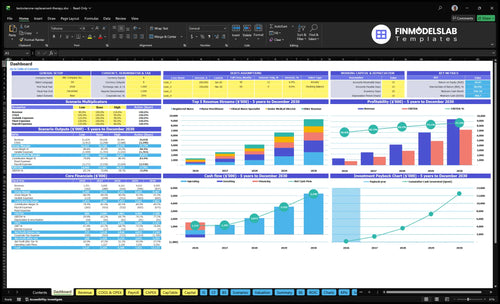
A Testosterone Replacement Therapy Clinic can show very high margin on paper, but the real profit answer depends on payroll, lab costs, and how fast cash comes in. In the model, listed COGS and variable expenses are 205% of revenue in Year 1 and 155% by Year 5, while even after $183k in monthly fixed overhead, pre-payroll operating margin is 633% in Year 1 and 821% in Year 5; for the cost side, see What Are Operating Costs For Testosterone Replacement Therapy Clinic?. That is not final profit, because provider payroll and reserves are not included.
What moves margin
Lab billing can swing results fast.
Medication and supplies cost matter most.
Claim timing changes cash flow.
Patient affordability drives volume.
What to watch
Cash-pay usually collects cleaner.
Insurance adds denials and admin work.
Marketing efficiency affects payback.
Provider payroll still changes true profit.
How much can a TRT clinic owner take home after expenses?
A Testosterone Replacement Therapy Clinic owner can’t treat collections or EBITDA as take-home pay; the source model shows $135M Year 1 revenue and $8.546M pre-payroll operating profit after listed costs, but that pool still pays providers, medical director fees, taxes, debt, and reserves; see What Are Operating Costs For Testosterone Replacement Therapy Clinic? for the cost base. By Year 5, the source case reaches $930M revenue and $764M pre-payroll operating profit, but the owner should not withdraw all of it.
Take-home ceiling
$8.546M Year 1 pre-payroll pool
$764M Year 5 pre-payroll pool
Not equal to owner cash
Payroll comes before distributions
Cash to hold back
Fund payroll timing gaps
Cover lab bill cycles
Keep marketing test budget
Reserve for compliance needs
How many TRT patients do you need to make owner income?
You don’t size a Testosterone Replacement Therapy Clinic by unique patients first; you size it by visit cadence and retention. In Year 1, 473 monthly treatments at about $238 collected each is roughly $112,574 in monthly revenue, and if patients average one paid treatment per month, that’s about 473 monthly patient encounters, not confirmed unique patients.
Fast planning math
473 treatments per month
$238 average collected price
$112,574 monthly revenue
One paid visit equals one encounter
What drives owner income
Owner pay plus payroll first
Then add fixed overhead and reserves
Divide by monthly contribution per patient
Grow only with compliant care
Testosterone Replacement Therapy Clinic Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
Want the six TRT clinic income drivers?
1
Patient Volume
$1.35M
More active patients drive the biggest share of revenue, so retention and repeat visits lift owner take-home fastest.
2
Pricing Mix
$238
A higher blended treatment price raises revenue per visit without adding matching labor or rent.
3
Provider Capacity
60%-85%
Higher clinician utilization turns fixed staff into profit, and weak scheduling cuts EBITDA fast.
4
Cost Control
20.5%
Keeping lab, supply, and other variable costs in check protects margin on every treatment.
5
Acquisition Efficiency
4%-6%
Lower marketing spend keeps new patient growth from eating the cash the clinic earns.
6
Overhead Load
$21.8K/mo
Rent, IT, insurance, and licensing set the monthly break-even floor, so lean overhead protects owner income.
Testosterone Replacement Therapy Clinic Core Six Income Drivers
Active TRT Patient Panel And Retention
Active Patient Retention
This driver is the number of TRT patients who stay active and keep coming back on schedule. 473 capacity-adjusted monthly treatments in Year 1, rising to 3,148 in Year 5, takes revenue from $1,126k per month to $7,754k per month, so repeat visits are what pay fixed overhead before owner draw.
Here’s the quick math: every missed follow-up cuts treatment revenue and lab-related gross profit. If retention slips, the clinic has to replace lost volume with more paid ads, and that usually hurts cash flow. Pushing volume without proper care also raises compliance and churn risk, so growth has to stay tied to safe follow-up timing.
Track Follow-Up Completion
Measure active patient count, follow-up completion rate, missed-visit rate, and monthly treatments per clinician. Keep a weekly view of booked, completed, and overdue visits, plus revenue per active patient. That shows whether growth is coming from real retention or from costly reacquisition.
Book the next visit before checkout.
Flag overdue patients every week.
Review no-shows by provider.
Test reminder timing and channel.
If retention weakens, fix the care flow before adding ad spend. Stronger follow-up keeps treatment and lab dollars in-house, which lifts contribution margin and makes owner pay more predictable. The clean gain is fewer lost patients, not faster patient replacement.
1
TRT Clinic Pricing Model And Payer Mix
Pricing and payer mix
The clinic’s price ladder runs from $150 to $170 for a Registered Nurse to $450 to $510 for a Senior Medical Director. But Year 1 collected price is only about $238 per treatment, so owner pay depends on what actually lands in cash, not just what gets billed. Because this is fee-for-service, the mix of cash-pay and insurance sets the ceiling on distributable income.
Cash-pay usually improves timing, while insurance can add denials and billing work. If payer mix shifts toward insurance, revenue can look strong while cash collections lag, and that delay cuts the cash available for payroll, overhead, and owner draws.
Track collected price, not just billed price
Measure collected price per treatment, payer mix, and denial rate every month. Here’s the quick math: if the clinic stays near $238 collected per treatment and collections stay clean, more of each visit turns into spendable cash for the owner. If the mix drifts and collections slow, the income statement can look fine while take-home pay tightens.
Split cash-pay and insurance monthly.
Reconcile billed vs collected revenue.
Watch denial-heavy payers closely.
Flag any drop in collected price.
2
Provider Capacity And Owner Role
Provider Capacity And Owner Role
If provider time runs short, revenue tops out before demand does. In Year 1, capacity ranges from 400% for Registered Nurses to 600% for the Senior Medical Director; by Year 5, it rises to 800% to 850%. Staffing also scales from 6 clinical staff to 22, so the owner’s income depends on whether enough licensed hours exist to support each month’s treatment volume.
The tradeoff is simple: more hiring raises capacity, but payroll lands before volume fully matures. Owner-clinician work can reduce early payroll pressure if legally allowed, but lower-cost staffing cannot replace required medical oversight. If the schedule is thin, cash flow tightens and owner pay gets squeezed. Matched staffing protects margin.
Track Capacity Before You Add Payroll
Measure booked treatments, provider hours, and visits per licensed role against monthly demand. Use those inputs to test when added clinicians will actually earn back their cost. The key question is whether you are buying revenue capacity or just adding fixed cost.
Track idle hours by role.
Compare payroll to booked volume.
Use owner time early, if legal.
Add staff only when schedules stay full.
Watch for missed follow-ups and underused provider blocks. Both slow collections and cut gross profit, which delays the owner’s draw. The right staffing mix keeps the clinic medically safe and keeps payroll aligned with demand.
3
Medication, Lab, And Supplies Gross Margin
Medication, Lab, and Supply Margin
This driver is the gap between treatment revenue and direct clinic costs like laboratory analysis fees, medical supplies, and hormones. In Year 1, lab fees are 65% of revenue and supplies plus hormones are 55%, so combined COGS is 120%. That means direct cost can outrun revenue before rent, payroll, or owner pay. By Year 5, combined COGS improves to 90%.
Here’s the quick math: if billed revenue is $100, Year 1 direct cost is $120, while Year 5 direct cost is $90. The owner only gets paid after this layer, so small shifts matter a lot. Bundled pricing pushes cost risk onto the clinic, while pass-through billing changes revenue quality and collections risk. Do not treat sourcing or prescribing as a margin shortcut.
Track Direct Cost Per Treatment
Measure lab cost per visit, drug and supply cost per protocol, and gross margin by treatment type. Tie each to treatment count, average order value, and collection rate so you can see whether margin improves as volume grows. If combined COGS stays near 120%, the clinic cannot fund overhead or owner draw cleanly.
Watch the mix between bundled and pass-through billing. One clean rule helps: if a protocol can’t hold margin at scale, reprice it or tighten the order set. A move from 65% lab cost to 50%, and from 55% to 40% on supplies and hormones, is worth real cash because every point flows straight into take-home income.
4
TRT Clinic Marketing Cost And Lead Conversion
Lead Conversion And Acquisition Cost
Marketing only helps owner income when a new TRT patient stays long enough to pay back the acquisition cost. The model shows Digital Marketing and Acquisition at 60% of revenue in Year 1, easing to 40% by Year 5, with card processing at 25%. A separate Year 1 benchmark puts marketing at about $811k on $135M revenue.
If consult conversion, no-shows, or early drop-off are weak, revenue can grow while cash to the owner shrinks. Cheap leads are not cheap patients. Referrals and retention matter because they spread acquisition cost across more treatment months, which protects margin and free cash for payroll, compliance, and owner draw.
Track cost per booked consult.
Track no-show and close rates.
Track referral share monthly.
Track 90-day retention by channel.
Cut CAC, Lift Show Rate
Measure paid ads, local search, referrals, and consult-to-start conversion separately, so you can see which channel actually pays back. The quick math is simple: if acquisition cost rises and retention stays short, the clinic may book revenue but still lose distributable cash.
Keep claims tight, because claims-based marketing can create compliance risk and force costly ad changes. Push referrals, improve reminders, and cut no-shows. A small lift in conversion or retention can matter more than a bigger ad budget because it lowers the cost per patient month.
5
Fixed Overhead, Compliance, And Reserves
Fixed Overhead And Compliance Reserves
Fixed overhead comes before owner pay. In this clinic model, rent, EHR and IT, and malpractice insurance total $183k/month, or $2.196M/year. That load equals 163% of Year 1 revenue, then falls to 24% by Year 5 as volume grows. If collections slow, the owner’s draw gets squeezed fast.
Compliance is not optional. Add admin staff, licensing, legal review, billing support, medical waste if needed, insurance, and cash reserves into the true overhead number. Reserves lower near-term distributions, but they keep payroll funded and the clinic open if claims, denials, or a care issue hits cash flow.
Track The Full Fixed-Cost Run Rate
Measure overhead as a monthly cash burn, not a yearly budget. Start with the known base of $183k/month, then layer in admin, billing, legal, licensing, and reserve funding. The key test is simple: if collections slip for one month, can the clinic still cover payroll, rent, and malpractice without cutting owner pay first?
Track fixed cost by line item.
Separate compliance from growth spend.
Set a reserve before distributions.
Review cash collections weekly.
What this hides: a clinic can look profitable on paper while cash stays tight. If revenue is thin in Year 1, taking money out too early can weaken continuity and raise risk for the owner and staff.
6
Testosterone Replacement Therapy Clinic Business Plan
30+ Business Plan Pages
Investor/Bank Ready
Pre-Written Business Plan
Customizable in Minutes
Immediate Access
Compare lean, base, and high TRT clinic owner-income scenarios
Owner income scenarios
Lower capacity, slower retention, and higher acquisition spend push owner income down fast. The base model still throws off strong EBITDA, while the high case adds volume but also more staffing and compliance load.
Low, base, and high owner income cases for the clinic.
Scenario
Low CaseLow Case
Base CaseBase Case
High CaseHigh Case
Launch model
The clinic opens slower and never reaches the modeled treatment mix.
The clinic follows the model's Year 1 to Year 5 ramp.
The clinic fills capacity faster and converts more visits into cash.
Typical setup
Volume stays below plan, retention is softer, and marketing plus lab and supply costs run high.
The clinic runs near modeled capacity with 473 monthly treatments, 20.5% COGS plus variable costs, and EBITDA growing from Year 1 to Year 5.
Volume runs above plan, collections are cleaner, acquisition cost improves, and stronger pricing offsets the added staffing and compliance load.
Cost drivers
Lower capacity
slower retention
higher marketing spend
higher lab and medication cost
more payroll drag
473 monthly treatments
20.5% COGS
variable fees
steady pricing
modeled staffing mix
Higher capacity
stronger retention
lower acquisition cost
improved COGS
more staffing and compliance
Owner income rangeBefore owner reserves
$300k - $800kDownside plan
$809k - $1.7MCore plan
$1.7M - $7.2MUpside plan
Best fit
Use this to test a cautious launch, weaker referral flow, and a bigger cash reserve need.
Use this as the working plan for budgeting, staffing, and cash flow.
Use this to test upside if the clinic scales well and keeps cash collection tight.
!
Planning note: Scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
In the provided model, revenue is $135M in Year 1 and grows to $930M by Year 5 The model starts with 473 capacity-adjusted monthly treatments at about $238 average collected price Revenue is not owner income because payroll, reserves, taxes, and debt service still come out after collections
Break-even timing depends on payroll and reserves, which are not provided Using only listed costs, Year 1 fixed overhead is $183k per month and COGS plus variable expenses equal 205% of revenue The model’s $1126k monthly revenue clears listed overhead, but true break-even needs provider pay and compliance costs
No, but a non-clinician owner still needs properly licensed providers, medical oversight, and compliant operations An owner-clinician may reduce early payroll pressure if legally allowed A manager or semi-absentee owner must budget for more provider payroll, admin coverage, malpractice, EHR/IT, and reserves before taking distributions
The biggest drivers are active patient retention, pricing, payer mix, provider capacity, medication and lab costs, and marketing efficiency In Year 1, listed lab and supply costs are 120% of revenue, marketing and card fees are 85%, and fixed overhead is $2196k per year Payroll can change the final answer materially
Plan distributions after payroll, taxes, debt service, compliance costs, and reserves, not from top-line revenue The source model shows $8546k in Year 1 pre-payroll operating profit, but that is not safe take-home Keep a reserve for claim delays, lab bills, medication and supply purchases, payroll timing, and marketing tests
About the author
Jason Burke
Business Operations Writer
Jason Burke is a business operations writer at Financial Models Lab who researches how small businesses launch, operate, and earn money, with a focus on first-year business costs and the shift from side project to real business. He writes simple business projections and practical guidance that helps non-finance readers make business planning feel clearer, more useful, and easier to act on.
Choosing a selection results in a full page refresh.