How To Open An Autism Support Service In 8 Weeks To 6 Months
To open an autism support service, define the service model first, then confirm state rules, hire qualified clinical staff, set up HIPAA-ready intake and records, prepare payer enrollment if needed, build referral sources, and start with a controlled first-client ramp The researched planning assumption is an opening timeline of 8 weeks to 6 months, with private-pay or caregiver coaching launches usually faster and insurance or Medicaid-funded clinical services slower In Year 1, planned monthly capacity is about $118,820 before direct supply and electronic health record transaction costs, based on staffing, session volume, pricing, and utilization assumptions The main bottleneck is not demand alone it’s qualified staff, payer approval, documentation readiness, and safe supervision before accepting clients
Time to Open6 monthsSetup windowLaunch Sequence5 stagesCompliance firstKey BottleneckStaffing gapApproval pathFirst Revenue StepSigned intakePayer approved
Launch timeline
Short web summary of the launch plan; the XLSX export has the detailed Gantt chart.
How do you get clients for an autism support service?
Get clients for Autism Support Service by building ethical referral pipelines first: pediatricians, schools, diagnosticians, early intervention networks, local autism organizations, parent groups, local search, and payer directories. For the intake KPIs behind that funnel, see What Are The Five Core KPIs For Autism Support Service Business? First revenue starts when a family signs intake and the case matches private-pay, school, referral partner, insurer-approved, or Medicaid-approved eligibility. If response time slips, families move on, so fast follow-up matters.
Best client sources
Start with pediatrician referrals.
Ask schools and diagnosticians.
Join local autism groups.
Use parent searches and directories.
Track intake fast
Count calls and eligibility checks.
Track assessment bookings and authorizations.
Log start dates and no-shows.
Match marketing to real capacity.
Year 1 assumes 70% RBT use.
BCBA supervisor use is 75%.
SLP and OT use are 65%.
Clinical psychologist use is 50%.
What autism support service launch mistakes should you avoid?
Avoid launching an Autism Support Service before clinical supervision, payer approval, and billing workflows are ready. With $118,820 in planned Year 1 monthly revenue capacity, the model only works if staffed capacity and utilization are real, because 65% direct costs leave little room for weak claims or slow collections. The quick check is simple: can the team assess, schedule, supervise, document, bill, and communicate with families every day, or not?
Launch risks to avoid
Don’t open before supervision works.
Don’t start before payer approval.
Don’t hire past capacity limits.
Don’t rely on one referral source.
Readiness checks that matter
Use intake forms for care plans.
Build notes for claims readiness.
Track documentation and billing load.
Watch authorizations and onboarding lag.
How long does it take to open an autism support service?
An Autism Support Service usually takes 8 weeks to 6 months to open. A private-pay caregiver coaching or limited home-based model can launch faster if state rules, insurance, staff, consent, scheduling, and documentation are ready, while insurance-funded ABA or multidisciplinary therapy takes longer because credentialing, payer contracts, prior authorizations, and Medicaid approval can delay first revenue. A clinic-based launch also adds lease, buildout, equipment, safety, and scheduling work, and Year 1 staffing assumes 3 BCBA Supervisors, 12 Registered Behavior Technicians, 2 speech-language pathologists, 2 occupational therapists, and 1 clinical psychologist.
Faster launch
8 weeks is the fast end.
Private-pay opens sooner.
Ready forms cut delays.
Consent and scheduling must be set.
Slower launch
6 months is common for full care.
Insurance approval slows cash flow.
Lease and buildout add time.
Do not serve payer clients early.
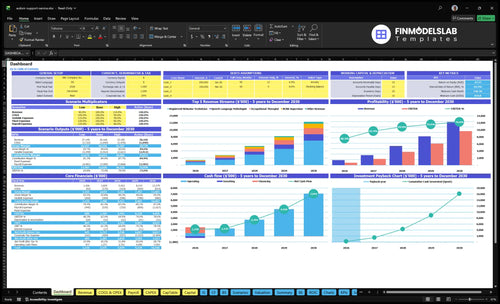
Autism Support Service Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
Confirm what must be ready before accepting the first autism support clients
Launch readiness checklist
Use this go-live approval checklist to confirm the service is ready to open before first client acceptance.
1Entity and license
Entity registeredCritical
A legal entity must exist before contracts, banking, and licensing steps can move ahead.
License path approvedCritical
The service cannot take clients until the state licensing path is confirmed.
Insurance boundCritical
Professional and general liability coverage should be active before any client care starts.
2Privacy and records
HIPAA policies activeCritical
HIPAA rules need clear internal controls before protected health information is handled.
Consent forms approvedCritical
Signed consent forms are required before first-client intake and treatment.
Records retention setHigh
Record retention rules keep charts, notes, and releases consistent and auditable.
3Staffing and supervision
BCBA coverage assignedCritical
Board Certified Behavior Analyst coverage must be in place before behavior services start.
Credentials verifiedCritical
Therapist licenses and certifications should be checked before client scheduling.
Background checks clearedHigh
Background checks reduce safety risk before staff enter client homes or the center.
Supervision plan setCritical
A written supervision plan is needed to support safe Registered Behavior Technician work.
4Intake and scheduling
Intake workflow testedCritical
The intake path must work end to end before the first family is accepted.
Eligibility checks verifiedCritical
Eligibility checks help prevent unpaid visits and avoid treatment delays.
Documentation templates loadedHigh
Notes, assessments, and service logs must be ready for day one charting.
Care plan templates readyHigh
Care plan templates keep goals, progress notes, and services consistent across clients.
5Billing and handoffs
Scheduling system liveHigh
A working schedule keeps therapists, families, and session slots aligned.
Billing setup testedCritical
Billing must post cleanly before the first claim or self-pay invoice goes out.
Claims workflow readyCritical
Claims handling must be ready before launch to protect cash flow.
Referral handoff definedHigh
Clear referral handoffs prevent gaps when a family needs speech, OT, or psychology support.
6Facility and go-live
Parent updates process readyHigh
Families need a simple update process before first-session communication starts.
Therapy rooms clearedCritical
Rooms must be safe, private, and set up before any in-person session begins.
Safety systems testedCritical
Security, access, and facility controls should work before clients enter the space.
Go-live cash clearedCritical
Cash should cover startup strain through the Month 2 low point before opening.
Want the six main launch drivers before you open?
1Service Scope
8 wks-6 mo
Narrow coaching can open faster; a clinical hybrid pushes setup toward the 6-month end.
2Compliance
License gate
State approval and payer rules control when you can accept clients and bill cleanly.
3Clinical Team
20 staff
Year 1 coverage needs 3 supervisors, 12 behavior technicians, 2 speech pathologists, 2 occupational therapists, and 1 psychologist before safe starts.
4Billing Ready
Claims ready
Credentialing and authorizations can delay cash even when schedules are full.
5Intake System
Go-live flow
Strong intake keeps assessments, notes, and care plans clean across multiple services.
6Referral Ramp
Referral flow
Pediatric and school referrals should fill staffed slots without overpromising to families.
Service Model And Scope
Scope Drives Launch
Service model is the first launch decision because it sets staffing, compliance, pricing, payer eligibility, records, and how fast you can open. An ABA-only or caregiver coaching model can start faster; a hybrid clinical model with speech, occupational therapy, or psychology takes longer because each service line adds licensing, documentation, and payer rules.
Year 1 pricing assumptions are $150 for BCBA Supervisor treatments, $65 for Registered Behavior Technician treatments, $130 for speech-language pathologist treatments, $130 for occupational therapist treatments, and $200 for clinical psychologist treatments. One clean rule: the broader the scope, the slower the setup and the more cash you need before day one.
Lock Scope Before Hiring
Before opening, write down exactly which services you will offer on day one: Applied Behavior Analysis, caregiver coaching, family support, social skills, in-home support, center-based support, speech therapy, occupational therapy, psychology, or a hybrid mix. Then match each service to the right staff, room setup, records, and payer path so you do not hire or bill for work you cannot legally or operationally deliver.
Here’s the quick check: if the model needs BCBA supervision, therapist schedules, prior authorization, or multiple treatment notes, build those workflows first. If you keep the launch narrow, you reduce approval risk and speed up first revenue. If you go broad on day one, expect more lead time for staffing, forms, and insurance setup.
Choose one launch scope.
Map staff to each service.
Match records to payer rules.
Confirm room and equipment needs.
Test billing before opening.
1
Compliance, Licensing, And Payer Eligibility
Licensing And Payer Readiness
This is the gate that decides whether you can open on time and serve families from day one. For autism support, rules can change by state and by service type, so you need the right license, Medicaid provider status, insurance panel setup, and supervision rules before you take the first client.
Miss this step and launch slows fast: claims can stall, intake gets delayed, and staff may be ready before the business is legally and financially ready. ABA, home-based support, caregiver coaching, and Medicaid-funded care can each have different rules, so a one-size plan can create compliance gaps and unpaid work.
Verify Before You Book
Map the exact service mix first, then check the state license path, payer enrollment, prior authorization, background checks, consent forms, privacy notices, documentation standards, and supervision rules. HIPAA, the Health Insurance Portability and Accountability Act, also means your records and privacy process need to be set before the first visit.
Build a go-live file for each payer and service line. Keep a live checklist for eligibility checks, referral approval, and documentation templates, because a client who looks ready can still be not billable until the payer verifies coverage and approves treatment.
Confirm state license rules by service
Check Medicaid and insurance enrollment
Prepare consent and privacy forms
Set supervision and note standards
Test eligibility and authorization flow
2
Qualified Clinical Staffing And Supervision
Safe Clinical Coverage
For an autism support service, staffing is the launch gate. Year 1 assumes 3 Board Certified Behavior Analyst supervisors, 12 Registered Behavior Technicians, 2 speech-language pathologists, 2 occupational therapists, and 1 clinical psychologist; if even one role is short, client starts slip because supervision, treatment hours, and backup coverage all depend on the full team.
Utilization also matters: Year 1 ranges from 50% for the clinical psychologist to 75% for BCBA supervisors. That means schedules must match realistic caseload limits, credential checks, background checks, onboarding, and supervision ratios before opening. No safe staff coverage means no safe client starts.
Build the coverage map first
Before you book the first family, verify each clinician’s license or certification, supervision need, and open hours. Map who covers assessments, direct treatment, parent meetings, and absences, then document backup coverage so one sick day does not stop care.
Check credentials before schedules.
Match caseloads to utilization.
Test backup coverage weekly.
If onboarding slips by even a week, day-one capacity drops fast because supervision and scheduling are linked. The launch plan should only open when the team can cover the first client set without stretching anyone past safe limits.
3
Payer, Billing, And Authorization Readiness
Payer And Claims Readiness
If you plan to bill insurance for autism therapy, credentialing and Medicaid billing readiness decide when cash can actually start. The model shows about $118,820 in monthly revenue capacity before direct costs, but that is not cash if prior authorizations, eligibility checks, or claims are still pending.
This setup includes payer contracting, billing codes, treatment documentation, claims workflow, denial tracking, and family responsibility estimates. With 25% electronic health record transaction fees in Year 1, weak billing setup can stall starts, delay collections, and force the center to open with more cash tied up than planned.
Bill Before You Start
Before opening, verify which payers are active, which services need authorization, and which codes match each therapy type. One missed rule can block claims even when families are already scheduled. Build the billing flow before the first intake so the team can collect from day one, not chase payments later.
Confirm payer contracts and credentialing status.
Test eligibility checks before first visits.
Map prior authorization steps by service.
Set denial tracking and follow-up owners.
Train staff on family responsibility estimates.
4
Intake, Care Coordination, And Documentation Systems
Intake and Records
If intake is clunky, the center cannot open cleanly. For an autism support service, the first-day path must handle intake calls, eligibility screening, payer checks, consent packets, assessment scheduling, care plans, progress notes, parent communication, secure records, scheduling, and follow-up tasks without gaps.
This matters even more in Year 1 because the model spans behavior support, speech, occupational therapy, and psychology. Applied Behavior Analysis intake also has to support assessments, supervision, authorizations, and treatment notes. If forms, notes, or records are inconsistent, the business is not launch-ready, and billing gets messy fast.
Test the full intake flow
Before opening, run one full client path from first call to first scheduled visit. Verify that the intake script, consent packet, documentation templates, and secure record setup all match the actual services offered. One clean workflow beats four half-built ones.
Match forms to each service type.
Check authorization steps early.
Set one owner for follow-up tasks.
Use one record standard across staff.
Here’s the quick math: if the intake path delays assessments or payer checks, first revenue slips too. That is why the front end has to be ready before demand starts. Clean intake supports smoother onboarding, fewer missed steps, and cleaner billing from day one.
5
Referral Pipeline And First-Client Ramp
Referral Ramp
Open with trusted referral sources, not broad volume. Pediatricians, school teams, diagnostic clinics, early intervention contacts, parent communities, local search, and payer directories bring the first leads, but each lead still needs fast intake follow-up, eligibility checks, and an assessment booked before start. If that chain breaks, families wait and day-one capacity sits empty.
Keep first clients inside staffed capacity and payer readiness. Year 1 utilization leaves room to ramp: RBTs at 70%, BCBA Supervisors at 75%, speech-language pathologists at 65%, occupational therapists at 65%, and clinical psychologists at 50%. Steady starts beat overpromising to families, and they protect early schedule stability.
Track the intake chain
Set up one launch dashboard before the first call. Track referral source, intake speed, eligibility, assessment booked, authorization status, and start date. That shows where leads stall and keeps booking tied to real capacity, not hope.
Assign one owner for follow-up
Respond to new leads same day
Match starts to open slots
Hold clients until payer approval
If referrals outrun staffing or approvals, the result is delay, rework, and unhappy families. Use the pipeline to keep the center open on time and start clients only when care, billing, and schedules are ready.
Yes, but the clinical work still needs qualified leadership A non-clinician owner should hire a clinical director or appropriate licensed supervisor before taking clients For the researched Year 1 plan, that means building around 3 BCBA Supervisors, 12 Registered Behavior Technicians, 2 speech-language pathologists, 2 occupational therapists, and 1 clinical psychologist, subject to state and payer rules
Home-based or caregiver coaching is usually faster to launch because it can avoid lease and buildout delays A clinic-based model may support broader services, but it adds facility setup, scheduling, equipment, safety, and staffing pressure Use the 8 weeks to 6 months range, then test whether your staff, records, payer setup, and referrals can support the model
Not always, but you need them before relying on insurance-funded revenue A private-pay or school-referred launch may start sooner if state rules and clinical readiness are met Insurance or Medicaid work needs credentialing, eligibility checks, prior authorization, documentation, and billing workflow before service starts Otherwise, the first signed family may not become collectible revenue
You need scheduling, intake, consent, secure records, documentation, billing, and referral tracking before serving families The model assumes electronic health record transaction fees at 25% of revenue in Year 1, plus 40% for medical supplies and sensory materials Keep the system simple, but make sure staff can document care and support claims from opening month
Hire leadership before demand and line staff as launch capacity becomes real Start with qualified supervision, then add therapists and technicians around signed referrals, payer approvals, and scheduling coverage The Year 1 plan assumes 20 clinical staff total, but utilization starts below full capacity, from 50% for psychology to 75% for BCBA supervision, so avoid hiring too far ahead
About the author
Patrick Hughes
Small Business Writer
Patrick Hughes is a small business writer who focuses on business affordability analysis for side-hustle builders planning with limited capital. He researches how small businesses launch, operate, and earn money, with a practical eye on business idea evaluation. His writing highlights common costs new founders often miss, helping readers make clearer, more realistic decisions before they start.
Choosing a selection results in a full page refresh.