How do you get patients for an occupational therapy clinic?
If you’re asking how to get patients for an Occupational Therapy Clinic, start with scheduled evaluations and referral paths, not broad awareness. First revenue comes from completed reimbursable visits, and the Year 1 model assumes about 414 monthly treatments with patient acquisition marketing at 80% of revenue. Track referral source, show rate, payer status, and completed visits so you know what actually fills the schedule.
Referral paths
Build physician referrals
Use pediatrician contacts
Call discharge planners
Reach schools and case managers
Track and convert
Log every referral source
Watch show rate
Check payer status
Count completed visits
How long does it take to open an occupational therapy clinic?
Opening an Occupational Therapy Clinic usually takes 4 to 9 months, and the schedule is driven more by dependencies than paperwork. Start legal setup and payer enrollment early, run lease improvements and equipment buys in parallel, and hire before final occupancy so staff can train before first visits. With Year 1 staffing assuming 6 therapists, recruiting timing can move the opening date.
What sets the clock
Payer credentialing can delay opening.
Lease improvements often take weeks.
EHR implementation needs setup and testing.
Referral development starts before day one.
Best sequence
Finish legal setup first.
Run buildout and procurement in parallel.
Hire before final occupancy.
Train staff before first visits.
What launch mistakes create the biggest OT clinic readiness risks?
The biggest readiness risks are opening before credentialing is active, assuming referrals convert right away, and underestimating claim lag; with $1125k monthly non-wage fixed overhead, a $10k Clinic Director salary, and 155% revenue-linked costs, a slow ramp can burn cash fast. Test intake and claim submission before day one, pre-book evaluations, and match staffing to real demand.
Big launch risks
Don’t open before payer status clears.
Don’t count on instant referral conversion.
Don’t hire too late for demand.
Don’t skip front desk training.
Fast risk cuts
Confirm credentialing before launch.
Test intake and claim submission.
Pre-book evaluations early.
Train on plan-of-care documentation.
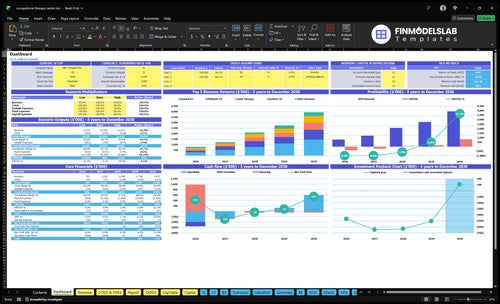
Occupational Therapy Clinic Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
Confirm whether the OT clinic is ready to accept first patients
Launch readiness checklist
Use this go-live approval checklist to confirm the occupational therapy clinic is ready before opening.
1Compliance
State license approvedCritical
No visits should start until the clinic and clinicians are legally allowed to practice.
HIPAA workflow documentedHigh
Privacy, access, and record rules need to be set before patient data is handled.
Liability coverage boundCritical
Coverage should be active before staff treat patients or sign vendor contracts.
Scope rules confirmedHigh
Scope limits protect the clinic from offering services it cannot bill or deliver.
2Facility
Lease work signed offCritical
Incomplete build-out can delay opening and block inspections.
ADA access verifiedHigh
Patients must be able to enter, move, and use the space safely.
Therapy rooms equippedHigh
Each room needs the right tools before the first appointment is booked.
3Systems
EHR configuredCritical
Charting must work on day one or visits and billing stall.
Templates loadedCritical
Missing intake and treatment templates slow notes and claims.
Billing workflow testedCritical
Untested claims create rework and delay cash in Month 1.
Scheduling liveHigh
Patients need a working way to book before the first revenue step starts.
4Staffing
Therapist roster matches Year 1Critical
Year 1 assumes six therapists across five specialties.
Front desk trainedHigh
Scheduling and intake fail fast if the front desk team is not ready.
Assistant support assignedMedium
Assistants need clear coverage so therapists stay on treatment time.
5Payers
Payer enrollment activeCritical
Inactive payer status will block claims and slow revenue.
Claim codes mappedHigh
CPT and payer rules need a clean map before the first claim.
Referral sources confirmedHigh
Opening needs patient sources ready so schedules do not start empty.
6Finance
Cash runway covers Month 37Critical
Minimum cash hits about $90k in Month 37, so runway must cover the ramp.
Overhead budget approvedHigh
Monthly fixed overhead is about $11.25k before clinical wage ramp.
Go-live signoff completeCritical
Open only when licenses, staff, systems, billing, and patient flow are all live.
Which launch drivers decide OT clinic opening readiness?
1Payer Access
4-9 mo
Active payer status decides when visits become billable, so opening can slip without enrollment.
2Clinic Space
ADA-ready
ADA-ready rooms and safe flow cut delays, cancellations, and lease-driven launch drift.
3Licensed Staffing
6 therapists
Licensed coverage across blocks lets you schedule first patients and reach Year 1 capacity.
4Referral Pipeline
414/mo
Scheduled evaluations, not introductions, drive the ramp toward about 414 monthly treatments.
5EHR Workflow
15% fees
Clean intake, notes, claims, and denials reduce rework and keep reimbursement moving.
6Runway Ramp
26 mo
Runway must cover payroll and rent before visits and payments catch up, with breakeven near month 26.
Payer Credentialing And Reimbursement Access
Payer Access Before First Visit
Payer credentialing is a hard launch gate for an occupational therapy clinic because visits are not billable until contracts and enrollment are active. Before scheduling insurance-based evaluations, the team needs National Provider Identifier setup, payer applications, Medicare enrollment where it applies, and a clear read on reimbursement rules and authorization steps.
If this slips, you can open with clinicians and rooms but still have no reimbursable visit path. That slows cash from day one and creates rework on claims. The model also shows why this matters financially: Year 1 billing service fees run at 40% of revenue, so clean payer setup protects early margin and speeds cash conversion from evaluation to claim.
Front-Load Enrollment Checks
Build the payer work plan before opening day, not after referrals start. Confirm the payer list, assign each application owner, track contract status, and test one sample claim flow end to end. The readiness signal is simple: confirmed payer status before scheduling insurance-based evaluations.
Use a launch checklist with authorization workflows, fee schedule review, and claim testing. Keep every payer date, follow-up, and missing document in one tracker. If one contract stalls, you can still open only if you know which visit types are cash-pay or self-pay from day one.
Set up NPI and enrollment first
Map payer rules by visit type
Test claims before first evaluation
Track authorizations and contract dates
1
Compliant Clinic Space And Equipment
Clinic Space Ready on Day One
For an occupational therapy clinic, the space has to match the opening service mix, not a future wish list. If the suite is missing an ADA-accessible entry, parking, signage, evaluation rooms, treatment areas, or safe patient flow from check-in to checkout, opening can slip even when clinicians are hired and referrals are coming in.
The cash side matters too. With $7,500/month rent and $1,000/month utilities, lease and buildout timing hit runway fast. If lease work runs late, credentialed clinicians may be ready but still idle, which pushes back first visits, raises cancellation risk, and leaves the clinic overbuilt before demand proves out.
Match the Buildout to First Visits
Plan the room list from the first billable services you will actually offer. That means evaluation space, treatment space, documentation setup, safety controls, and infection control supplies before any extra equipment. If you offer pediatrics or hand therapy, add only the equipment those visits need now. Readiness means a client can move from intake to treatment without workarounds.
Verify ADA access before lease signing.
Map patient flow from entry to checkout.
Confirm evaluation and treatment room count.
Order only service-specific equipment.
Test safe movement and documentation space.
Track buildout dates against clinician start dates.
Here’s the key test: if the space supports evaluations, treatment, and charting on day one, it’s ready. If not, the clinic may have staff, licenses, and insurance lined up but still miss opening because the suite fails inspection, needs rework, or cannot support safe patient movement.
2
Licensed Staffing And Clinical Coverage
Licensed Clinical Coverage
Without licensed coverage in every scheduled treatment block, the clinic can’t open safely or book day-one visits. The Year 1 plan assumes 6 therapists: 2 General OT, 1 Pediatric OT, 1 Geriatric OT, 1 Hand Therapy therapist, and 1 Ergonomics therapist. If a license, supervision rule, or shift is missing, capacity falls fast and compliant care stalls.
Here’s the quick math: that staffing plan supports about 414 modeled monthly treatments at Year 1 volume. If hiring starts after referrals begin, first-patient scheduling slips, front desk coverage gets thin, and documentation quality suffers because the team is rushed. The real launch gate is licensed time, not just headcount.
Lock Coverage Before Intake
Verify active licenses, supervision rules, and shift schedules before the first evaluation is booked. Then assign front desk coverage, billing support, and utilization targets to each service line so every treatment block has a named owner. Test the path from intake to charting, because a full schedule only works if documentation and billing can keep up.
The readiness signal is licensed coverage during all scheduled treatment blocks. If even one therapist starts late, the clinic may still carry rent and payroll while the 414-treatment plan stays out of reach, so cash needs rise before visit volume does.
Confirm each license status.
Map supervision and backup coverage.
Set schedules by treatment block.
Train front desk and billing handoff.
Test charting before first patient.
3
Referral Pipeline And Patient Acquisition
Referral Demand Before Opening
An occupational therapy clinic can open on time only if referrals are already moving. If clinicians are licensed but the calendar is empty, payroll starts before revenue does, and the clinic misses its day-one operating target.
The real readiness signal is scheduled evaluations, not introductions. This matters even more because the model assumes patient acquisition marketing at 80% of Year 1 revenue and a ramp toward about 414 monthly treatments. One clean booking is worth more than ten warm contacts.
Build the Referral List Before the Lease Starts
Map sources early: physicians, pediatric practices, hospitals, case managers, schools, senior care providers, employer injury programs, workers’ compensation contacts, and local search pages. Assign each source an owner, outreach cadence, and next step so the clinic is not waiting on chance calls after opening.
Test the path from referral to visit. Use discharge planner meetings, school contact mapping, local website pages, and intake scripts to prove a lead can become a scheduled evaluation. If referrals stop at “good conversation,” the clinic may open with licensed staff ready but no demand to fill treatment blocks.
Build source lists by referral type
Set weekly outreach before opening
Book discharge planner meetings early
Publish local pages before launch
Practice intake scripts with mock calls
Track scheduled evaluations as the gate
4
EHR, Intake, Documentation, And Billing Workflow
EHR And Claim Readiness
This has to be live before opening day. In an occupational therapy clinic, evaluations, plans of care, authorizations, coding, claims, and denial follow-up all depend on the EHR. If intake forms, consent, HIPAA workflows, scheduling, and documentation templates are not set, you can still see patients, but you cannot turn that visit into a billable claim cleanly.
The readiness test is simple: a test patient should move from scheduled evaluation to documented claim without manual workarounds. If that path breaks, the clinic opens with rework, slower cash, and higher denial risk. Budget for the system too: $800/month for the EHR subscription plus 15% of Year 1 revenue in transaction fees.
Test The Full Claim Path
Set up the whole workflow before the first appointment. That means intake forms, consent, HIPAA steps, scheduling, evaluation templates, documentation standards, authorization tracking, coding setup, claim submission, and denial management. Assign one owner for each step so the clinic does not rely on memory or ad hoc fixes during week one.
Confirm required fields and templates.
Map prior auth by payer.
Load codes before scheduling.
Test one clean claim end to end.
Document denial follow-up steps.
No clean claim path, no real opening. If a patient can be scheduled, evaluated, documented, and billed in one flow, the clinic is ready to launch without day-one billing chaos.
5
Financial Runway And Visit-Volume Ramp
Visit-Volume Ramp and Runway
This launch driver matters because the clinic can start paying payroll and rent before visits and claim cash catch up. The model shows about 414 monthly treatments across 6 therapists, supporting about $659k/month in modeled revenue, so opening on time depends on having patients, billing, and collections ready at the same time.
Here’s the quick math: the plan ties revenue to treatment count, price, and service-line capacity. If referrals are slow or claim lag stretches out, the clinic can still look “open” but run short on cash. The risky part is not just volume; it’s whether the first weeks produce billable visits fast enough to cover fixed overhead and the $120k/year Clinic Director.
Build the cash bridge first
Before opening, verify the launch runway against the first 60 to 90 days of visit volume, because that is where claim lag and hiring timing usually bite. Confirm payer mix, authorization timing, referral calendar, and staffing start dates before the lease and full payroll lock in. One clean test: can a scheduled evaluation move to a billed claim without delay?
Map monthly visits by therapist.
Track payer status before scheduling.
Model claim lag by payer.
Stagger hires to visit demand.
Watch referral ramp weekly.
Use the model’s revenue-linked costs as a stress test, not a comfort check. The plan lists revenue-linked costs at 155%, so even small delays in collections, denials, or authorization work can widen the cash gap fast. If visits start after payroll, the launch still “opens,” but day-one operations turn into a funding problem.
Start by defining the service mix, then verify state OT board rules, form the business, secure space, set up EHR and billing, and begin payer credentialing The researched Year 1 case uses 6 therapists, about 414 modeled monthly treatments, and roughly $659k in modeled monthly revenue once ramped
Plan for about 4 to 9 months, with payer credentialing and lease readiness usually driving the schedule Business registration may be quick, but hiring 6 Year 1 therapists, setting up billing, and building a referral pipeline take longer Start referral outreach before the opening month
You need active payer access before relying on insurance-based revenue You can open with direct-pay services, but reimbursable evaluations require payer enrollment, authorization workflows, and claim submission readiness In the model, billing service fees equal 40% of Year 1 revenue, and EHR transaction fees add 15%
The common delays are payer credentialing, lease buildout, licensed staff hiring, untested EHR workflows, and weak referral conversion Year 1 fixed non-wage overhead is $1125k/month in the model, plus a $120k annual Clinic Director salary, so delay hurts cash before visits ramp
Book reimbursable evaluations from qualified referral sources, then complete documented treatment visits that can be billed Focus first on physicians, discharge planners, schools, senior care partners, workers’ compensation contacts, and direct-pay niches The Year 1 model assumes 500% to 650% capacity by service line during the launch period
About the author
Charles Bryant
Business Plan Writer
Charles Bryant is a business plan writer at Financial Models Lab who helps founders make sense of startup costs and choose realistic business ideas. He focuses on founder-friendly business numbers, with clear guidance on operating expense planning and startup planning without heavy finance jargon. Charles writes from a practical founder perspective, making complex decisions feel manageable for readers who want useful, realistic insight before they start a business.
Choosing a selection results in a full page refresh.