How To Open A Medical Simulation Training Business In 4 To 9 Months
Medical Simulation Training Bundle
To open a medical simulation training business, define your target learners, choose the training modality, secure a lab or mobile delivery model, source simulators or VR tools, document curriculum, hire qualified instructors, and sell paid pilots before opening broadly A realistic launch window is 4 to 9 months, but equipment lead times, instructor availability, curriculum approval, and healthcare buyer cycles can stretch that timeline Use researched planning assumptions such as 20 Year 1 billable days/month, 40% occupancy, and a modeled access mix of $115,000/month before custom projects to test launch readiness, not to force a fixed opening date
Time to Open6 monthsSetup windowLaunch Sequence7 stagesMarket firstKey BottleneckVendor setupLead timeFirst Revenue StepPaid pilotBuyer trial
Launch Timeline
This is a short web summary; the XLSX export holds the task-level Gantt Chart and dependencies.
How do you get customers for medical simulation training?
If you’re asking how to get customers for Medical Simulation Training, start with relationship-based B2B sales, not broad ads, and align the spend with the launch math in What Is The Estimated Cost To Open And Launch Your Medical Simulation Training Business?. First buyers usually come from hospitals, nursing schools, EMS programs, allied health programs, and continuing education providers. Sell paid pilots, skills refreshers, onboarding programs, department packages, and custom scenario work; the Year 1 model includes $10,000 in custom scenario projects and up to $115,000/month in subscription potential if access targets are hit.
Target the right buyers
Call hospitals and health systems
Pitch nursing schools and EMS programs
Work allied health programs
Offer continuing education providers
Sell proof first
Start with paid pilots
Package onboarding and refreshers
Sell department-level contracts
Build custom scenarios for $10,000 upfront work
What launch mistakes cause medical simulation center opening problems?
Medical Simulation Training centers usually stumble when they buy equipment before demand, pick a site before learner flow, and open without signed pilot customers or clear safety and privacy rules. 40% Year 1 occupancy is not automatic; it has to be earned. The safest launch move is one paid pilot, one documented curriculum path, and one tested delivery workflow before broad opening.
Common launch misses
Buy gear before demand is proven
Pick site before learner flow
Understaff instructor coverage
Skip maintenance and safety rules
Launch first, then scale
Secure one paid pilot
Document one curriculum path
Test one delivery workflow
Set privacy rules for recordings
How long does it take to open a medical simulation center?
Opening a Medical Simulation Training center usually takes 4 to 9 months. The clock moves with patient simulator procurement, VR platform setup, facility buildout or mobile readiness, instructor recruiting, curriculum validation, and healthcare buyer approval cycles. Here’s the quick rule: sequence market niche first, then modality, site, equipment, curriculum, staff, and pilots, and don’t promise a fixed opening date if approval or contracting slips.
Timing drivers
4 to 9 months is the practical range
Simulator procurement can slow start
VR setup adds build time
Facility or mobile readiness changes the schedule
Launch risks
Curriculum validation can move the date
Buyer approval cycles can take time
Recruit instructors before pilots
Launch only when ready, not early
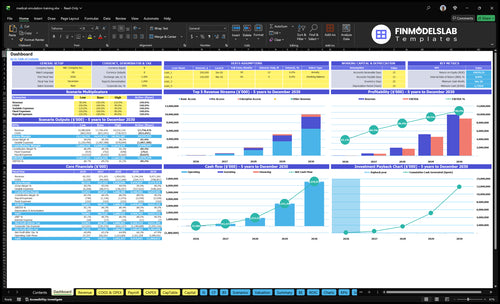
Medical Simulation Training Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
Confirm what must be ready before accepting learners or clients
Launch readiness checklist
Use this go-live approval checklist to confirm the business is ready before opening.
1Compliance
Entity formedCritical
You need a legal entity before contracts, banking, and insurance move.
Insurance boundCritical
Modeled insurance is $1,200/month, so bind coverage before opening.
Local approvals reviewedHigh
Confirm any local operating approvals before you book training time.
Safety policy approvedHigh
A written safety policy lowers risk during learner handling and live sessions.
2Facility / tech
Facility access securedCritical
You need reliable room access for booked sessions and equipment storage.
Equipment inventory loggedHigh
Track manikins, VR gear, and spares before the first class.
Software licenses verifiedCritical
VR and training software must be licensed before learner use.
Maintenance plan documentedHigh
Document cleaning, calibration, and repair steps to avoid session downtime.
3Curriculum
Curriculum files completeCritical
Incomplete files slow delivery and make sessions hard to repeat.
Instructor credentials verifiedCritical
Verify instructor background before they run high-stakes simulations.
Scenario content reviewedHigh
Clinical review helps keep cases realistic and safe.
Assessment rubric setMedium
A clear rubric makes learner results consistent across sessions.
4Staffing
Safety cleaning steps trainedCritical
Cleaning and reset steps protect learners and protect equipment.
Scheduling system liveHigh
The calendar must match available rooms, gear, and staff.
Support coverage assignedMedium
Backup coverage keeps sessions from slipping when someone is out.
Instructor handoffs definedMedium
Clear handoffs reduce confusion between setup, teaching, and reset.
5Sales
Client contract template readyCritical
A clean contract speeds buying and sets session terms early.
Pricing sheet approvedHigh
Pricing must cover staffing, overhead, and equipment wear.
Marketing pipeline activeHigh
You need active leads before the first billable month.
Booking and payment testedCritical
Test the full path so customers can book and pay without friction.
6Finance
Cash runway checkedCritical
You need enough cash to cover setup and the early ramp.
Overhead budget loadedHigh
Use the $12,700/month fixed overhead before salaries as the base test.
Launch model stress testedCritical
Test 20 billable days, 40% Year 1 occupancy, and early pricing.
Go-live signoff completeCritical
Final signoff should confirm compliance, staff, tools, and cash are ready.
Which six drivers decide launch readiness?
1Target Buyer
Named buyer
A named buyer and use case keep the pilot narrow and pricing fit clean.
2Equipment Ready
20 days/mo
Installed, tested equipment keeps the lab usable across 20 modeled billable days a month.
3Credible Curriculum
$50/$150/$400
Qualified instructors and scored scenarios make $50/$150/$400 pricing easier to sell.
4Delivery Setup
Month 1-8
A clear room or mobile flow cuts idle time and helps the opening month run smoothly.
5Safety Protocols
$1.2K/mo
Signed protocols and $1.2K monthly insurance ease institutional approval and lower learner risk.
6Pilot Sales
1 paid pilot
A paid pilot proves demand and gets you moving toward 40% Year 1 occupancy.
Target Healthcare Buyer And Use Case
Buyer and Use Case Fit
This launch driver decides whether the business can open with a real first customer, or just a pile of generic scenarios. In medical simulation, the named buyer, use case, decision maker, training outcome, and pilot scope must be clear before equipment or site spend, or you risk building content no department owns.
Here’s the quick filter: talk to hospital teams, nursing programs, EMS providers, surgical skills labs, allied health programs, or continuing education buyers, then confirm who signs, what skill they want improved, and what a pilot includes. If that chain is vague, opening slips because curriculum, pricing, staffing, and sales all stay fuzzy.
Lock the buyer before the build
Run discovery calls first, then review one sample scenario and test pricing fit against that buyer’s budget path. A simple readiness sign is one department, one owner, and one pilot scope on paper. Without that, you can waste weeks on content that does not convert.
Use a short approval list:
Buyer named and reachable
Decision maker identified
Training outcome written down
Pilot scope agreed in writing
Scenario matches the buyer’s role
That keeps the opening plan tight and helps first-day delivery start with a real client need, not a general demo.
1
Simulation Modality And Equipment Readiness
Equipment Ready to Teach
This driver decides whether you can open on time and run a full training day from day one. The key choice is the modality mix: high-fidelity manikins, clinical task trainers, VR headsets, software licensing, or a blended setup. If the gear is not installed, tested, calibrated, stored, insured, and supported, pilots slip and paid sessions get blocked.
For this business, readiness means the equipment can handle the planned schedule of 20 modeled billable days per month without failures. That depends on vendor ordering, commissioning, maintenance, user training, and a backup workflow. One unusable system can turn a booked class into a refund, a reschedule, or a weak first impression with a hospital buyer.
Lock the setup before you book
Start by matching the modality to the buyer’s use case, then place orders early and get every unit commissioned before sales dates are set. Build a simple readiness file for each item: purchase order, install check, calibration record, storage location, insurance proof, and support contact. Here’s the quick rule: if it can’t run a full session twice in a row, it’s not ready.
Assign one person to test the backup path for each session type, including a spare device, spare login, or alternate scenario format. Train staff on startup, shutdown, cleaning, and reset steps so the room can turn over fast. What this hides: a blended model can help, but only if the team can switch cleanly when one system fails.
Order gear before pilot dates.
Test every workflow end to end.
Document reset and backup steps.
Store and insure all equipment.
Train staff on daily checks.
2
Curriculum And Instructor Credibility
Curriculum and Instructor Credibility
If healthcare buyers do not trust the curriculum or the instructor roster, they will stall the pilot. For medical simulation training, the launch risk is not just content quality; it is whether your scenarios, learning objectives, and debriefing protocol look credible enough for a hospital, school, or EMS buyer to approve use on day one.
The readiness signal is a qualified instructor roster plus documented scenarios ready for pilot delivery. That means each module has medical expert review, competency checks, and client-specific training records in place before the first session, so you do not lose time rebuilding materials after a buyer asks for proof.
Build proof before you sell the pilot
Lock the training package before opening: scenario design, learning objectives, scoring rubrics, debriefing scripts, and feedback forms. Keep each item tied to one buyer use case, so the curriculum feels specific instead of generic. One clean line matters here: if the instructor can’t explain the scenario and score it, the buyer won’t trust the pilot.
Run instructor rehearsal and medical expert review before launch. Use a simple readiness file for each program: scenario version, competency check, debriefing protocol, and training record template. That lowers rework, speeds buyer approval, and keeps day-one delivery from slipping because the team is still editing slides after the pilot date is booked.
Review every scenario with a clinician
Practice instructor delivery before launch
Test scoring before the first pilot
Prepare client-specific training records
Keep feedback forms ready upfront
3
Facility Or Mobile Delivery Setup
Delivery Model Readiness
Your site model can make or break opening day. For medical simulation training, you need a setup that matches actual learner flow, storage, cleaning, accessibility, audiovisual capture, check-in, and reset work, or the first classes will slip and the room will sit idle.
The choice is usually fixed lab, rented training space, onsite client delivery, or a mobile model. Here’s the quick math: if the room, transport, or reset process is not ready, you lose billable days before the first pilot. If you build too much space too early, you tie up cash in capacity you cannot yet fill.
Map Flow Before Fit-Out
Start with the actual day-one workflow, not the floor plan. Verify room layout, equipment transport, cleaning schedule, and scheduling rules before you commit to a lease or vehicle plan. The goal is simple: the next group should be able to enter, train, and reset without a pause that breaks the schedule.
Document learner entry and exit flow.
Test storage, cleaning, and reset steps.
Match setup to pilot size and travel need.
What this estimate hides is the real bottleneck: overbuilding before demand or underplanning onsite delivery. A lean setup with a clear reset process usually opens smoother and keeps idle capacity lower in the first month.
4
Safety, Insurance, And Operating Protocols
Safety, Insurance, and Operating Rules
This driver can block opening if a hospital, school, or agency cannot see clear risk controls. For medical simulation training, the launch package should include waivers or agreements, professional liability coverage, infection control for shared equipment, emergency steps, and rules for recorded-session privacy. The readiness signal is simple: signed procedures instructors can follow.
Modeled insurance is $1,200/month, so this is a real launch cost, not a back-office detail. If the site cannot show client-specific compliance expectations up front, buyer approval can stall, and day-one sessions may be delayed even when the equipment is ready.
Build the safety packet before booking pilots
Put the operating procedure in writing before the first training date. Cover who can run a session, how shared equipment is cleaned, what happens in an emergency, and how recorded sessions are stored and shared. Keep one client version ready for each buyer type, because institutions often want different privacy and compliance terms.
Here’s the quick math: if approval takes an extra 2 to 4 weeks because the risk packet is incomplete, the opening date slips and early revenue slips with it. Assign one owner to collect signatures, confirm coverage, and test the instructor checklist so pilots can start without last-minute changes.
Verify insurance before pilot dates.
Document cleaning and reset steps.
Test emergency response with staff.
Lock privacy rules for recorded sessions.
5
Sales Pipeline And Pilot Contracts
Paid Pilot Before Capacity
For medical simulation training, the launch gate is not the equipment loadout — it is one paid pilot tied to a real buyer problem. If you open with rooms, headsets, or mannequins but no booked training dates, you carry idle capacity, weak cash flow, and no proof that your curriculum solves a clinical need.
The pilot package should include a clear use case, a named department champion, a proposal, a contract, and a signed training date. That is the first signal that the buyer understands the outcome, the schedule fits the calendar, and day-one delivery will not slip because sales was never finished.
Build the Pilot Path First
Start with an outreach list, then use one demo script across every call so the message stays tight. After that, move fast on the proposal and contract, because the real bottleneck is usually buyer approval, not the training itself. One clean pilot beats a full calendar of maybe later.
Before opening, lock the first workshop, the debrief format, and the opening calendar around that date. Verify the buyer’s goal, the number of seats, the training outcome, and who signs. If the pilot is not paid and dated, you do not have launch readiness — you have equipment inventory.
Start with one buyer type and one training use case Pick hospitals, nursing schools, EMS programs, or continuing education providers, then match equipment and curriculum to that need Use 4 to 9 months as a planning window, and test the model against 20 billable days/month and 40% Year 1 occupancy before opening
Most launches should plan for 4 to 9 months The main delays are simulator procurement, VR platform setup, facility or mobile readiness, instructor recruiting, curriculum review, and institutional buyer approval If a paid pilot is not signed, treat the opening date as tentative rather than forcing a full launch
Not always, but clients may require specific standards, documentation, or instructor qualifications Separate business readiness from accreditation Before any pilot, have insurance, safety procedures, curriculum records, instructor credentials, equipment maintenance steps, and privacy rules for recorded sessions Confirm client-specific requirements early
The common delays are equipment lead times, weak curriculum documentation, instructor gaps, and slow healthcare buyer approval A site can be ready while the training offer is not Your safer path is to validate demand first, then align modality, curriculum, staffing, and pilot dates before opening broadly
Sell a paid pilot to a hospital, nursing school, EMS program, or continuing education provider Keep the pilot narrow, measurable, and easy to approve The model’s Year 1 assumptions include $50 Basic, $150 Pro, and $400 Enterprise monthly pricing, plus $10,000 in custom scenario projects
About the author
Grace Hall
Startup Planning Writer
Grace Hall is a startup planning writer at Financial Models Lab, where she creates simple financial projections that help founders make business ideas easier to evaluate. She focuses on the numbers behind everyday businesses, especially for people planning to open a physical location. Grace writes about cost and income assumptions in a clear, practical way, helping readers understand what it really takes to open a business and build a realistic plan.
Choosing a selection results in a full page refresh.