How to Open a Mobile Health Clinic in 6 to 12 Months
You’re launching care on wheels, so readiness matters before the first patient visit This guide covers the 6 to 12 month mobile health clinic launch plan, including compliance, vehicle setup, staffing, vendors, scheduling, partnerships, and first revenue Use the financial model to validate costs, payer mix, capacity, and cash runway before opening month
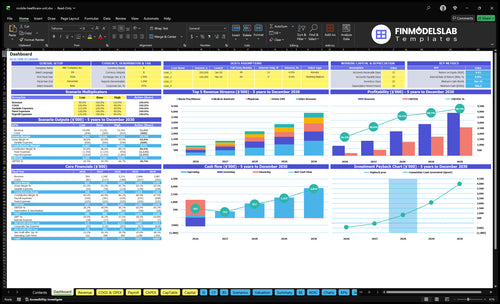
Time to Open6-12 monthsLaunch runwayLaunch Sequence7 stagesCompliance firstKey BottleneckBuildout delayState rulesFirst Revenue StepPartner eventsBooking live
Launch timeline
This is a short web summary; the XLSX export carries the detailed Gantt chart.
How long does it take to open a mobile health clinic?
It usually takes 6 to 12 months to open a Mobile Health Clinic in the US, and the real driver is the launch sequence, not the calendar. Vehicle procurement and custom buildout can happen alongside payer credentialing, but patient care should wait until compliance, staffing, EHR setup, and route testing are ready. A soft launch with limited sites is the safest way to open full routes.
What sets timing
6 to 12 months is the practical range.
Vehicle procurement can take months.
Custom medical buildout adds delay.
Service scope drives licensing and staffing.
What must be ready
Finish state approvals before care starts.
Complete payer credentialing in parallel.
Set up EHR, vendors, and supplies.
Open with limited sites first.
What mobile clinic launch mistakes should you avoid?
Don’t launch a Mobile Health Clinic until payer setup, route testing, HIPAA workflows, clinical protocols, supply controls, and partner agreements are ready. The clean rule is simple: if billing can’t start in the opening month, you’re not ready, and if onboarding takes 14+ days, patient trust and revenue collection both take a hit.
Readiness checks
Confirm payer setup before launch.
Test routes under real drive time.
Verify HIPAA documentation works.
Match supplies to service scope.
Common launch misses
Underestimating drive time.
Skipping medical waste steps.
Missing backup clinician coverage.
Having weak referral sources.
What licenses do you need to open a mobile health clinic?
A Mobile Health Clinic usually needs state healthcare facility approval, licensed clinicians, medical director oversight, malpractice coverage, HIPAA, OSHA, CLIA if testing is done, medical waste compliance, vehicle permits, and local site permission; requirements change by state and services offered, so confirm each item before launch and track outcomes through What Strategies Are You Using To Measure The Success Of Mobile Health Clinic?. The stakes are real: the U.S. Census Bureau reported 26.4 million uninsured people in 2023, so access is urgent, but compliance must be built before the first patient visit.
Core licenses
Check state clinic facility rules
Verify every clinician’s active license
Name a qualified medical director
Secure malpractice insurance before care
Scope triggers
Use CLIA waiver for basic tests
Follow HIPAA privacy rules
Meet OSHA bloodborne pathogen standards
Confirm billing and payer enrollment
Key Takeaways
Lock service scope before buying the vehicle.
Confirm licensing, HIPAA, OSHA, and testing rules early.
Build the vehicle around real clinic workflows.
Book routes, staff, and billing systems before launch.
Service Model and Target Population
Service Scope and Target Fit
Before you buy the vehicle, lock the service model and patient group. A mobile clinic that tries to serve everyone slows licensing, equipment choices, staffing, and payer setup, and that can push opening past the planned date. Pick primary care, preventive care, testing, phlebotomy, or event-based services, then tie that to the geography, route type, and how you get paid.
The readiness signal is a written scope that says who you serve, what care you provide, where you park, and how cash comes in. That one page keeps partner-site approvals cleaner and gives the team a clear day-one workflow instead of a mixed service list that is hard to staff and harder to bill.
Define the launch lane first
Use one service line, one patient segment, and one route pattern at launch. Then match that scope to licensing, equipment, staffing, payer rules, and partner sites before you order or convert the vehicle.
A tight scope lowers the risk of building for services you cannot support yet. It also makes intake, routing, and billing easier to test before opening, so first-revenue visits are cleaner and less likely to stall.
Write the service menu first.
Pick one target group.
Set route geography and parking.
Confirm payment channels before purchase.
1
Regulatory and Compliance Readiness
Compliance Ready
If the clinic starts without state approval, the right licenses, or the right oversight, it cannot legally see patients on day one. This driver covers clinician licensing, medical director oversight, malpractice coverage, HIPAA workflows, OSHA practices, CLIA waiver needs for testing, medical waste handling, and vehicle permits.
Here’s the quick risk: a late discovery that testing, prescriptions, or site rules need extra approval can push the opening date and stall first revenue. One missing permit can turn a ready vehicle into idle cash burn.
Verify Before Launch
Build the compliance file before booking visits: service scope, policies, consent forms, charting rules, emergency steps, and site permissions. Confirm who signs as medical director, who carries malpractice, and which locations allow parking and care delivery.
Use a simple go-live checklist. If testing is included, confirm the CLIA waiver, the federal clearance for some simple tests; if waste is generated, confirm pickup rules; if staff chart in an electronic health record (EHR), test billing workflows too. The modeled system cost is 2% of revenue + $1,000 per month, so a broken launch path hits both timing and cash.
Confirm state rules by service
Lock clinician licenses and oversight
Test consent and charting
Get site and vehicle permits
2
Vehicle, Equipment, and Physical Setup
Vehicle Buildout Fit
A mobile clinic only opens on time if the vehicle works as a clinical operating platform, not just a van. The buildout has to match the service model and patient flow: exam layout, power, refrigeration, water, accessibility, infection control, diagnostics, storage, safety gear, and a maintenance plan. If those pieces are late or mismatched, the launch slips or day-one care breaks down.
The risk is simple: a finished vehicle that cannot support real workflows. That means missed appointments, slower visits, and lost clinic days. Before opening, the team needs procurement, conversion, inspection, equipment installation, route stress testing, and backup power checks done and signed off.
Test Before First Route
Lock the vehicle design to the exact services you plan to deliver, then test it with real patient flow. A clinic that needs refrigeration, water, and diagnostics should prove each system holds up during a full route, not just in the lot. One clean rule: if staff cannot work safely in motion and on site, it is not launch-ready.
Verify exam layout against visit flow
Check backup power under load
Confirm storage and infection control
Run a full route stress test
Document maintenance and inspection timing
3
Staffing and Clinical Operations
Licensed Staff Coverage
Staffing is what turns a finished mobile clinic into a place that can see patients on day one. For this model, the Year 1 plan calls for 1 physician, 2 nurse practitioners, 3 medical assistants, 2 phlebotomists, and 2 Driver EMTs, plus clinic manager, scheduler or biller, and medical director time. If any route lacks licensed coverage, the clinic can’t open on time or bill cleanly.
The key readiness signal is backup coverage for every route. That means each route has a named clinical lead, a driver plan, and a backup if someone calls out. If the team is not credentialed, trained, and assigned by route, the vehicle may be ready but patient flow will stall, documentation will slip, and first-day revenue will be delayed.
Build Route-Level Coverage
Before launch, verify credential checks, scope rules, and who signs off on daily clinical work. Then map each route to specific roles: clinician, phlebotomy, driving, documentation, and closeout. Keep the staffing plan tied to service scope, state rules, and patient throughput so you do not open with a route that looks staffed on paper but cannot actually operate.
Also lock the operating basics: protocols, training, charting rules, and daily handoff steps. If the team does not know who documents, who collects samples, and who handles exceptions, billing gets messy fast. One clean rule: no route opens without a backup clinician and a backup driver plan.
Check licenses before scheduling routes.
Assign one lead per route.
Train on documentation before visits.
Test backup coverage for call-outs.
4
Partnerships, Routes, and Demand
Booked Routes Before Launch
For a mobile health clinic, partnerships are a pre-opening dependency, not a marketing task after launch. You need signed or confirmed access to employer sites, schools, senior centers, nonprofits, local governments, churches, shelters, housing communities, and referral partners before the vehicle rolls out. If those sites are not locked, you can open late or sit on the road with idle route time.
This driver also shapes day-one cash flow. Year 1 utilization assumptions run 70% to 80% by role, so demand has to be booked before scale. Here’s the quick math: no site agreement, no route calendar, no first revenue. A clinic that cannot park, enter, or staff an event on time is not launch-ready.
Lock Sites, Dates, and Access
Verify the basic inputs early: site agreements, route calendars, parking access, outreach scripts, referral workflows, and event staffing. Also confirm the service scope, insurance, and any local permissions, because each partner will ask what care you provide and who is covered. If those pieces are vague, the route plan will slip.
Sequence the work in the right order: confirm the site, then match staffing and supplies, then test the schedule. One clean rule: no confirmed access, no route. That keeps the opening plan realistic and helps first visits happen on day one instead of after a delay.
Get signed site access first.
Map parking and arrival windows.
Set referral and booking workflows.
Staff events to booked demand.
Match routes to 70% to 80% use.
5
Operating Systems, Billing, and Controls
Billing and Control Systems
Day one only works if a completed visit can be scheduled, documented, billed, and reconciled the same day. The core stack is the electronic health record (EHR), scheduling, billing, payer enrollment, consent forms, telehealth support, inventory tracking, route notes, daily closeout, and reporting. If service codes or payer setup are late, you can still see patients but miss revenue.
Here’s the quick math: Year 1 EHR and billing fees are 2% of revenue plus a $1,000 monthly base. That means every $10,000 in revenue adds $200 in variable fees, before the base fee. Clean controls matter because weak claim flow, bad denial handling, or missing daily closeout can turn real visits into delayed cash.
Test the revenue flow before opening
Build the launch sequence around the claim path, not just the clinic day. Verify payer enrollment, service codes, consent forms, and staff charting rules before the first route. Then test one full loop: appointment booked, visit completed, note signed, claim sent, denial routed, payment posted, and inventory updated. If that loop breaks, first-day revenue breaks too.
Confirm payer setup and service codes
Train staff on charting and closeout
Set inventory par levels and reorder triggers
Test denial workflows and payment posting
Match route notes to billed services
What this setup hides is simple: completed care is not collectible until the paperwork, systems, and site workflow all line up. If patient reminders, telehealth support, or daily closeout are weak, no-shows rise, claims slow down, and cash gets tighter in the first weeks.