How To Open A Balance Disorder Treatment Clinic In 6–12 Months
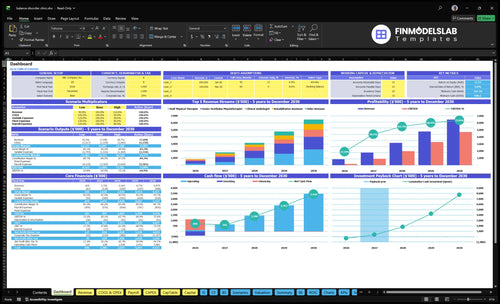
To open a balance disorder clinic in the United States, plan on a 6–12 month launch window, depending on payer credentialing, facility buildout, equipment delivery, and clinician hiring The core requirements are state clinical licensing, provider credentialing, malpractice coverage, HIPAA-ready workflows, diagnostic and rehab space, vestibular-trained staff, referral relationships, and a staged soft launch In the researched Year 1 model, monthly capacity at assumed utilization supports about 410 patient visits and roughly $696k in monthly revenue before ramp risk and collections timing The bottleneck is usually not demand it’s opening only after credentialing, billing, equipment calibration, and referral intake are ready
Time to Open6-12 monthsSetup windowLaunch Sequence8 stagesCompliance firstKey BottleneckPayer setupApproval pathFirst Revenue StepPaid evalReferral intake
Launch timeline
This is a short web summary; the XLSX export contains the detailed Gantt Chart.
What licenses are needed to open a vestibular clinic?
To open a Balance Disorder Treatment Clinic, start with state business registration, licensed providers working within scope, clinical leadership or a medical director if required, professional liability insurance, Health Insurance Portability and Accountability Act workflows, and payer credentialing before billing; this How To Write Balance Disorder Treatment Clinic Business Plan? guide can help sequence the launch. Requirements vary by state, ownership structure, and whether you offer diagnostics, rehab only, or physician-led evaluation; the Centers for Disease Control and Prevention reports 1 in 4 adults age 65+ fall each year, so documentation must be ready before the first patient.
Open legally
Register the legal business entity
Verify provider state licenses
Confirm clinical scope of practice
Secure professional liability coverage
Bill safely
Credential payers before insurance billing
Build HIPAA privacy workflows
Set documentation before first visit
Review CLIA only for lab testing
How long does payer credentialing take for a clinic?
Payer credentialing can be a major opening-date risk for a Balance Disorder Treatment Clinic, and it often sits inside the 6–12 month launch window. Don’t promise a quick start: leasehold improvements, vestibular equipment delivery and calibration, EHR and billing setup, clinician hiring, and payer enrollment all have to line up before first claims go out. Open only when claims workflow, provider enrollment status, referral intake, and patient financial policies are tested, or you can have ready visit volume with no clean revenue path.
Ready before opening
Leasehold work is done
Equipment is delivered and calibrated
EHR and billing are live
Clinicians are hired and enrolled
Risk if you open early
Claims can reject or stall
Referral intake may break
Patient payment rules may fail
Revenue can lag visits
What are the biggest mistakes opening a vestibular clinic?
The biggest mistakes opening a Balance Disorder Treatment Clinic are buying equipment too early, launching before payer credentialing and billing work, and pushing marketing before clinicians are trained on vestibular protocols. If claims fail or onboarding drags, cash runway and patient experience both take the hit. Start with a service-scope decision, then map equipment to each service and test billing before you go live.
Fix the launch order
Define services before buying gear
Build an equipment-to-service map
Train staff on vestibular protocols
Use a staff competency checklist
Test before full go-live
Run mock claims first
Test referral intake flow
Do a soft opening
Track a daily go-live dashboard
Balance Disorder Treatment Clinic Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
Confirm go-live readiness before accepting vestibular patients
Launch readiness checklist
Use this go-live approval checklist to confirm the clinic is ready before opening.
1Compliance
Entity and state licenses approvedCritical
Needed before contracts, claims, and hiring can move without risk.
Medical director documentedCritical
A named lead keeps clinical oversight clear from day one.
HIPAA workflows readyCritical
Patient data, access, and chart rules need a written process.
Malpractice coverage boundCritical
Coverage must be active before the first exam or treatment.
2Clinical
Vestibular rehab protocols approvedCritical
Standard care paths keep dizziness and balance treatment consistent.
Fall-risk procedures testedCritical
Fall checks lower injury risk during rehab and testing.
Referral intake rules setHigh
Intake rules route patients to the right clinician fast.
3Equipment
Diagnostic equipment installedCritical
Balance testing gear must be in place before the first visit.
Equipment calibrated and loggedCritical
Calibration logs support reliable results and audit trails.
EHR and billing liveCritical
Billing and charting must close the first claim cleanly.
4Staffing
Year 1 clinical team hiredCritical
Base staffing needs 2 senior vestibular physiotherapists, 1 audiologist, 1 PT, and 1 assistant.
Competency signoffs completedHigh
Competency signoffs prove staff can use each system safely.
Coverage schedule publishedHigh
Open hours need enough hands for visits, notes, and handoffs.
5Access
Payer credentialing or self-pay setCritical
Claims need credentialing done, or self-pay needs to be set.
Booking and intake liveCritical
Patients need one clear path to book and start care.
Referral channel activeHigh
Referrals need a simple handoff from local providers.
6Finance
Cash runway covers month 6Critical
Model shows minimum cash of $640k in month 6.
Vendor contracts lockedHigh
Supply, billing, IT, and calibration vendors need signed terms.
Go-live signoff completeCritical
Do not open until all core gates are green.
Want the six launch drivers in one view?
1Clinical Scope
6-12 mo
A signed service menu sets scope early, so licensing, equipment, and scheduling stay aligned.
2Provider Ready
2-1-1-1
Year 1 needs 2 vestibular PTs, 1 audiologist, 1 staff PT, and backup coverage before marketing ramps.
3Facility Ready
Calibrated
Installed and calibrated rooms and devices prevent launch delays and support about 410 monthly visits at utilization.
4Billing Ready
60% rev
Credentialing, test claims, and charge capture cut denials, but Year 1 collections can lag visits.
5Referral Network
50% rev
Active physician and partner referrals bring earlier evaluations and better treatment-plan conversion from day one.
6Operations Ready
Soft open
Test appointments and intake controls catch no-shows, safety issues, and claim gaps before full opening.
Clinical Service Scope
Clinical Service Scope
Scope has to be set before you open, because it decides what you can legally bill, what rooms you need, and what equipment must be ready on day one. A rehab-first launch is simpler than a full diagnostic center, while adding testing, BPPV treatment, concussion balance care, or physician-led evaluation adds more staffing, documentation, and payer setup.
The readiness signal is a signed service menu tied to provider scope and billing workflow. If that menu is vague, first-patient scheduling gets messy, equipment gets bought too early, and you can miss launch dates while you sort out licenses, payer enrollment, and room use. One bad scope decision can slow the whole opening.
Lock the service menu early
Before lease fit-out, decide exactly which services open on day one: diagnostic testing, vestibular rehab, fall-risk assessment, BPPV care, concussion balance care, or specialty evaluation. Then map each service to the provider scope, billing code flow, room use, and staff needed so you do not build for services you cannot launch yet.
Match services to licensed providers.
Separate rehab from diagnostic testing.
Test scheduling against the service menu.
Document billing rules before soft opening.
That sequence cuts equipment mistakes and makes first-patient booking cleaner. If a test or treatment is not in the signed scope, push it to phase two instead of forcing a delayed opening.
1
Provider And Staffing Readiness
Provider and staffing readiness
If the clinic opens before the care team is fully licensed and trained, the first problem is not demand, it’s safe capacity. Year 1 assumes 2 senior vestibular physiotherapists, 1 clinical audiologist, 1 staff physical therapist, and 1 rehabilitation assistant, with no neurologic specialist physical therapist until Year 2, so the opening plan has to match that bench.
The readiness signal is simple: licensed coverage, vestibular training, front-desk intake, billing support, and backup coverage. If any of those are weak, first-day scheduling gets thin, handoffs break, and marketing can outpace the team before the clinic can safely see patients.
Lock coverage before marketing volume
Here’s the quick check: confirm who is licensed, who is trained, who answers intake, who handles billing, and who covers sick days or leave. The Year 1 capacity assumptions are 650% for senior vestibular physiotherapists, 500% for the audiologist, 600% for the staff physical therapist, and 400% for the rehabilitation assistant, so the schedule should stay inside those limits until real throughput proves otherwise.
Verify active licenses before scheduling.
Train staff on vestibular intake.
Test billing handoff and backup coverage.
If the front desk can’t screen, route, and book cleanly on day one, the clinic risks avoidable delays, patient confusion, and missed revenue while the calendar fills faster than the team can safely treat.
2
Facility And Equipment Readiness
Facility and Equipment Readiness
This driver decides whether the clinic can see patients on time. If treatment rooms, safe gait and balance areas, diagnostic space, and EHR-linked equipment aren’t ready, first visits slip and staff sit idle. The room plan has to match the services you can actually bill, so the launch doesn’t promise care you can’t deliver on day one.
The real risk is not just buying equipment; it’s proving it works. Installed, calibrated, tested, and documented equipment before soft opening protects patient safety, reduces repeat visits, and avoids launch delays. If vendor lead time runs long or operators aren’t trained, the opening date moves and cash burn rises while the clinic waits.
Build the room flow before you buy gear
Start with the service menu, then map each room and device to a reimbursable service and a trained operator. Video nystagmography, video head impulse testing, posturography, and vestibular rehab tools only belong in the plan if they fit scope and staffing. That keeps the buildout tight and avoids paying for gear that can’t bill.
Confirm room flow limits fall risk.
Test each device with the operator.
Check EHR setup and charting.
Document calibration and service logs.
Train staff before first patient.
Run test patients in the exact order you’ll use on day one: intake, balance exam, diagnostic testing, therapy, and discharge note. That exposes bottlenecks in patient flow, charting, room turnover, and staffing before paid visits start.
3
Payer And Billing Readiness
Billing and Claims Setup
If billing isn’t ready, the clinic can open with full schedules and still run short on cash. This launch driver matters because Year 1 billing and claims processing is modeled at 60% of revenue, and collections can lag visits, so opening-month cash may not match booked volume.
Start Medicare, commercial insurance, and self-pay setup early, then lock in documentation standards, claim submission workflow, denial prevention steps, patient responsibility collection, and a Current Procedural Terminology (CPT) code review for internal workflow only. The key readiness signal is simple: credentialing status, test claims, charge capture, and clean superbill logic are all working before day one.
Build the billing path before first visit
Before opening, verify payer enrollment, benefit checks, front-desk scripts, and who owns each step from checkout to follow-up billing. Map the inputs: payer IDs, fee schedule, superbills, EHR charge capture, denial edits, and payment policy. If any of those are still loose, the clinic can still see patients, but cash strain and rework rise fast.
Confirm credentialing status first
Run test claims before launch
Check charge capture daily
Train staff on patient balances
Fix superbill logic before opening
4
Referral Network Development
Referral Network Setup
A balance clinic can open its doors, but it cannot fill its schedule without referral flow. For this specialty model, physician and partner referrals are modeled at 50% of revenue in Year 1, so the network has to be active before opening, not after. A signed referral path is what turns the clinic from a fixed cost into a usable day-one service.
The launch risk is simple: if ear, nose, and throat, neurology, primary care, audiology, physical therapy, senior community, and fall-risk partners are not sending patients, first visits will lag and treatment plans will convert more slowly. Tracked sources and fast appointment access matter because earlier evaluations are the launch effect that keeps the calendar moving.
Lock referral paths before first visit
Build the referral kit before opening: service criteria, referral forms, response times, and a direct booking path. Add a Google Business Profile and local pages so referring offices and patients can verify the clinic fast. One clean rule helps: every referral source should know who to send, what you treat, and how quickly you can see them.
Confirm partner list and contact owners.
Track every source from day one.
Test intake-to-appointment turnaround.
Match services to referral criteria.
Prepare fast slots for new evaluations.
If these pieces are late, the clinic may still open on schedule, but it opens underfilled. That pushes cash pressure into the first months because the schedule depends on outside senders, not walk-ins alone. Active referral partners are the readiness signal, not a marketing wish list.
5
Operations And Soft-Launch Controls
Soft-Launch Clinic Flow
This is the control that keeps a vestibular clinic opening on time and safe on day one. If triage questions, contraindication screening, and referral paperwork are weak, first visits slow down, treatment plans stall, and avoidable safety issues show up before the schedule is steady.
A soft launch should prove the path from referral to first follow-up with test appointments, because claim status and visit notes need to line up before volume rises. That matters here because Year 1 billing is modeled at 60% of revenue, so messy intake can quickly turn into slower cash and weaker conversion.
Test the intake-to-follow-up handoff
Before full opening, run real test visits and watch the full flow: scheduling, referral source, evaluation time, treatment plan acceptance, patient education, follow-up cadence, and claim status. The readiness signal is a working balance clinic intake workflow from referral to first follow-up, with no safety flags and clean documentation.
Start with service scope, licensed clinical leadership, payer strategy, and referral targets A practical launch plan runs 6–12 months and should cover state licensing, malpractice coverage, HIPAA workflows, electronic health record setup, equipment calibration, and staffing In the Year 1 model, the opening team includes 2 senior vestibular physiotherapists, 1 clinical audiologist, 1 staff physical therapist, and 1 rehabilitation assistant
Plan for 6–12 months, not a quick office opening The real timeline depends on payer credentialing, leasehold improvements, diagnostic equipment delivery, clinician hiring, and billing setup A clinic can look ready before it can bill cleanly, so schedule soft opening only after credentialing status, equipment testing, documentation, and referral intake are working
It depends on state rules, ownership structure, payer contracts, and service mix Many launch plans include medical director or clinical leadership because vestibular care can involve diagnosis, referral triage, testing, rehab protocols, and documentation risk If you offer physician-led specialty evaluation or complex diagnostics, confirm scope, supervision, and credentialing before signing the lease
Payer credentialing, specialized equipment readiness, trained clinician hiring, and billing workflow failures are the common blockers Year 1 revenue assumptions only matter if visits can be scheduled, documented, billed, and collected Treat each blocker as a launch dependency with an owner, deadline, and backup path before committing to a public opening
The first revenue step is referral-driven vestibular evaluations that convert into rehab plans Focus on ear, nose, and throat physicians, neurologists, primary care practices, audiologists, physical therapists, and fall-prevention partners The researched Year 1 model supports about 410 monthly visits at utilization and roughly $696k in monthly revenue before collections timing and payer mix effects
About the author
Simon Reed
Small Business Educator
Simon Reed is a small business educator at Financial Models Lab who helps service business founders understand the numbers behind everyday business ideas. He focuses on pricing and margin basics, common business costs, and the first months after launch, giving readers a clearer view of what it takes to build a healthy business. Simon brings a simple, confident approach that balances optimism with cost-aware planning.
Choosing a selection results in a full page refresh.