How do ambulatory surgery centers get patients for first cases?
Ambulatory surgery centers get first cases from surgeon-owners and affiliated surgeons who already have eligible outpatient work, not from ads alone. If you’re sizing startup needs, What Is The Estimated Cost To Launch An Ambulatory Surgery Center? sits beside case commitment, because Year 1 volume only works when surgeons bring patients. That plan often assumes 8 providers, 1,235 monthly cases, and about $539,250 in monthly revenue.
Where first cases come from
Committed surgeon-owners start volume
Affiliated surgeons add eligible cases
Orthopedic, general, and ophthalmic drive flow
Referral paths support, not replace, surgeons
What must be ready
Secure payer contracts early
Finish provider credentialing fast
Set prior authorization workflows
Build scheduling and revenue-cycle setup
How long does it take to open an ambulatory surgery center?
An Ambulatory Surgery Center usually takes 12 to 24 months to open in the US. The timeline depends on state review, certificate of need, plan approval, construction, inspections, equipment install, accreditation survey timing, Medicare certification, payer credentialing, and surgeon block time. Construction can finish first, but first cases may wait if life-safety approval or payer contracts lag, so Year 1 revenue should track a ramp toward 1,235 monthly cases at 60% to 65% utilization.
What drives timing
State review can add months
Certificate of need may delay opening
Plan approval and inspections take time
Equipment and survey timing matter
What to plan for
Use 12 to 24 months as the range
Cases can start after buildout, not before approvals
Model 1,235 monthly cases in Year 1
Assume 60% to 65% utilization ramp
What licenses are needed to open an ambulatory surgery center?
To open an Ambulatory Surgery Center, you typically need state ASC licensure, any required certificate of need, building permits, fire and life-safety approvals, controlled-substance and pharmacy setup if applicable, plus a Centers for Medicare & Medicaid Services certification path; tie this work to What Is The Most Important Indicator Of Success For Your Ambulatory Surgery Center? because surveys and payer enrollment can delay revenue.
Core Licenses
Get state health department ASC licensure
Check CON rules: 35 states plus DC
Secure local building and zoning permits
Pass fire and 2012 Life Safety Code review
Revenue Gatekeepers
Prepare for 42 CFR Part 416 compliance
File Medicare enrollment through CMS-855B
Align policies before survey readiness
Avoid payer delays; Medicare penalties can hit 2.0%
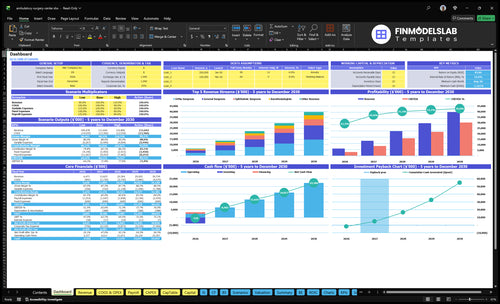
Ambulatory Surgery Center Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
Confirm whether the ASC is safe and commercially ready to open
Launch readiness checklist
Use this go-live approval checklist to confirm the Ambulatory Surgery Center is ready before opening.
1Licensing
Entity setup filedCritical
The center needs a legal entity before licenses, leases, and payer work can move.
State ASC license approvedCritical
This is the core operating permit for same-day surgery.
Certificate of need clearedHigh
If your state requires CON, clear it before build-out and staffing.
CMS coverage path mappedHigh
Map Conditions for Coverage gaps before survey prep starts.
Emergency transfer agreement signedCritical
You need a clear hospital transfer path for emergencies and survey review.
2Facility
Procedure rooms signed offCritical
Rooms must support the planned procedures before the first case.
Recovery area readyCritical
Patients need a safe recovery area with monitored discharge flow.
Sterile processing readyCritical
Clean instrument flow has to work before any surgery starts.
HVAC and airflows testedHigh
Air handling affects infection control and room uptime.
Medical gas testedCritical
Medical gas must be reliable before anesthesia cases begin.
3Vendors
Surgical equipment installedCritical
Core equipment has to be in place before case scheduling opens.
Biomedical checks completedCritical
Testing proves critical devices work and are safe to use.
Implant supply contracts signedHigh
Implants need a locked source so cases do not slip.
Maintenance and waste vendors activeHigh
Service and waste pickup keep the center compliant and running.
4Staffing
Surgeons credentialed and scheduledCritical
You need approved surgeons before the first block time is sold.
Anesthesia coverage staffedCritical
Anesthesia has to be covered for every planned case day.
Nursing and scrub teams readyCritical
Case flow breaks fast if the room team is thin.
Administrator and infection lead namedHigh
One person must own operations and infection control.
5Revenue
Payer contracts loadedCritical
No contracts means slow or no payment after launch.
Prior auth workflow setHigh
Approvals protect cash and cut avoidable denials.
Scheduling and charge capture testedCritical
If scheduling misses charges, revenue leaks on day one.
Coding and billing system readyCritical
Clean coding and claims are what turn cases into cash.
6Cash
Monthly model reconciledCritical
Validate 1,235 cases, $539,250 revenue, 185% variable costs, and known fixed spend.
Cash runway through Month 8Critical
The model's low point is Month 8, so funding must cover that dip.
Fixed commitments lockedHigh
Known monthly commitments start at $50,000 before missing maintenance.
Go-live signoff approvedCritical
Open only after compliance, staffing, vendors, and revenue flow are all green.
Which six drivers decide whether the ASC opens cleanly?
1Regulatory Path
12-24 mo
State licensure, CON, and survey clearance set the opening date and can block first cases.
2Physician Cases
1,235/mo
Signed surgeons and anesthesia coverage drive case volume and decide if OR time is worth staffing.
3Buildout Ready
Month 9
Compliant rooms, life-safety systems, and infection control decide whether inspections pass before opening.
4Staffing Lead
8 providers
Eight providers plus nursing and tech coverage must be ready before the first case.
5Payer Cycle
$539K/mo
Contracts, coding, and authorizations must be live, or clean cases still turn into slow cash.
6OR Workflow
Vendor-ready
Procedure trays, implants, and sterilization must be in place before the first case runs.
Regulatory Approval And Certification Path
Regulatory Approval Path
An ambulatory surgery center can’t open on time until the state licensure path is clear, and in some states that also means a certificate of need decision, plus building and life-safety approvals. The launch signal is written approval, not a near-finish checklist. If the facility is not survey-ready, first cases slip, and so do payer enrollment and Medicare-certified surgery center status.
Here’s the quick math on risk: one delayed inspection, plan review, or CON ruling can block the first billable case, even if the space is built and the surgeons are ready. That makes approval timing a cash issue, not just a compliance issue. Inspection clearance, an emergency transfer agreement, and complete compliance files have to be done before day one.
What to verify before opening
Start with the state health department, then lock the plan review, policy build, and survey prep in order. The center should have survey-ready policies, staff training, a mock survey, and deficiency fixes done before the final inspection window. One clean rule: if a reviewer asks for a file, it should already be in the folder.
Confirm state license steps early
Check CON need by state
Finish life-safety plan review
Keep transfer agreement signed
Run a mock survey
Train staff before inspection
Correct deficiencies fast
What this estimate hides is timing risk. If one approval slips, staffing, payer setup, and first-day case scheduling all move with it. So the launch plan should track each approval as a hard gate, not a loose task.
1
Physician Case Commitment
Physician Case Commitment
Physician case commitment is the launch driver that decides whether an ambulatory surgery center (ASC) can open on time and run full enough from day one to justify the fixed cost. Year 1 planning assumes 2 orthopedic surgeons, 2 general surgeons, 1 ophthalmic surgeon, 2 anesthesiologists, and 1 pain physician, driving 1,235 total cases per month.
The readiness test is not interest alone. You need a signed eligible procedure list, block schedule, payer participation, and a working referral flow. If those are late, the center may still staff rooms, anesthesia, and front desk coverage before enough cases are booked, which hurts operating-room utilization and delays first revenue.
Lock Volume Before You Hire
Get each physician to commit in writing to case mix, monthly volume, and block time before final staffing. Here’s the quick math: the model depends on 24 orthopedic, 30 general, 195 ophthalmic, 24 anesthesia-related, and 26 pain cases per month. If one service line slips, the gap shows up fast in the schedule.
Get signed volume targets.
Map eligible procedures.
Load block schedules early.
Test referral handoffs.
Confirm payer participation.
What this estimate hides is timing risk: if commitments come late, staffing and supply plans can outgrow actual day-one demand, and the center opens with empty room time instead of booked cases.
2
Facility Buildout And Life-Safety Readiness
Buildout That Passes Life-Safety
An ambulatory surgery center cannot open on time if the rooms, utilities, and patient flow do not match the procedure mix. The launch risk is simple: if procedure rooms, recovery bays, sterile processing, HVAC, medical gas, and emergency systems fail survey or fire review, first cases stop. That is especially true when Year 1 planning assumes 1,235 cases per month.
What matters most is passing construction, fire, life-safety, biomedical, and infection-control checks before scheduling patients. If design gaps show up after the buildout is done, the center can lose weeks to rework, reinspection, and delayed accreditation. That pushes back first revenue and leaves staffing, supplies, and leased space sitting idle.
Verify the Build Before You Book Cases
Lock the plan early, then test it against the actual day-one flow. The founder should confirm architectural plan approval, contractor sequencing, equipment room fit, utility validation, and a mock patient walkthrough. One clean run through intake, procedure, recovery, and discharge will surface bottlenecks faster than a paper checklist.
Match room count to procedure mix
Validate recovery and storage space
Test HVAC and medical gas
Document fire and infection controls
Walk the full patient path
If any core system is unfinished, delay the opening date rather than start with a weak schedule. A center can look built and still fail day one if turnover, sterilization, or patient flow is not ready. The safe launch signal is simple: every required room works, every utility is live, and every check is signed off.
3
Staffing And Clinical Leadership
Clinical Team Ready
For an ambulatory surgery center (ASC), staffing is a go/no-go item. Before the first case, you need a medical director, credentialed surgeons, anesthesia coverage, nursing, scrub techs, infection prevention oversight, an administrator, and trained front-desk and revenue-cycle staff. If any of those are thin, the center can’t open safely or keep the schedule full.
Here’s the quick math: the Year 1 plan assumes 8 providers and 1,235 monthly cases, so staffing should match that load, not a future-state org chart. Readiness means completed credentialing, privileges, competencies, emergency drills, policy sign-offs, and real schedule coverage. Hiring late or training after survey raises cancellation risk and can delay first revenue.
Build Coverage Before Survey
Lock the roster early and map each role to a live duty schedule. Verify who covers each room, each shift, and each emergency backup slot, then document it before survey work starts. That keeps training tied to actual case flow, not guesswork.
Confirm medical director sign-off.
Finish credentialing and privileges.
Test anesthesia and nursing coverage.
Train front desk and billing staff.
Run emergency drills before opening.
Use a simple readiness file for each person: license, credentials, competencies, policy acknowledgments, and training date. If one key role is missing, the center may still pass paperwork but fail day-one operations because cases need full team coverage to start and stay on time.
4
Payer Contracting And Revenue Cycle
Payer Contracting & Cash Flow
Payer contracting is what turns an ambulatory surgery center (ASC) case into cash. If contracts, credentialing, coding, and prior authorization are not done before opening, you can perform a clinically clean case and still get delayed or denied payment.
Here’s the quick math: Year 1 modeled monthly revenue is about $539,250. Billing and collections fees at 35% equal about $188,738 a month, so weak revenue-cycle setup hits cash fast. One clean one-liner: if it isn’t billable, it isn’t launch-ready.
Load Payer Rules Before First Case
Before opening, verify that payer contracts are loaded, fee schedules are tested, authorizations are confirmed, claim forms are mapped, and patient responsibility workflow is live. That sequence matters because revenue starts with the first claim, not the first surgery.
Confirm provider credentialing and payer enrollment.
Test charge capture and coding rules.
Map prior auth by procedure.
Send sample claims before launch.
Train staff on estimates and collections.
What this setup hides is timing risk: if cases start before billing rules are clean, the center can run full days of surgery and still sit on unpaid claims. The bottleneck is performing cases that are clinically ready but not cleanly billable.
5
Equipment, Supplies, And Operating-Room Workflow
Day-One Equipment Readiness
Day-one opening lives or dies on the room being fully stocked for the exact specialties scheduled. If the tray, implant, drug, sterilization path, or vendor service contract is missing, the first case gets canceled and staff, patients, and payers feel it right away. This driver covers procedure-specific equipment, instruments, sterile processing, pharmacy setup, biomedical checks, maintenance agreements, and operating-room turnover.
Here’s the quick math: with modeled monthly revenue of $539,250, medical and surgical supplies at 80% of revenue imply about $431,400/month in supply spend before implants. That makes inventory control a launch issue, not just an ops task. What this estimate hides is the working capital needed to stock preference cards, cover vendor lead times, and hold backup trays for the first weeks.
Lock the Supply Path Before First Cases
Before opening, verify stocked preference cards, validated sterilization, working equipment, and delivery dates for every vendor. Run a simulated case turnover and time the handoff from room cleanup to the next start. If the cycle breaks on one tray, one implant, one drug, or one service contract, fix it before the first booked day.
Match equipment to launch specialties.
Confirm sterilization and biomedical checks.
Load implants, disposables, and pharmacy stock.
Sign maintenance and service agreements.
Lock vendor delivery schedules in writing.
Rehearse turnover with the full team.
Assign one owner to the supply list and one owner to room flow. That split keeps case delays from hiding inside purchasing, and it gives you a clean yes or no on first-day readiness.
Start with physician case commitment, market feasibility, and the state approval path The researched base case opens with 8 providers, 1235 modeled monthly cases, and 60% to 65% Year 1 utilization Then sequence licensure, facility design, construction, staffing, payer contracting, revenue-cycle setup, and first-case scheduling
Plan on 12 to 24 months in many US markets, but the real driver is dependency timing Certificate of need review, architectural approval, construction, inspections, accreditation survey timing, Medicare certification, and payer credentialing can all move the opening month A finished facility still may not be billable without payer readiness
It depends on the state, payer mix, and Medicare strategy Many launch plans prepare for accreditation or Medicare certification because payers and patients expect survey-ready operations Build policies, credentialing files, emergency protocols, infection control, sterile processing, and life-safety records before the survey window, not after construction ends
First revenue is delayed when scheduled cases are not billable Common blockers include missing payer contracts, incomplete provider credentialing, weak prior authorization workflow, untested coding, and claim setup gaps In the Year 1 planning case, about $539,250 in monthly revenue depends on 1235 cases moving through clean scheduling, care, billing, and collections
Validate demand and approvals before signing Confirm surgeon commitments, eligible case mix, state licensure rules, certificate of need exposure, facility requirements, and payer feasibility The base model assumes 2 orthopedic surgeons, 2 general surgeons, 1 ophthalmic surgeon, 2 anesthesiologists, and 1 pain physician, so space planning should match that launch scope
About the author
Brian Fox
Local Business Observer
Brian Fox writes for Financial Models Lab with a focus on simple cash flow planning for early-stage founders turning a service idea into a real business. As a local business observer, he explains business costs in plain language and uses startup budget examples to show how revenue, expenses, and profit fit together. His practical, realistic style helps readers understand the numbers behind starting small and building with clarity.
Choosing a selection results in a full page refresh.