How Much Can a Vitamin IV Therapy Clinic Owner Make? $58k/Month
You’re trying to turn clinic revenue into owner income, not confuse sales with take-home pay In these five-year planning assumptions, the clinic moves from a first-year loss to about $101k/month of EBITDA-like profit in Year 2 and about $578k/month in Year 3 before tax, debt service, reserves, and distributions
Owner income$578k/moNet margin34%Revenue for target pay$1.7M/moBusiness difficultyHard
Want to test your owner pay?
Owner income calculator
Estimate owner take-home and target-pay gap from monthly revenue, margin, operating costs, reserves, and target pay.
!
Planning note: Research-based planning estimate only. It is not guaranteed salary, tax advice, or owner distribution advice. Actual take-home depends on collections, staffing, taxes, and reinvestment.
Want the six income drivers?
1
Visit Volume
1.9K-7.5K/mo
Visits rise from 1,905 a month to 7,455 by Year 3, so volume drives most of the top-line jump.
2
Ticket Mix
$202-$212
A richer service mix and small price lifts push revenue per visit higher without needing the same jump in foot traffic.
3
Clinical Payroll
$425K-$710K
Clinical payroll climbs as RN and NP coverage expands, so staffing has to stay in step with booked visits.
4
Supply COGS
15%-12%
Fluids and single-use supplies fall from 15% to 12% of revenue, and each point saved drops straight to margin.
5
Marketing Spend
4%-2%
Marketing eases from 4% to 2% of revenue, so lower customer-acquisition cost helps protect cash as the clinic matures.
6
Fixed Overhead
$9.6K/mo
Fixed overhead stays near $9.6K a month, so the clinic needs enough booked volume to cover rent, insurance, software, and utilities.
Want to check owner income in the Vitamin IV Therapy Clinic model?
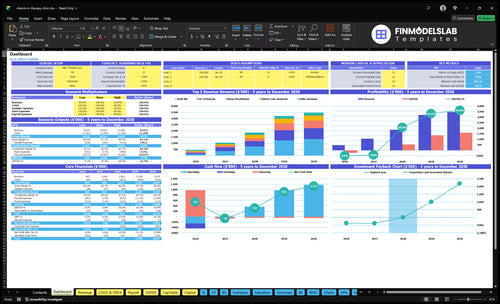
The Vitamin IV Therapy Clinic Financial Model Template shows revenue by provider, visit volume, ticket size, capacity, COGS, marketing, fees, fixed costs, staffing, and owner income. It flags Year 1 loss, Year 2 $101k/month profit, and Year 3 $578k/month profit; use the assumptions tab to test scenarios and open the full model for deeper planning.
Owner-income model highlights
Owner income output chart
Revenue and margin build-up
Assumptions for scenario testing
What profit margin can an IV therapy clinic earn?
A Vitamin IV Therapy Clinic can reach 85% gross margin in Year 1 and 88% by Year 5, but net profit still hinges on payroll and overhead; see How Much Does It Cost To Open A Vitamin IV Therapy Clinic? for the setup side. After marketing and payment fees, contribution improves from 79% to 84%, and Year 3 lands at about a 37.2% EBITDA-like margin, or $578k profit on $1,552k monthly revenue.
Gross margin
85% in Year 1
88% by Year 5
Supply costs fall from 15% to 12%
IV fluids, nutrients, and single-use supplies drive cost
Profit reality
Contribution rises from 79% to 84%
Marketing and payment fees sit above supply costs
Net profit depends on payroll and overhead
Year 3: 37.2%, or $578k
How many IV drips does it take to pay the owner?
For Vitamin IV Therapy Clinic, there isn’t a universal drip count. Use the target pay formula: monthly visits = (fixed costs + payroll + target owner pay) / contribution per visit; with a Year 2 contribution per visit of about $164, the model needs about 363 visits/month to support roughly $10k/month for the owner, and about 424 visits/month to hit the full plan.
Use the pay formula
Visits = costs ÷ contribution
$205 ticket drives the math
80.2% stays after variable costs
That leaves about $164 per drip
What the model needs
363 visits/month supports $10k owner pay
424 visits/month covers the target model
$50k payroll is a big load
$96k fixed overhead must be covered
Is an owner-operated IV therapy clinic more profitable?
A Vitamin IV Therapy Clinic can be more profitable early if the owner replaces a paid manager or clinician role, but only if the owner’s licensed scope and availability can cover demand. Once you build a staffed model, payroll rises fast: $425k in Year 1 and $710k in Year 3, while capacity can scale to 7,455 monthly visits by Year 3 and 1,314 by Year 5. Compliance and supervision costs still need to be modeled, not guessed.
Why owner-operated can help
Owner labor can replace a salary.
Year 1 cash burn can stay lower.
Best if the owner can treat clients.
Capacity still depends on owner time.
What staffed growth costs
Add RN, NP, and technician payroll.
Add coordinator and manager pay too.
Year 1 payroll: $425k.
Year 3 payroll: $710k.
Key Takeaways
Volume drives profit; Year 2 can reach profitability.
Staffing ahead of bookings burns cash fast.
Fixed overhead sets the breakeven floor.
Repeat visits and supply control protect margin.
Compare low, base, and high owner-income scenarios
Owner income scenarios
Owner income moves fast here because visits, ticket size, staffing, and fixed payroll all scale together. These cases show how a Year 1 ramp, Year 3 model, and Year 5 maturity change monthly cash.
Monthly owner income shifts with volume, pricing, and staffing.
Scenario
Low CaseDownside case
Base CaseBase case
High CaseUpside case
Launch model
This is the lower-earnings path, built on Year 1 ramp and negative monthly cash before tax.
This is the modeled middle case, built on Year 3 scale and steadier clinic cash flow.
This is the stronger earnings path, built on Year 5 maturity and fuller clinic capacity.
Typical setup
About 1,905 visits a month at a $202 ticket, $385k revenue, 85% supply gross margin, $96k fixed overhead, and $425k payroll.
About 7,455 visits a month at a $208 ticket, $1.552M revenue, about 86.5% supply gross margin, and $710k payroll.
A mature clinic with a $220 ticket, $2.891M revenue, 88% supply gross margin, and $930k payroll.
Cost drivers
Low visit volume
$202 ticket
85% supply margin
$96k fixed overhead
$425k payroll
Higher visit density
$208 ticket
86.5% supply margin
$710k payroll
stable staffing
Higher ticket
88% supply margin
fuller capacity
$930k payroll
scale efficiency
Owner income rangeBefore owner reserves
-$146k/moYear 1 ramp
$578k/moYear 3 scale
$1.56M/moYear 5 maturity
Best fit
Best for stress-testing early ramp, slower patient flow, and a tighter cash buffer.
Best for a normal planning case and lender or investor review.
Best for testing upside when the clinic runs near capacity and staffing scales well.
!
Planning note: These scenario figures are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Vitamin IV Therapy Clinic Core Six Income Drivers
Appointment Volume
IV Appointment Volume
Appointment volume is the main income driver because the clinic’s fixed costs do not move with every drip. At 1,905 monthly visits in Year 1, the clinic loses about $146k/month; at 4,245 visits in Year 2, it reaches about $101k/month profit; at 7,455 visits in Year 3, profit rises to about $578k/month.
That means owner pay depends on booked and completed treatments, not just demand on paper. Volume must match provider count, chair capacity, open hours, and local demand. Hiring ahead of bookings burns cash fast, because payroll starts before the schedule is full.
Match Staff To Booked Visits
Track daily booked visits, show rate, and chair utilization, then staff to the schedule you can actually fill. One clean rule: do not add a provider unless booked volume supports the next month’s capacity.
Use a simple forecast: visits per provider per day × open days × chairs. If bookings lag, cut hours or delay hires; if demand holds, expand in steps. That protects gross margin and keeps cash available for owner draws instead of idle labor.
Watch booked visits weekly
Limit empty chair time
Hire after demand proves out
Retention And Marketing Efficiency
Retention And Marketing Efficiency
Marketing cost starts at 4% of revenue in Year 1 and drops to 3% by Year 3, while payment processing stays at 2%. That means owner income improves when each client comes back more than once, because the first-sale acquisition cost gets spread across more visits and more revenue.
The key inputs are new leads, booking rate, repeat visit rate, average ticket, and marketing spend. Here’s the quick math: if leads convert but do not repeat, you buy revenue noise, not profit. Reviews, local partnerships, memberships, events, and tight follow-up scheduling all raise the share of revenue that turns into take-home income.
Track Repeat Revenue, Not Just Leads
Measure repeat visits per client, cost per booked visit, and marketing as a percent of revenue. If marketing holds at 4% while processing stays at 2%, the clinic is already giving away 6% of sales before labor, supplies, and rent. That only works if retention keeps revenue dense.
Use follow-up calls, same-day rebooking, and membership offers to lift repeat use. Track which channels bring returning clients, not just first visits. A channel that fills the calendar once but does not bring clients back can raise gross revenue and still lower owner pay.
Track repeat visit rate by source
Measure marketing as revenue percent
Compare booked visits to repeat visits
Test memberships and follow-up timing
Clinical Staffing Costs
Clinical Staffing Costs
Clinical staffing costs can move owner pay more than rent in an IV therapy clinic. Annual payroll rises from $425k in Year 1 to $600k in Year 2, $710k in Year 3, and $930k by Year 4. That includes RN labor, Nurse Practitioner coverage, IV technicians, patient coordination, and management coverage.
Here’s the quick math: payroll is a fixed cost that must be covered by appointment margin. Owner-as-clinician can reduce early cash burn, but under-staffing caps visits and over-staffing raises the breakeven visit count. The key inputs are staffed hours, provider mix, and monthly visit volume.
Track Labor Mix Weekly
Measure labor by role, not just total payroll. Track RN hours, NP coverage, technician shifts, and admin time against booked visits. If payroll jumps before volume does, owner income gets squeezed fast. If the owner works clinically, count that time too, since it lowers cash burn but can hide real labor cost.
Watch payroll as a % of revenue
Match staffing to booked chairs
Delay hires until demand holds
Separate clinical and admin labor
Supply Cost Control
Supply Cost Control
IV drip supply cost covers fluids, nutrients, tubing, needles, and single-use medical supplies. The model shows 15% of revenue in Year 1, 135% in Year 3, and 12% in Year 5. That Year 3 figure needs a data check, because 135% would push gross margin negative. At $1.552M/month in Year 3 revenue, each 1-point COGS move changes profit by about $15.5k/month.
So inventory waste, vendor pricing, and unused vials hit the owner’s take-home pay fast. Higher supply cost lowers gross margin, which leaves less cash for payroll, rent, and owner draw. When supply leakage grows, the clinic can look busy and still pay the owner less.
Tighten Cost Per Drip
Track COGS per treatment by fluids, nutrients, tubing, needles, and discard. The key inputs are treatment count, average ticket, service mix, and vendor price per vial. If premium drips lift ticket size, keep supply cost per visit on target so margin rises too.
Treatments per month
COGS per drip
Expired or unused vials
Vendor price changes
Use par levels and expiry checks before every reorder. If unused inventory is not tied to booked appointments, you turn cash into spoilage. At this scale, a 1-point COGS drift is roughly $15.5k/month, so small waste needs fast action.
Fixed Clinic Overhead
Fixed clinic overhead
$96k/month of fixed overhead sets the breakeven floor before the first appointment. The named costs add to $23.1k a month: $5k rent, $1k utilities, $15k malpractice insurance, $800 software, $500 general liability insurance, $600 cleaning, and $200 website costs. That means the full overhead figure includes other clinic costs beyond the list.
For the owner, this is pure cash pressure every month, even when bookings are light. Overhead is the floor, not the prize. Bigger space and more rooms raise the volume needed to cover fixed costs, so rent signed before demand is proven increases payback pressure and can delay owner pay.
Track the burn before you sign
Build the fixed-cost model from the actual lease, insurance, software, cleaning, and website bills, then test it against planned appointment volume. The key check is simple: can likely monthly visits cover $96k/month before owner salary or profit draw?
Track each fixed cost line item.
Match room count to demand.
Stress test slower booking months.
Delay long leases until demand is proven.
Use location size as an income decision, not just an ops choice. If the space is too large for current demand, the clinic needs more visits just to break even, and that pushes cash flow down before the owner sees real profit.
Average Ticket And Service Mix
Average Ticket And Service Mix
The average IV therapy ticket is the blended price per visit across premium infusions, add-ons, memberships, wellness packages, and corporate bookings. It moves from about $202 in Year 1 to $208 in Year 3 and $220 in Year 5, so higher realized pricing lifts gross profit per appointment if supply cost and labor stay in line.
Here’s the quick math: the move from $202 to $220 is $18, or about 8.9%. At 1,000 visits a month, that is $18,000 more revenue before variable costs. Discounts can fill the calendar, but if they pull down the average ticket, they can also cut gross profit per visit and shrink owner pay.
Protect Realized Price
Track realized ticket by service line, not just menu price. Measure add-on attach rate, membership share, corporate booking price, and discount rate. Those inputs tell you whether the clinic is earning more per chair hour or just selling more low-margin visits. Keep service language focused on wellness benefits and avoid unsupported medical claims.
Watch average ticket by service
Set a discount floor
Test premium add-on bundles
Compare membership vs. one-off visits
Forecast revenue from booked visits
If a promo raises bookings but lowers the average ticket, owner income can still fall. The best mix is the one that raises revenue per appointment without adding much supply cost or labor, so more of each visit drops into contribution and cash flow.