Start An AI Healthcare Solutions Company In 6–18 Months
AI Healthcare Solutions Bundle
You’re launching into hospitals and clinics, so the plan must prove clinical value before sales scale This guide covers the 6–18 month launch path, from use-case validation and HIPAA-ready data handling to pilot sales, EHR workflow planning, and a five-year revenue model check Use the next step to test whether your first pilot can support $3,000–$5,000 monthly subscription pricing and $6,000–$10,000 setup fees
Time to Open6-8 monthsLaunch runwayLaunch Sequence6 stagesUse case firstKey BottleneckValidation gateProcurement pathFirst Revenue StepPaid pilotTrial converts
Launch timeline
This is a short web summary of the launch plan, and the XLSX export contains the detailed Gantt Chart.
How do you get first customers for an AI healthcare startup?
First customers for AI Healthcare Solutions usually come from one narrow clinical use case, one credible clinical sponsor, and a small paid pilot. Hospitals buy when you can show measurable impact, security readiness, and a clear implementation path; for a quick cost check, see What Is The Estimated Cost To Open And Launch Your AI Healthcare Solutions Business?. In Year 1, a realistic first sale is a $6,000-$10,000 setup fee plus $3,000-$5,000 monthly per module, with sales mix often at 50% diagnostic AI, 30% treatment optimization, and 20% workflow automation.
First buyer signal
Narrow the use case
Pick one workflow pain
Use one clinical sponsor
Keep the pilot small
What closes the pilot
Show measurable impact
Prove security readiness
Map the procurement path
Define conversion plan
What mistakes should founders avoid when launching AI healthcare software?
Founders should not launch AI Healthcare Solutions without clinical validation, clear regulatory classification, and workflow fit. Here’s the quick math: do not assume every trial converts, because Year 1 trial-to-paid conversion is only 60%, CAC starts at $1,500, and the annual marketing budget starts at $150,000; prove one use case first, then add modules.
Main launch mistakes
No clinical validation before launch
Unclear regulatory classification
Weak data governance and controls
No EHR workflow integration
Readiness checks
Test HIPAA safeguards and data rights
Check model performance and bias
Require audit trails and support coverage
Confirm pilot buyer ownership early
Do AI healthcare startups need FDA approval?
AI Healthcare Solutions may need FDA clearance or authorization if it diagnoses, recommends treatment, or changes clinical care; admin-only workflow tools may avoid FDA review but still need HIPAA and security checks. Treat this as a regulatory pathway review, not legal advice, and pair it with What Is The Most Critical Metric For AI Healthcare Solutions To Measure Its Impact On Patient Outcomes? before pilots; the FDA’s 510(k) review clock is 90 FDA days, while broader clinical claims can stretch validation beyond 6–18 months.
FDA Risk Triggers
Diagnoses patients
Recommends treatment paths
Influences clinician decisions
Claims outcome improvement
Launch Readiness
Classify before pilots
Sign data-use agreements
Document access controls
Keep audit trails
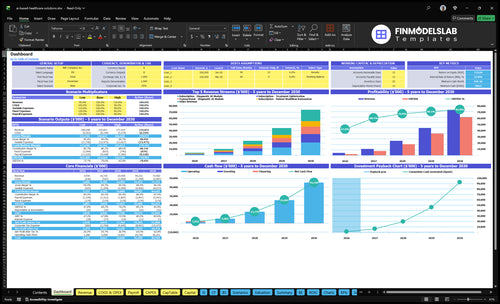
AI Healthcare Solutions Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
Confirm what must be ready before selling to providers
Launch readiness checklist
Use this go-live approval checklist before opening so the team can confirm compliance, platform readiness, staffing, and first revenue flow.
1Regulatory
HIPAA safeguards mappedCritical
Protected health information needs access, storage, and sharing controls before any pilot starts.
Data rights documentedCritical
You need written rights for training data, client data, and output use before launch.
Product class reviewedHigh
The launch path changes fast if the system is treated as clinical decision support or another class.
2Validation
Validation plan signedCritical
Define test sets, pass rules, and signoff rules before any hospital sees the model.
Pilot accuracy threshold setHigh
You need a clear bar for false positives, false negatives, and drift before go-live.
Clinical review completedHigh
A clinician must confirm the output fits real workflow and patient risk.
3Platform
EHR integration path definedCritical
The electronic health record handoff must be mapped before onboarding the first clinic.
Support owner assignedHigh
One owner should handle issues, tickets, and escalation so pilots do not stall.
Pilot environment testedHigh
Run the product in a safe test setup so launch bugs do not hit live care.
4Infrastructure
Cloud capacity confirmedHigh
Hosting needs enough room for current pilots and the Year 1 sales plan.
Security tools installedCritical
Data security and privacy tools must be live before any protected data moves.
Model license terms clearedHigh
Third-party AI model licensing needs written terms before revenue starts.
5Team
Clinical advisor namedCritical
Someone with care experience needs to review outputs and edge cases.
ML lead assignedCritical
A clear technical owner keeps model quality, retraining, and bug fixes moving.
Integration engineer namedHigh
Hospitals will expect fast help for interfaces and data mapping.
Customer success owner namedHigh
Onboarding needs one owner because churn rises when setup drags.
6Go-to-market
Sales lead assignedHigh
The first deals need one owner for outreach, demos, and follow-up.
Pilot sponsor confirmedCritical
A buyer sponsor must back the pilot or trial-to-paid can stall.
Launch pricing approvedCritical
Pricing has to support $1,500 CAC, 60% trial-to-paid, and the 16% variable-plus-COGS load.
Cash runway coveredCritical
The plan must cover the Month 2 low point of $769k and $5,000 office rent until Month 3 break-even.
Which launch drivers matter most?
1Clinical Focus
Pilot fit
Locks the first workflow, which speeds pilot approval and keeps value easy to defend.
2HIPAA Ready
Trust gate
Sets privacy and security basics early, so hospital reviews move faster and stall less.
3Data Validation
Evidence gate
Uses legal, representative data, so the model earns clinical trust and pilot conversion.
4EHR Fit
EHR fit
Fits existing screens and handoffs, so clinicians do not face extra clicks or alert fatigue.
5Pilot Pipeline
Paid pilot
Builds sponsor-led pilots with clear ROI, turning demos into setup fees and monthly revenue.
6Support Capacity
Day-one team
Keeps onboarding and support staffed, so pilots do not outrun the team.
Clinical Use-Case Focus
One Clinical Use Case
A healthcare AI launch is ready when it solves one named workflow for one named user. If the problem stays broad, hospitals can’t defend the purchase, and the pilot turns into a vague demo. That slows approval and makes day-one operations shaky because the team still has to guess what value to show.
The readiness signal is simple: named user, defined workflow, baseline metric, and pilot success target. Start with clinician interviews, score the pain, pick one module, and test pricing against the Year 1 mix of 50% Diagnostic AI, 30% Treatment Optimization, and 20% Patient Workflow Automation.
Lock The Pilot Scope
Before opening, write the use case in plain terms: who uses it, where it fits in review or handoff, what metric moves, and what “success” means. That keeps the build small enough to ship and gives procurement a clear case for the setup fee and monthly subscription.
Interview clinicians first.
Score the top pain points.
Choose one module only.
Test pricing early.
Document baseline and target metrics.
If the use case is fuzzy, procurement has no defensible reason to buy, and first revenue slips. If it’s sharp, pilot approval is faster and the product fit is cleaner from day one.
1
Regulatory And HIPAA Readiness
HIPAA and Security Readiness
If the platform touches protected health information (PHI), hospital launch depends on privacy safeguards, access controls, audit trails, and vendor files being ready before the first security review. The review path also changes if the software diagnoses, recommends treatment, or only supports workflow, so that classification has to be settled early.
The practical risk is treating compliance as a post-launch checkbox. That can slow procurement, pull in legal and IT review, and block day-one use even when the software works.
Front-Load the Compliance Packet
Build the launch file before outreach: classification review, data-use agreements, security package, incident response plan, and one named compliance owner. Tie in legal counsel, a clinical advisor, and the technical controls that enforce least-access and logging. One clean packet speeds buyer trust and cuts back-and-forth in information security review.
Classify the use case first.
Document PHI handling rules.
Test access controls and logs.
Keep vendor docs current.
One missing policy can stall launch. If the security pack is incomplete, the hospital may delay onboarding, which pushes back first revenue and leaves the team supporting a live workflow without approved controls.
2
Data Access And Model Validation
Legal Data and Clinical Validation
Healthcare AI only opens on time if the training and test data are legal, documented, and broad enough to match the patients the product will serve. A demo that only works on narrow or unapproved data will not survive hospital review, and weak evidence can slow pilots for months.
Before day one, the team needs dataset sourcing, rights review, de-identification where appropriate, and a validation protocol with performance metrics, bias checks, clinician review, and a monitoring plan. One line matters here: if the model cannot support real care decisions, it is not launch-ready.
Lock the evidence before pilot
Start with the exact use case, then prove the data rights and the model fit. Ask: who owns each dataset, what patient groups are covered, what was de-identified, and what output is safe for a clinician to use. That sequence keeps legal review, clinical review, and product launch moving together.
Confirm data rights in writing.
Document de-identification steps.
Test bias across user groups.
Get clinician sign-off on outputs.
Assign model monitoring ownership.
Weak validation raises launch risk fast: slower procurement, less clinical trust, and lower pilot conversion. Strong validation does the opposite, because buyers see evidence that the model works on their patients, not just a clean demo set.
3
EHR And Workflow Integration
EHR And Workflow Integration
EHR integration is what keeps clinicians from chasing a separate tool during a busy shift. If the software does not fit existing screens, handoffs, alerts, and review steps, launch slips because staff have to build a new habit before they trust the product.
For opening on time, the launch needs data exchange design, alert logic, an implementation plan, IT security review, sandbox testing, and a support playbook. The key dependencies are an integration engineer, the customer IT team, a clinical sponsor, and data access. If the workflow creates alert fatigue or duplicate work, frontline users push back fast and day-one adoption drops.
Integration Readiness Check
Before go-live, verify the software fits the hospital’s actual order, review, and escalation flow. Get the IT team to confirm access early, then test in a sandbox with real workflow steps, not a demo path. One clean line: if the tool adds clicks, it slows launch.
Document who owns each step, from interface setup to support after launch. Make sure the clinical sponsor signs off on alert rules, since bad thresholds can create duplicate work or missed follow-up. A tight handoff plan lowers rework, speeds approval, and helps the team operate from day one.
Confirm screen placement before build.
Test alerts for duplicate work.
Assign one IT owner, one clinician.
Load support steps before launch.
4
Pilot Customer Pipeline
Pilot Pipeline
Opening on time depends on getting a hospital pilot lined up before launch. A real pilot needs a clinical sponsor, economic buyer, procurement path, pilot scope, and success metric; without all five, you may have interest but no budget owner, so the launch slips.
This also drives day-one cash. A paid pilot can start with a $6,000–$10,000 Year 1 setup fee and $3,000–$5,000 monthly subscription, but only after security review, terms, and workflow scope are clear. The first win is not broad AI talk; it’s proof that one workflow gets better.
Prebuild the pilot path
Before opening, build the target account list, get advisor introductions, and send a pilot proposal with the security packet and ROI case. Ask each account to name the sponsor and buyer, then map the procurement steps, pilot dates, and success target in writing.
Named sponsor
Named buyer
Procurement owner
Scoped workflow
Measured outcome
One clean rule: no budget owner, no paid pilot. If the terms are signed before launch, demo interest turns into revenue faster and the team can support a real customer from day one.
5
Staffing And Support Capacity
Staffing and Support Capacity
This launch driver matters because the platform can’t open on time if the team cannot validate, sell, integrate, and support on day one. For this kind of AI healthcare product, the core launch bench needs a clinical advisor, an ML or data science lead, healthcare compliance support, an integration engineer, a sales lead, and an implementation or customer success owner.
The weak spot is simple: selling pilots faster than the team can implement them. Year 1 planning also needs to carry 30% customer success and onboarding cost, plus 70% sales commissions and performance marketing, so headcount and support load have to match the pilot pace, not the pitch deck.
Launch staffing checklist
Before launch, lock role ownership, written advisor agreements, a support process, an escalation path, and a pilot onboarding checklist. Keep the scope tight enough for the integration engineer and customer success owner to handle hospital IT needs without creating a backlog.
Here’s the quick test: every pilot should have a named owner, a backup, and a clear handoff from sales to implementation. If any of those are missing, first revenue may still close, but day-one delivery will slip. That creates slower onboarding, more support tickets, and avoidable cash pressure.
Start with one clinical use case, not a broad platform Then confirm data rights, review HIPAA and regulatory scope, build an MVP, recruit clinical and technical advisors, and sell a small paid pilot The planning assumptions support Year 1 subscriptions of $3,000–$5,000 per month, setup fees of $6,000–$10,000, and 60% trial-to-paid conversion
Plan for 6–18 months before a serious hospital or clinic launch The long poles are data access, clinical validation, information security review, EHR workflow fit, legal review, and procurement Clinics may move faster than hospitals, but you still need a clear pilot scope, sponsor, and support plan before first revenue
Yes, you need clinical input before pilots A clinical advisor helps test whether the use case fits real care workflows, whether metrics matter, and whether buyers will trust the output Pair that with an ML or data science lead, compliance support, integration help, sales ownership, and customer success coverage for implementation
Clinical validation and procurement usually create the biggest delays Data rights, HIPAA controls, security documents, EHR integration, legal review, and physician adoption can each slow the launch Your model should test delayed revenue, a $150,000 Year 1 marketing budget, $1,500 CAC, and only 60% trial-to-paid conversion
The first revenue step is usually a paid pilot, implementation fee, or subscription pilot with one clinic or hospital The Year 1 assumptions price modules at $3,000, $4,000, and $5,000 per month, with one-time fees from $6,000 to $10,000 Keep the pilot narrow and tie payment to measurable workflow or care improvement
About the author
Patrick Hughes
Small Business Writer
Patrick Hughes is a small business writer who focuses on business affordability analysis for side-hustle builders planning with limited capital. He researches how small businesses launch, operate, and earn money, with a practical eye on business idea evaluation. His writing highlights common costs new founders often miss, helping readers make clearer, more realistic decisions before they start.
Choosing a selection results in a full page refresh.