How To Open A Medical Tourism Business In 8 To 16 Weeks
Medical Tourism Bundle
You’re building trust before you ever book a trip, so the launch work starts with niche focus, provider vetting, liability controls, patient intake, and case management This guide covers 8 to 16 weeks of launch execution and uses a 5-year planning model only to test revenue ramp, marketing spend, staffing, and cash runway
Time to Open8-16 weeksSetup windowLaunch Sequence6 stagesNiche firstKey BottleneckVendor setupProvider coverageFirst Revenue StepCoordination depositAfter qualification
Launch timeline
This is the short web summary of the launch plan, and the XLSX export holds the detailed Gantt Chart.
How long does it take to start a medical tourism agency?
Medical Tourism usually takes 8 to 16 weeks to launch, and the clock runs on provider trust, not the website. Weeks 1 to 2 set the niche and compliance plan, weeks 3 to 6 lock in hospitals, specialty clinics, and wellness centers, and weeks 5 to 8 build intake and records flow. By weeks 7 to 12, start patient acquisition, but hold the first case until contracts, consent forms, emergency protocols, and response-time standards are tested.
Launch timing
8 to 16 weeks is practical
Website build is not the gate
Provider vetting takes most time
Package clarity speeds booking
Launch gate
Test contracts before first case
Verify consent and emergency plans
Set response-time standards early
Liability controls must be ready
What are the biggest medical tourism business risks at launch?
The biggest launch risks in Medical Tourism are weak provider vetting, unclear liability, bad emergency planning, and poor aftercare. If treatment packages lack complication protocols, response-time standards, or post-trip follow-up paths, don’t launch yet. The cash risk is also real: Year 1 marketing assumptions total $350,000 across patient and provider acquisition, so slow conversion can drain runway before the network earns trust.
Safety risks
Vet providers with written contracts
Use clear consent forms
Review liability insurance first
Set escalation contacts now
Money risks
Show package pricing clearly
Screen patients before booking
Protect medical record handling
Watch $350,000 in launch spend
How do you get clients for a medical tourism business?
Get clients for Medical Tourism by starting with one procedure niche and one destination message, not a broad marketplace. Build procedure-specific landing pages, plain-English process pages, qualification calls, paid consultations, referral partners, and compliant testimonials where allowed; for startup cost context, see How Much Does It Cost To Open And Launch Your Medical Tourism Business?.
With a $200,000 year-one buyer budget and $400 CAC, you get about 500 buyers if the model holds. At a weighted order value of $20,300, a 12% commission is about $2,436 per order, so the first money should come from a paid consultation or coordination deposit after qualification.
Lead sources
Pick one procedure niche first.
Pick one destination message.
Use qualification calls before booking.
Use referral partners and testimonials.
Offer and math
$200,000 budget can buy 500 buyers.
$400 CAC keeps spend visible.
12% of $20,300 equals $2,436.
Start with a paid consultation or deposit.
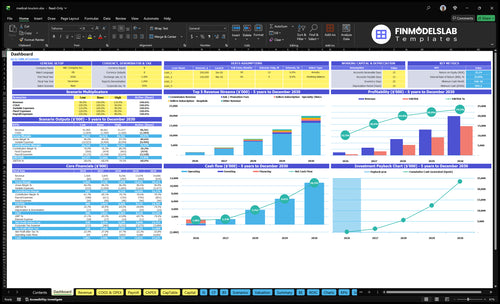
Medical Tourism Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
Confirm the business is ready before accepting patient clients
Launch readiness checklist
Use this go-live approval checklist to confirm the business is ready to open before the launch plan moves into execution.
1Regulatory
Source and destination rules reviewedCritical
Cross-border rules must be clear before any patient or provider contract is signed.
Entity and tax setup completeCritical
The business needs a clean legal and tax base before it books revenue.
Insurance policy boundCritical
Coverage should be active before any patient intake or referral work starts.
Consent forms approvedHigh
Signed consent language protects the business and sets clear patient expectations.
2Providers
Provider contracts signedCritical
No launch should start until providers are under contract and ready to serve.
Credentials verifiedCritical
Verified licenses and physician background reduce patient safety and trust risk.
Complication protocols confirmedCritical
Clear response steps are needed if a patient needs urgent care abroad.
Package pricing approvedHigh
Package prices must be set before marketing and quote work begin.
3Intake
HIPAA-aware intake liveCritical
Health data handling must be privacy-minded before the first lead comes in.
CRM status tracking readyHigh
Case tracking keeps quotes, docs, and follow-ups from falling through the cracks.
Call scripts approvedHigh
Scripts keep the team consistent on scope, pricing, and next steps.
Booking and payment testedCritical
The first revenue path must work end to end before launch day.
4Travel
Lodging and transport setHigh
Patients need a clear travel plan before they commit to treatment abroad.
Translation support arrangedHigh
Language support lowers risk during intake, treatment, and discharge.
Emergency contacts mappedCritical
Fast escalation depends on local contacts and a clear response chain.
Aftercare handoff setHigh
Follow-up care must be assigned before the patient leaves the destination.
5Staffing
Intake staff trainedHigh
Trained intake staff keep lead handling and patient screening consistent.
Case coordination roles assignedHigh
Each case needs one owner so travel, care, and follow-up stay on track.
Provider relations owner namedMedium
A single owner helps keep provider response times and issue handling tight.
Escalation playbook rehearsedHigh
Practice reduces confusion when a patient issue needs fast action.
6Finance
Year 1 marketing budget approvedCritical
Year 1 buyer marketing is planned at $200,000, so spend needs approval first.
Buyer CAC target validatedHigh
Buyer CAC is modeled at $400 in Year 1, so pricing and volume need to support it.
Seller marketing budget approvedHigh
Year 1 provider marketing is $150,000, so the outreach plan needs funding now.
Go-live signoff completeCritical
Launch should not start until contracts, consent, protocols, and staffing are all ready.
Which six launch drivers decide if you’re ready?
1Niche Focus
8-16 wks
A narrow procedure and destination focus speeds trust, pricing, and launch readiness.
2Provider Vetting
$150K / $2.5K
Signed provider terms and tested response times cut referral risk before first patient.
3Compliance Setup
Docs done
Clear consent, privacy, and liability rules protect cash flow when outcomes or cancellations change.
4Intake Workflow
$200K / $400
A tight CRM stops bad leads early and keeps screening from wasting ad spend.
5Travel Handoffs
Playbook
Written travel and aftercare steps reduce handoff risk when flights, lodging, or follow-ups shift.
6Trust Marketing
12% / $20.3K
At 12% commission, a $20.3K weighted order value makes first bookings worth real money.
Treatment Niche And Destination Focus
Narrow Niche, One Destination
One procedure and one destination make the launch workable. Niche choice sets provider vetting, pricing clarity, and patient trust, so if you try to open with every treatment at once, the site copy, quote rules, and case review process keep changing and can push the launch date back.
The Year 1 mix assumes 50% elective surgery at $12,000 AOV, 30% complex treatment at $45,000 AOV, and 20% wellness travel at $4,000 AOV. That blend points to a weighted Year 1 order value of $20,300, but only if the first package, intake path, and destination playbook are fixed before opening.
Lock the first lane
Before launch, choose the first treatment scope, the first country or city, and the exact case filter. Then define the package inclusions, the quote template, and the documents needed to qualify a patient. That keeps the team from building custom workflows for cases you cannot yet support on day one.
Pick one launch package.
Set one qualification path.
Write one destination playbook.
Test provider response times.
Readiness signal: one clear offer, one intake path, and one operating playbook. If that is missing, first bookings become custom work, and custom work slows opening, raises cash needs, and weakens the patient experience fast.
1
Provider Vetting And Contracts
Provider Network Readiness
For medical tourism, the provider network is a launch gate, not a later upgrade. You cannot safely take first bookings until you’ve verified accreditation, physician credentials, response times, complication protocols, patient records handling, package pricing, refund rules, and aftercare handoff.
The Year 1 mix assumes 40% hospitals, 45% specialty clinics, and 15% wellness centers. With a $150,000 acquisition budget and $2,500 seller CAC, that implies about 60 providers if the model holds. If escalation paths are unclear, one bad case can stop bookings fast.
Contract And Handoff Checklist
Before opening, get signed terms and test communication with every provider. The goal is simple: when a patient asks a question, gets a complication, or needs a refund, the team already knows who responds, how fast, and what happens next. That is day-one operating readiness.
Confirm accreditation and licenses
Test response time before launch
Document refund and aftercare rules
Map records handling and handoff steps
Assign escalation owners for each provider
Readiness is not a directory full of names. It is signed contracts plus a tested path from quote to care to follow-up, so the first patient does not expose a broken workflow.
2
Compliance, Liability, And Privacy Boundaries
Compliance, Liability, and Privacy
Medical tourism launch trust depends on clear legal lines. If US patient data is collected, Health Insurance Portability and Accountability Act (HIPAA) exposure starts at intake, so consent, storage, and access rules must be set before the first lead. The platform should say it coordinates care and travel, while licensed clinicians make medical decisions.
One-line test: if staff start explaining treatments, the boundary is too weak. Signed business formation, insurance review, patient agreements, provider agreements, referral reviews, consent forms, and ad review all need to be done before launch, or a complication, cancellation, or bad outcome can turn into a cash and liability problem.
Lock the legal stack first
Before opening, verify the document set, then train staff on approved scripts. The scripts should say what the platform does, what it does not do, and when a clinician must answer. That keeps sales, intake, and support from drifting into medical advice.
Confirm entity and insurance.
Review provider and referral terms.
Set HIPAA-safe record handling.
Approve consent and ad language.
Test scripts on first calls.
Readiness shows up when every patient-facing step has a sign-off path and a named owner. If any agreement is still in review, opening can slip because you cannot safely book, collect records, or take deposits on day one.
3
Patient Intake And Case Management
Patient Intake Workflow
Medical tourism intake has to work before launch, or the team will waste paid leads and miss first-booking revenue. With $400 buyer CAC, every bad screen is expensive, so the business needs a clean path from lead capture to qualification, records, quote, deposit, and status updates on day one.
The key boundary is simple: staff can coordinate logistics, but licensed clinicians must handle diagnosis and treatment advice. A weak handoff can bring in unqualified patients before provider review, which raises refund risk, delays case setup, and can make the launch look unready even if the website is live.
Set Up the Intake CRM
Before opening, build a CRM with intake stages, a document checklist, response standards, and escalation rules. That means one clear path for lead capture, qualification call, medical record collection, provider quote, package explanation, travel planning, deposit, case tracker, and post-trip follow-up.
Test the workflow with real cases and make sure every handoff is assigned. If records are missing or the quote waits on provider input, the case stalls and the team cannot operate from day one. Keep admin work separate from medical advice, and do not move a patient forward until the provider has reviewed the file.
4
Travel Logistics And Aftercare Coordination
Travel Handoff Readiness
For medical tourism, travel support has to work like an operations desk, not a vacation planner. This launch driver covers destination partners, translation help, airport transfers, recovery lodging, local transport, emergency contacts, return-trip timing, and US-based follow-up. If these handoffs are weak, the business can’t safely open on time or handle day-one changes.
It matters more on $45,000 complex-treatment cases than $4,000 wellness trips, because bigger cases need tighter scheduling and cleaner recovery steps. The real readiness check is simple: a written destination playbook, named backups, and tested vendor response times. One missed flight, bad lodging handoff, or late follow-up appointment can break the patient experience fast.
Build the Backup Plan First
Before launch, lock the full travel chain in writing: who books transfers, who handles translation, who confirms lodging, and who owns aftercare coordination after return. Test every vendor with response-time checks, then record escalation rules for flight changes, complications, and appointment shifts. That keeps the launch plan realistic and the first cases movable.
Use a destination checklist with emergency contacts, local transport options, recovery-length guidance, and follow-up timing back in the US. If any partner can’t respond quickly, replace them before opening. The bottleneck is not demand; it’s whether the team can re-route a patient when plans change without delaying care or creating liability.
Write one destination playbook.
Test vendor reply times.
Assign aftercare ownership.
Prebuild flight-change backups.
Confirm return-travel timing.
5
Trust-Based Marketing And First Bookings
Trust First, Book Later
For medical tourism, launch timing depends on whether buyers trust the process enough to pay a consultation or coordination deposit after qualification. With $200,000 in Year 1 marketing and $400 CAC, you’re targeting about 500 acquired buyers, so weak trust pages or unclear claims can burn cash before the first booking.
Here’s the quick math: weighted Year 1 order value is about $20,300, and a 12% commission implies about $2,436 per order. That only works if the funnel is built around procedure-specific education, transparent process pages, and compliant testimonials. Aggressive claims raise legal, refund, and trust risk, which can delay opening and stall day-one revenue.
Build the Deposit Gate
Before opening, lock the path from interest to paid deposit. Verify the education pages, qualification call script, referral partner outreach, testimonial review process, and conversion tracking so each lead has one clear next step. The readiness signal is simple: after qualification, the patient sees one paid consult or coordination deposit.
Use a tight launch checklist and assign owners for each step.
Track source to deposit.
Approve claims before publish.
Test compliant testimonial use.
Review refund language early.
Measure booked calls weekly.
If the funnel is vague, marketing may create leads that never convert, and the team will still need to handle questions, document requests, and payment issues on day one.
Start with one treatment niche, one destination, and a short list of vetted providers Build contracts, privacy-aware intake, liability coverage, destination logistics, and a patient qualification call before marketing A practical launch window is 8 to 16 weeks Use the Year 1 assumptions, including $400 buyer CAC and 12% commission, to test the first revenue plan
Plan on 8 to 16 weeks if the scope is focused The main delays are overseas provider vetting, written contracts, package pricing, language support, and emergency protocols A website can go live faster, but the business should not accept patients until intake, consent forms, provider response times, and aftercare handoffs are ready
Yes, you need vetted providers before taking patient deposits Year 1 assumptions show a provider mix of 40% hospitals, 45% specialty clinics, and 15% wellness centers That mix only works if each partner has clear pricing, credentials, complication protocols, records handling, and written terms Provider readiness is the launch gate
First revenue is delayed when the agency has leads but no safe way to qualify, quote, and coordinate the case The model assumes $200,000 in Year 1 patient marketing and $400 buyer CAC, so weak conversion gets expensive fast The first revenue step should be a paid consultation or coordination deposit after patient qualification
Hire coordinators when founder-led intake starts slowing response times or case follow-up Early launch can stay lean, but complex treatment cases need tighter tracking than wellness travel Use CRM stages, provider response standards, and case volume to time hiring If aftercare, travel changes, or document collection slip, the role is needed
About the author
Liam Foster
Business Idea Researcher
Liam Foster is a business idea researcher at Financial Models Lab, focused on the revenue and profit basics that early-stage founders need when preparing a simple business plan. He helps simplify business plans for non-finance readers by turning business model overviews into clear, practical insights. With a simple, confident approach, Liam breaks down revenue, expenses, and profit in a way that makes financial thinking easier to understand and use.
Choosing a selection results in a full page refresh.