How To Open A Fertility Tourism Agency In 3 To 6 Months
To start a fertility tourism agency, validate target destinations and clinics, complete legal and privacy review, set up patient intake, sign referral and travel partners, and test your first lead channel before launch A researched planning assumption is 3 to 6 months, mainly because clinic due diligence, contract review, compliant marketing, and patient workflow setup take time Your first revenue step is usually converting a qualified fertility travel consultation into a paid coordination package or referral-based order In the model, Year 1 order economics use $15,000 IVF AOV, $8,000 egg-freezing AOV, $100,000 surrogacy AOV, and $500 plus 75% commission, so the launch plan must prove trust before volume
Time to Open3-6 monthsLaunch runwayLaunch Sequence4 stagesCompliance firstKey BottleneckTrust gapClinic vettingFirst Revenue StepPaid consultConsult converts
Launch timeline
This short web summary shows the launch plan, and the XLSX export contains the detailed Gantt Chart.
How do fertility tourism agencies get first customers?
First customers for a Fertility Tourism Agency usually come from trust-building channels, not broad ads, so start with educational search content and patient-ready resources like How Much To Start A Fertility Tourism Agency Business?. With a Year 1 model that assumes a $500,000 buyer marketing budget and $400 buyer CAC, lead quality matters more than traffic. Track inquiry-to-consultation and consultation-to-paid-package first, and tie revenue to a paid consultation or coordination package.
Trust first
Publish destination guides
Explain clinic vetting clearly
Use fertility financing content
Run patient webinars
Measure what converts
Track inquiry-to-consultation
Track consultation-to-paid-package
Use niche social proof
Build referral relationships
Can I start a fertility tourism agency from the United States?
Yes, you can start a Fertility Tourism Agency from the United States, but only if contracts, healthcare marketing, privacy handling, referral payments, and patient disclaimers get professional review first; this cost check belongs beside What Are The Operating Costs For A Fertility Tourism Agency?. Keep the agency role clear: coordinate care, travel, and clinic handoffs, but don’t give medical advice unless licensed to do so.
How long does it take to open a fertility tourism agency?
The Fertility Tourism Agency usually takes 3 to 6 months to open. Faster launches work when you keep destinations limited, use founder-led consultations, and start with pre-vetted partners; slower launches happen when contracts, privacy review, clinic credential checks, website content, and lead generation are still unfinished. Don’t open the first month until you can handle consultation, clinic handoff, travel planning, and follow-up.
Fast launch path
3 months is the fast end.
Limit destinations and clinic count.
Use founder-led consultations first.
Pre-vet partners before opening.
What slows launch
6 months is more realistic if legal work lags.
Delay comes from clinic vetting and terms.
Build compliant intake and follow-up workflows.
Open only after lead quality is proven.
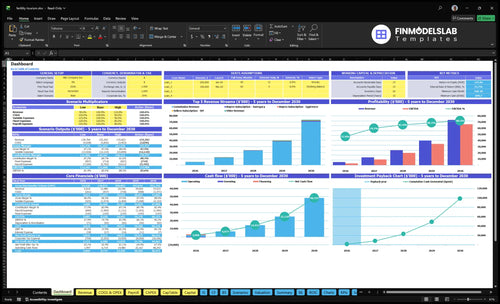
Fertility Tourism Agency Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
Confirm what must be ready before accepting fertility tourism clients
Launch readiness checklist
Use this go-live approval checklist to confirm the business is ready before opening.
1Regulatory
Role boundaries are documentedCritical
The agency must work as coordination and travel support unless licensed otherwise.
Referral disclosures are approvedCritical
Clear disclosures lower risk when a patient is sent to an outside clinic.
Medical marketing claims reviewedCritical
Vague treatment claims can create legal trouble before the first sale.
2Intake
Patient intake form is readyHigh
Intake data should be captured before any clinic handoff starts.
Consent forms are finalizedCritical
Consent protects the agency when patients share health and travel details.
Privacy process is activeCritical
Missing privacy steps can block launch and slow patient intake.
3Clinics
Clinic vetting files are completeCritical
Clinic files should prove quality, scope, and referral fit.
Escalation contacts are listedHigh
Fast escalation paths matter when a patient needs a clinic answer.
Hand-off process is documentedHigh
A clear handoff keeps the clinic, patient, and agency aligned.
4Travel
Travel vendors are contractedHigh
Hotels, transfers, and support vendors must be live before bookings.
Passport and visa checks builtCritical
Timing checks prevent trip delays that can break a treatment plan.
Insurance limits are clearHigh
Patients need to know what the agency does and does not cover.
5Funnel
Consultation script is approvedHigh
The script should set expectations and avoid medical overreach.
Website and CRM are liveCritical
The first revenue step needs working intake, tracking, and follow-up.
Pricing package is publishedHigh
Clear pricing supports the $500 fixed fee plus 7.5% commission model.
6Finance
Runway covers setup periodCritical
The model should show 3 to 6 months of runway before scale.
Year one CAC is testedHigh
Test the $400 buyer CAC and $20,000 provider CAC against launch spend.
Go-live signoff is completeCritical
Launch only when contracts, workflows, vendors, and consultations are live.
What launch drivers decide if the agency is ready?
1Vetted Fertility Clinic Partnerships
6 mo
Documented clinic vetting builds trust and cuts handoff failures with first IVF-heavy partners.
2Compliance And Patient Privacy
Legal gate
Reviewed contracts and privacy rules reduce legal risk and keep marketing claims safe.
3Patient Intake And Qualification
Intake flow
Structured intake turns sensitive inquiries into qualified consultations and cleaner CRM routing.
4Travel Coordination Infrastructure
Ops flow
Repeatable trip planning prevents overpromising and keeps patients clear on what the agency controls.
5Trust-Led Marketing
$400 CAC
Trust-led content fills the funnel, but weak claims can burn the $400 buyer CAC fast.
6Sales-To-Operations Handoff
1st sale
A documented quote-to-handoff path keeps sales promises aligned with delivery capacity.
Vetted Fertility Clinic Partnerships
Clinic Vetting
Vetted clinic partnerships decide whether the business can open on time and look credible on day one. If clinic due diligence, package details, success-rate context, referral steps, response times, and escalation contacts are not documented, early consultations will stall and handoffs will fail. Legal review and privacy workflow are gating items, because the agency needs clear rules on what patient information can be shared.
The first provider mix also matters. Year 1 assumes 70% IVF, 20% egg freezing, and 10% surrogacy, so the launch should start with IVF-heavy partners that can handle the highest share of demand. If overseas approval moves slowly, the launch date slips, and the team cannot route leads, book consults, or answer patient questions with confidence.
Handoff Setup
Before opening, lock the partner file so sales and operations use the same playbook. Here’s the quick check: clinic materials, approved contact names, handoff steps, patient-sharing limits, and escalation paths. That’s what turns a “maybe” partner into a usable launch partner.
Check provider packets and package terms.
Document referral and response times.
Confirm what patients can see.
Assign escalation contacts at each clinic.
Test one full handoff before launch.
What this setup hides: if the clinic won’t approve materials fast, your first consultations may be ready before the partner side is. That creates trust gaps, delayed bookings, and extra manual follow-up right when the team needs a clean day-one process.
1
Compliance And Patient Privacy
Patient Privacy and Compliance
This launch driver protects opening day. If contracts, consent forms, referral disclosures, ads, and disclaimer language are not reviewed before go-live, the agency can blur the line between coordination and medical advice. For a fertility tourism agency, that creates legal risk, slower approvals, and patient confusion before the first booking is even sold.
The core boundary is simple: the agency handles coordination, referral, and travel support unless it is licensed to do more. That scope has to match the CRM, intake forms, website copy, and sales scripts. If one of those says the wrong thing, day-one operations can still be live but not safe to run.
Lock Scope Before Launch
Review the legal and patient-facing flow in this order: contracts, consent forms, privacy handling, referral disclosures, advertising claims, then medical-disclaimer language. The handoff should be clear enough that staff can explain it the same way every time. Here’s the quick test: if a patient asks for medical advice, the script should route them to the licensed clinic, not guess.
Set CRM fields before intake opens.
Limit staff scripts to approved wording.
Document what data you collect.
Define referral fees and disclosures.
Test every disclaimer on mobile.
What this controls: faster approvals, fewer misunderstandings, and less launch delay from last-minute legal edits. The biggest bottleneck is unclear boundaries around medical advice, so fix that before marketing starts. If the privacy workflow is not ready, the agency may have leads, but it will not be ready to handle them safely from day one.
2
Patient Intake And Qualification
Structured Patient Intake
This launch driver matters because it turns sensitive inquiries into qualified consultations instead of loose leads. If the intake is not built before launch, staff waste time on unfit cases, response times slip, and the agency opens with weak conversion from day one.
The intake should capture treatment goals, destination preferences, budget range, timeline, passport readiness, travel companion needs, and partner-clinic fit. Any medical-history review must route to licensed providers and clinics, or the team risks blurrier boundaries, slower handoffs, and avoidable privacy problems.
Build the Qualification Rules First
Before opening, lock the form fields, call script, and CRM fields so every inquiry is screened the same way. Use a simple rule set: collect logistics first, then route medical detail out of agency handling. That keeps the team within its role and prevents over-collecting sensitive data with no clear next step.
Test the workflow end to end: inquiry, qualification, clinic match, and handoff. One clean intake is better than a long form that stalls prospects. If the privacy workflow or clinic criteria are not ready, delay launch rather than opening with a process that cannot support first-revenue consultations.
Capture goals, budget, and timeline.
Check passport and travel readiness.
Record companion and clinic-fit needs.
Route medical history to licensed partners.
Match CRM fields to each intake step.
3
Travel Coordination Infrastructure
Travel Ops Readiness
This launch driver is what turns a sale into a real trip. If appointment timing, passport and visa checks, lodging, transport, companion travel, and emergency contacts are not mapped before launch, the agency can sell work it cannot deliver on day one. That creates delays, bad expectations, and avoidable trip failures.
The key dependency is the clinic’s appointment rules and the patient intake data. Build a repeatable file for itinerary changes, change notices, and escalation, and keep medication logistics inside documented agency boundaries. The risk is simple: do not promise control over travel steps the agency does not control.
Build the trip playbook
Before opening, lock the vendor list, itinerary template, change policy, and escalation workflow. Test them against at least one full sample case so the team knows what gets booked, what gets confirmed, and who acts when a flight, hotel, or clinic slot changes.
Use a clean handoff from intake to travel setup. If intake is missing passport status, travel companion needs, or destination limits, the team will stall after the sale. The fix is to capture those fields up front and route anything medical to the licensed clinic, not the agency.
Confirm clinic date rules first.
Check passport and visa status.
Prebuild lodging and transport options.
Document emergency contacts.
Write one trip-change path.
4
Trust-Led Marketing
Trust-Led Marketing
This launch driver decides whether early traffic becomes qualified demand or just expensive clicks. For this model, $500,000 of Year 1 buyer spend at $400 CAC means every weak message can burn cash fast, so the site needs clear proof before ads start.
That proof has to be ready on day one: destination guides, clinic-vetting pages, transparent process pages, consultation offers, webinars, and claims that have passed compliance review. If those assets are not approved, the launch slips because the team cannot market safely or answer patient doubts well enough to convert.
Approve Claims Before Spend
Build and review the trust stack before paid traffic goes live. Here’s the quick math: $500,000 ÷ $400 CAC = 1,250 potential acquisitions, so the funnel has little room for vague copy or unsupported claims.
Verify every healthcare claim.
Lock clinic documentation first.
Track consultation-to-booking conversion.
Test webinar and referral scripts.
Confirm disclaimer language is live.
The launch risk is not just marketing waste; it is trust friction that lowers lead quality and slows bookings. If the clinic proof, referral process, or consultation path is incomplete, first-day operations will still run, but conversion will be soft and support load will rise.
5
Sales-To-Operations Handoff
Sales-to-Operations Handoff
This launch driver decides whether the first inquiry turns into a paid coordination package or a broken promise. The business can’t open on time if sales is booking work before the path from inquiry to qualified consultation, clinic matching, travel planning, and follow-up is documented and ready to run.
The risk is simple: sales can outpace service capacity. If intake, the clinic network, or travel vendors are not ready, the team will overpromise on timing, support, or scope, and that hurts first-day execution and revenue recognition. One clean handoff path is what keeps the launch realistic.
Lock the Handoff Before Selling
Build the quote template, pricing package, CRM stage rules, follow-up cadence, and handoff checklist before the first paid offer goes out. Test one full case from inquiry to coordination, then confirm the next owner, next step, and approval point at each stage.
Use the checklist to verify intake is complete, clinic fit is approved, and travel vendor options are live before payment. If any step is still manual or unclear, pause the sale. That protects day-one service quality and keeps the launch from slipping while the team fixes avoidable gaps.
Start by proving the workflow before chasing volume Pick one or two treatment categories, vet clinics, complete legal and privacy review, build intake forms, and set up travel vendors Use 3 to 6 months as the planning range In Year 1, test demand against the $400 buyer CAC and $500 plus 75% commission assumption
Plan on 3 to 6 months if you’re building a US-based fertility travel agency with overseas clinic partners The timing depends on clinic due diligence, contract review, privacy workflow setup, and marketing readiness A lean launch can move faster, but only if the first destination, intake script, CRM, and patient handoff are already clear
Medical experience helps, but the safer requirement is clear role control Unless licensed, the agency should provide coordination, referral, and travel support, not medical advice You still need clinic vetting, consent language, privacy practices, and reviewed healthcare claims Medical review should sit with licensed fertility providers and partner clinics
The usual delays are slow clinic vetting, unclear referral contracts, weak privacy processes, and marketing claims that need review Travel vendors are easier to add than trusted fertility clinic partners If onboarding clinics takes longer than expected, the whole 3 to 6 month launch plan can stretch because the intake and handoff process depends on them
The first revenue step is converting a qualified inquiry into a paid consultation or coordination package Do not plan first revenue around high clinic volume The model checks order economics using $15,000 IVF AOV, $8,000 egg-freezing AOV, $100,000 surrogacy AOV, and $500 plus 75% commission, but trust drives the first sale
About the author
Peter Walsh
Launch Planning Specialist
Peter Walsh is a launch planning specialist at Financial Models Lab who helps online business beginners check whether a business idea is financially realistic by breaking down operating cost estimates into clear, practical planning steps. He focuses on opening and running small businesses, and he explains business costs in a helpful, plain-spoken way without unnecessary jargon.
Choosing a selection results in a full page refresh.