Veterinary Endoscopy Service Owner Income: $788K Year 1 EBITDA
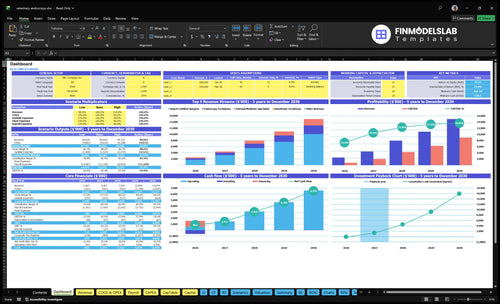
A veterinary endoscopy service owner can potentially earn a clinical salary plus distributions, but only after the business covers labor, supplies, equipment support, fixed overhead, reserves, taxes, and debt service In the researched base model, Year 1 revenue is $2467 million, EBITDA is $788,000, and the lead surgeon salary line is $220,000 By Year 5, revenue reaches $14974 million and EBITDA reaches $8954 million under higher staffing and utilization assumptions These are planning assumptions, not guaranteed owner income
Owner income$1.01MNet margin32%Revenue for target pay$1.56MBusiness difficultyHard
Want the six income drivers that matter most?
1
Case Volume
1,475/mo
Filled procedure slots drive cash fastest, and owner take-home follows cash after reserves, not bookings.
2
Mix and Price
$1,394
Shifting toward higher-fee surgeon and specialist cases lifts revenue per slot, even if volume stays flat.
3
Referral Flow
Month 2
A steady referral pipeline keeps the schedule full early and helps the clinic reach break-even by Month 2.
4
Labor Load
$83.8K/mo
Payroll is the biggest ongoing drag at $83.8K a month, so staffing to case load protects EBITDA.
5
Equipment Burden
$665K
The $665K equipment build ties up cash, so uptime and repair control decide how much profit reaches owners.
6
Ancillary Revenue
79%
Add-on services and a 79% contribution margin mean more of each case stays after direct costs.
Want to test your owner income case?
Owner income calculator
Estimate owner take-home and target-pay gap from revenue, margin, costs, reserves, and target pay.
!
Planning note: Research-based planning estimate only. It is not guaranteed salary, tax advice, or owner distribution advice.
Want to check owner income in the Veterinary Endoscopy Service model?
How many veterinary endoscopy procedures per month to pay the owner?
If the Veterinary Endoscopy Service wants to pay the owner a $220,000 lead-surgeon salary, it needs about 93 completed cases per month before reserves and debt. Here’s the quick math: the average collected fee is $1,394, variable costs are 21%, so contribution is about $1,101 per case; that has to cover $18,900 of fixed overhead plus about $65,417 of non-owner payroll. At the model volume of 1,475 monthly cases, the business has plenty of cushion, so the real risk is utilization, not price.
Pay target math
$1,394 average collected fee
21% variable cost rate
$1,101 contribution per case
93 cases to fund owner pay
Cost load to cover
$18,900 monthly fixed overhead
$65,417 non-owner payroll
$220,000 owner salary target
1,475 model monthly cases
Is a veterinary endoscopy service more profitable when owner operated?
For the Veterinary Endoscopy Service, owner-operated delivery can be more profitable when the owner performs procedures, because it keeps the $220,000 lead surgeon salary in-house and still shows $788,000 Year 1 EBITDA. Adding associate surgeons helps scale, but each full-time equivalent specialist adds about $185,000 in cost. This is not the right model for every market, because referral flow, case complexity, hiring risk, and owner burnout change the math.
Owner model math
$220,000 salary stays in-house
$788,000 Year 1 EBITDA shown
Owner keeps more procedure profit
Best when cases stay dense
Scale tradeoffs
Each specialist adds $185,000
Board-certified surgeons grow from 2 to 6
More surgeons mean more capacity
Burnout and hiring risk still matter
How much can a veterinary endoscopy clinic owner make?
A Veterinary Endoscopy Service owner can make $220,000 in clinical salary in Year 1 if they’re the lead surgeon, plus possible distributions from $788,000 Year 1 EBITDA; see What Are The 5 Core KPIs For Veterinary Endoscopy Service? for the operating drivers behind that income.
Owner Pay
$220,000 lead surgeon salary
$2.467 million Year 1 revenue
$788,000 Year 1 EBITDA
Salary and distributions stay separate
Income Drivers
Monthly procedure count
Referral demand strength
Owner clinical role
Staffing, financing, and ownership splits
Key Takeaways
Higher case volume spreads fixed overhead and payroll.
Procedure mix sets average fee and margin.
Referrals keep utilization high enough to cover costs.
Equipment cash needs can lag accounting profit.
Compare low, base, and strong veterinary endoscopy profit scenarios
Owner income scenarios
Owner income moves fast with case count, fee mix, and staffing scale. The low, base, and high cases show how the same service line earns very different results as volume and utilization rise.
Three planning cases for owner income tied to volume, fees, and margin.
Scenario
Low CaseDownside case
Base CaseCore case
High CaseUpside case
Launch model
This is the lower earnings path if Year 1 demand and staffing run closer to plan but not beyond it.
This is the modeled middle path if Year 3 volume and pricing land near plan.
This is the stronger earnings path if Year 5 capacity, pricing, and utilization all hold up.
Typical setup
About 1,475 cases a month at a $1,394 average fee, 79% contribution margin, $18.9k fixed overhead, and about $1.005M annual payroll, with $788k EBITDA and a $220k lead surgeon salary base.
About 428 cases a month at a $1,859 average fee, 82% contribution margin, and about $4.282M EBITDA as capacity and staffing scale.
About 781 cases a month at a $1,597 average fee, 83.5% contribution margin, and about $8.954M EBITDA with fuller staffing.
Cost drivers
1,475 monthly cases
$1,394 average fee
79% contribution margin
$18.9k fixed overhead
$1.005M payroll
428 monthly cases
$1,859 average fee
82% contribution margin
scaled staffing
$4.282M EBITDA
781 monthly cases
$1,597 average fee
83.5% contribution margin
fuller capacity
$8.954M EBITDA
Owner income rangeBefore owner reserves
$220k - $788kLower income band
$4.282MCore income band
$8.954MHigh income band
Best fit
Use this to test the downside if referral flow starts slow or staffing stays underused.
Use this as the main operating plan for budgeting, hiring, and cash needs.
Use this to test upside if referrals stay strong and the clinic fills more of its schedule.
!
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Veterinary Endoscopy Service Core Six Income Drivers
Case Volume And Utilization
Case Volume And Utilization
This driver is the number of completed endoscopy cases you actually turn into billed work, plus how fully you use the surgeon, internal medicine specialist, and technician time. At 1,475 completed monthly cases and $206,000 in monthly revenue, the clinic has to keep the pipeline full enough to spread $18,900 of fixed overhead and $83,750 of payroll. When volume slips, owner pay falls fast.
Here’s the quick math: the business carries $102,650 in monthly overhead and payroll before variable case costs. Utilization assumptions are 55% for board certified surgeon services, 45% for internal medicine specialist services, and 60% for endoscopy technician services. That means case flow must stay steady, because complex cases need longer rooms, anesthesia time, and technician support.
Track Completion Rate, Not Just Leads
Measure scheduled cases, completed cases, and utilization by role every month. A full schedule does not help if cases cancel, rooms sit open, or staff time is blocked by long procedures. The owner’s take-home income depends on converting referrals into billed procedures fast enough to cover payroll and overhead.
Track these inputs closely: completed cases, 55% / 45% / 60% utilization by role, case complexity, room time, anesthesia time, and technician hours. If referral flow weakens, push handoff speed, case follow-up, and schedule discipline. Fewer completed cases means less cash left for owner pay.
Watch booked-to-completed case conversion.
Flag long-room cases early.
Match staffing to referral volume.
Review utilization weekly, not quarterly.
Procedure Mix And Pricing
Procedure Mix and Pricing
This driver is the case mix across board-certified surgeon, internal medicine specialist, and endoscopy technician services, plus the price actually collected on each case. In Year 1, prices are $3,200, $1,800, and $450, and the blended collected fee is about $1,394 per completed case. That mix sets revenue per case and the room time, anesthesia, and biopsy burden behind gross margin.
Here’s the quick math: 100 completed cases at $1,394 collected fee is about $139,400 in revenue. If the mix tilts toward higher-complexity surgeon cases, revenue per case rises but labor and anesthesia also rise; more technician-heavy cases do the opposite. Local referral demand and case complexity decide the real collected fee, so one flat price can miss the margin.
Track fee by case type
Track realized fee, not just list price, by procedure type each month. The inputs are case mix, referral demand, biopsy frequency, anesthesia time, room time, and technician hours. If more cases need longer rooms or extra biopsy work, the true margin changes fast. Price should follow complexity bands, not a universal fee.
Watch contribution margin by case type and by referrer. A $3,200 surgeon case can still underperform if it uses more anesthesia and staff time than priced in, while a $450 technician service only works when scheduling is tight. The owner’s take-home income improves when collected fee per case stays ahead of variable labor, so salary and distributions aren’t squeezed.
Ancillary Revenue Capture
Ancillary Revenue Capture
Ancillary revenue is the extra collected fee tied to one endoscopy case: biopsy fees, pathology add-ons, pre-procedure diagnostics, anesthesia charges, consulting veterinarian work, and follow-up care. The model says consulting veterinarian pricing is $250 per service, but that revenue is not in the core revenue calculation, so it is upside if it is billed and collected.
This driver lifts revenue per appropriate case without much new fixed cost, so it can improve gross margin and owner pay. Here’s the risk: if charges are missed, cash leaks out; if you bill for work that is not medically needed, referral trust drops and future volume can fall. One clean line: bill what you do, and only what you do.
Measure the add-on capture rate
Track ancillary revenue by case type, not just total visits. The core inputs are case count, add-on frequency, fee per add-on, and collection rate. If a biopsy, pathology step, diagnostic test, or anesthesia add-on was medically needed, it should show up in the bill and in cash collected.
Use a charge checklist at intake, during the procedure, and at discharge so nothing gets missed. Keep the rule tight: bill for needed work, not extra work. That protects referral trust and turns more of each appropriate case into profit that can support owner draw, reserves, and smoother cash flow.
Referral Pipeline
Referral Pipeline
Veterinary endoscopy lives on referred cases. In Year 1, referral marketing and outreach are modeled at 5% of revenue, or about $10,300/month on $206,000 monthly revenue, so the pipeline is a real operating cost, not a side task.
If referrals slow, utilization drops and contribution margin shrinks before payroll and fixed overhead are covered. With $83,750 monthly payroll and $18,900 fixed overhead, fewer scheduled cases directly reduce the owner’s salary, reserve build, and distribution capacity. By Year 5, outreach falls to 3%, or about $6,180/month, if repeat referrals stay strong.
Keep Referrals Warm
Track referred cases, repeat-referral rate, report turnaround time, and utilization. The pipeline only helps owner income when it fills rooms fast enough to spread payroll and equipment costs across enough cases.
Measure weekly referred case count.
Track report delivery speed.
Watch repeat referrals by source.
Compare outreach spend to revenue.
Clean handoffs and fast reporting protect the referral loop. If follow-up slips, the owner pays for outreach but loses the margin that funds pay, reserves, and distributions.
Clinical Labor Model
Clinical Labor Mix
If the owner fills the lead surgeon seat, that pay is labor compensation, not pure profit, so take-home income is lower than headline revenue suggests. The model lists $220,000 for the lead board certified surgeon, $185,000 for an associate surgeon, and $175,000 for the head of internal medicine; those named roles total $580,000 before technician and coordinator pay.
If you add an associate surgeon before case flow is stable, fixed payroll rises before utilization does, so cash can tighten even when revenue grows. The key input is who performs each procedure, because owner pay shifts from salary to profit only after labor hours are covered by booked, collected cases.
Measure Pay Per Clinical Hour
Track collected revenue per clinician hour, payroll per completed case, and utilization by role. Split the owner’s clinical salary from profit draw so you can see whether growth is paying for labor or creating real margin.
Before adding an associate-led seat, test the schedule against referrals and booked cases. If volume is not already covering the named clinical payroll and the rest of staff pay, delay the hire or keep the owner in the lead seat until utilization catches up.
Equipment And Repair Burden
Equipment and Repair Burden
$665,000 in endoscopy gear and buildout ties up owner cash before the clinic reaches steady volume. That hits income twice: first through financing or cash outlay, then through ongoing maintenance at 3% of revenue, which is about $6,180 per month if Year 1 revenue runs near $206,000 monthly.
Here’s the quick math: the burden includes $85,000 for HD camera systems, $120,000 for rigid and flexible scopes, $65,000 for anesthesia workstations, and $250,000 for suite buildout and sterilization. Repair shocks and replacement reserves matter because EBITDA is not distributable cash; strong paper profit can still leave the owner short on take-home pay.
Track cash, not just profit
Set a monthly repair and replacement reserve from day one. Track maintenance as a percent of revenue, equipment downtime, and cash left after payroll, debt service, and supplies. If the 3% benchmark gets beat up or scopes sit idle, owner draws should slow until cash cover is rebuilt.