunds
What lifts income
The near-term lift comes from higher collected price per plan, not more patients first. Focus on procedures with higher complexity, cleaner payment terms, and tighter follow-up packaging. If collections hold, each pricing step-up flows straight into revenue and owner pay, but weak collection controls erase that gain fast.
Cash lift
For planning, treat this as a revenue lever, not a guarantee. With 16,175 treatment lines in year one, even small changes in collected price move monthly cash fast; the risk is assuming list price equals collected cash. That mistake overstates profit and leaves the owner short on reserves.
Clinical capacity and provider cost
Capacity
Income starts with clinic capacity. This plan uses 2 regenerative orthopedists, 1 sports medicine physician, 1 spine specialist, 2 physician assistants, and 2 physical therapists. Utilization runs from 350% to 600%, so the schedule has to stay full. If slots sit open, revenue stalls; if they fill, the same base can carry more procedures.
Payroll
Clinical payroll support totals $819k a year, including a $320k Medical Director. Estimate it as headcount times pay, plus leadership fees and support roles. This is a major startup line, so the real test is how many completed procedures each provider can support before payroll outruns collections.
Hiring
Don’t hire ahead of demand. Watch provider utilization, completed procedures per provider, clinical support ratio, and schedule fill rate each month. The clean move is adding capacity only when calendars stay full, so margin expands before fixed costs jump. One thin schedule can waste a lot of payroll.
Watchpoints
Here’s the quick math: the $819k payroll base gets easier to carry only when those 350% to 600% provider hours turn into filled procedure slots. If schedule fill rate slips, capacity becomes idle cost fast. If it stays high, added capacity can lift margin without waiting for a big fixed-cost reset.
Direct procedure cost
Cost load
Direct procedure cost hits gross profit before overhead. In year one, the modeled direct and variable load is 225% of revenue: 120% biologic procedure kits, 30% laboratory processing, 60% patient acquisition marketing, and 15% clinical medical supplies. So every $100 collected carries $225 of direct and variable cost pressure.
What it covers
Build this from case inputs, not a clinic average. Include biologics, kits, sterile supplies, lab or processing fees, imaging support, and waste. Estimate it with units × unit price, outside lab quotes, per-case imaging fees, and a waste rate. This sits inside gross margin, so it must be tied to each treatment line.
Count cost per treatment line.
Use vendor quotes per case.
Separate simple and complex care.
Keep it in line
Control it with case-level tracking, not broad averages. Watch cost per treatment line and gross contribution by treatment type. The main leak is waste, rework, or underpriced complex care. If supply use and pricing stay aligned, contribution margin improves; if they drift, the clinic can be busy and still lose money on each completed procedure.
Margin signal
Price the full case before treatment and compare it to actual kit, lab, and supply use after the case closes. If a complex case needs more waste or imaging support, the price has to cover it up front, or owner take-home gets squeezed fast.
Marketing efficiency and fixed overhead
Fixed overhead
First-year fixed overhead is $27,700/month. The biggest piece is the $15,000 lease, then $4,500 malpractice insurance, $2,200 EHR (electronic health record) and IT, $3,000 utilities and maintenance, $1,200 admin office costs, and $1,800 compliance and accreditation. Rent alone is 54% of fixed overhead, so space cost matters fast.
Marketing drag
Patient acquisition marketing is 60% of first-year revenue, so the top line gets hit hard before the clinic feels stable. Track customer acquisition cost (CAC), booked consult cost, and referral share together; a cheap lead that never books still burns cash. One clean read: every $1 of revenue leaves only $0.40 before other operating costs.
Protect cash
Do not underfund malpractice, compliance, or patient-safety operations. The protection bucket here is $8,500/month across insurance, EHR and IT, and compliance, so cutting it to save cash can backfire. Watch rent as a percentage of revenue, payroll load, and cash reserves; sustainable owner take-home comes after those are covered.
Owner cash first
Overhead discipline decides how much contribution turns into owner cash, and the first-year load is already heavy at $27,700/month fixed plus 60% of revenue spent on marketing. The clinic has to keep enough cash for referrals, payroll load, and reserves before any owner draw.
Stem Cell Therapy Clinic Business Plan
30+ Business Plan Pages
Investor/Bank Ready
Pre-Written Business Plan
Customizable in Minutes
Immediate Access
Compare low, base, and high owner-income scenarios
Owner income scenarios
Owner cash moves with utilization. Faster patient volume helps, but payroll, marketing, compliance, and facility costs can still outrun revenue if ramp stalls.
Low, base, and high cases show how throughput changes owner cash.
Scenario
Low CaseRamp
Base CaseScaled
High CaseCapacity-heavy
Launch model
This is the slower owner-cash path if the clinic stays in first-year ramp mode and utilization rises unevenly.
This is the modeled middle path once the clinic reaches steady, midscale throughput.
This is the stronger path when the clinic runs near peak capacity and keeps adding volume.
Typical setup
About 162 monthly treatment lines, about $3.772M year 1 revenue, and about $1.8M operating cash before taxes, debt, reserves, and distributions.
About 562 monthly treatment lines, about $12.862M year 3 revenue, and about $8.9M operating cash as the clinic adds staff and uses more capacity.
About 1,051 monthly treatment lines, about $25.763M year 5 revenue, and about $19.4M operating cash at a fuller schedule.
Cost drivers
Slow patient ramp
heavy facility lease
fixed clinical payroll
marketing spend
compliance overhead
Midscale utilization
staffing growth
patient acquisition marketing
lab and supply costs
compliance load
Near-full capacity
higher staffing needs
larger marketing reach
more compliance work
facility load
Owner income rangeBefore owner reserves
$1.8MRamp case
$8.9MScaled case
$19.4MPeak case
Best fit
Use this to stress-test opening-year throughput and fixed-cost pressure.
Use this as the core operating plan for a growing clinic with stable demand.
Use this to test upside when volume stays high and fixed costs do not outrun utilization.
!
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
In the researched first-year model, the clinic generates about $177M in operating cash flow before taxes, debt service, reserves, reinvestment, and owner distributions That comes from $377M in annual revenue, 162 monthly treatment lines, and a 470% operating margin after listed payroll, direct costs, marketing, and overhead
Profitability depends on utilization, not just opening the doors In this model, first-year break-even before owner pay is about 64 monthly treatment lines, using $1,943 average collected revenue and about $1,506 contribution per treatment line The model assumes 162 monthly treatment lines, but slower demand or longer onboarding would delay cash flow
Not always, but the owner role changes the economics and may affect structure This model includes a $320k Medical Director salary as an operating cost If the owner fills that role, compensation may include that salary plus distributions If the role is hired, the clinic must cover the cost before owner take-home
The biggest profit drivers are qualified demand, consult conversion, collected treatment price, provider utilization, direct procedure cost, and overhead discipline First-year variable costs equal 225% of revenue, payroll is $819k annually, and fixed overhead is $3324k annually Small changes in capacity fill or marketing efficiency can materially change owner cash
Protect owner income by funding compliance, insurance, staffing, and cash reserves before taking aggressive distributions In the first-year model, malpractice insurance is $4,500 per month, compliance and accreditation is $1,800 per month, and payroll is $68,250 per month Underfunding these areas may create operational risk even when revenue looks strong
About the author
Philip Stone
Business Model Writer
Philip Stone is a business model writer at Financial Models Lab, focused on the economics behind day-to-day business operations. He explains startup planning in plain language, helping aspiring small business owners think through the money questions new founders ask. With a clear, grounded approach, he helps readers compare business opportunities realistically and choose ideas that fit their goals without getting lost in heavy finance jargon.
Choosing a selection results in a full page refresh.