How To Open An Orthopedic Clinic In The US In 6 To 12 Months
You’re opening a medical practice where the slow parts are usually payer credentialing, clinical buildout, imaging readiness, and staffing This guide covers the orthopedic clinic launch steps from entity setup through first patient revenue, with financial modeling used only to test timing, staffing, revenue ramp, and cash runway The researched planning case assumes 6 to 12 months to open and a Year 1 clinical team starting with 2 surgeons, 4 PAs, 1 radiologist, 3 therapists, and 5 nurses
Time to Open8-12 monthsLaunch runwayLaunch Sequence8 stagesCompliance firstKey BottleneckCredentialing gateApproval pathFirst Revenue StepBooked consultsBooking live
Launch timeline
This is a short web summary of the launch plan, and the XLSX export contains the detailed Gantt chart.
Which launch drivers decide whether the clinic opens on time?
1Payer Credentialing
6-12 mo
Completed enrollment and test claims speed first collections and cut opening-month claim failures.
2Facility Readiness
Buildout ready
Approved rooms, imaging, and patient flow reduce delays and keep providers productive on day one.
3Staff Coverage
2S 4PA 1R
Day-one coverage keeps surgeons from absorbing intake, documentation, and authorization work.
4Billing Setup
18% load
Working templates and claim tests speed cash from the first visits.
5Referral Pipeline
60% Yr 1
Booked referrals before opening help the clinic ramp toward first-year capacity instead of starting empty.
6Compliance Controls
$5K/mo
Privacy, consent, and incident rules cut preventable launch disruptions and keep care safer.
Confirm what must be ready before the first orthopedic patient visit
Launch readiness checklist
Use this go-live approval checklist before opening the orthopedic clinic.
1Clinic clearances
Clinic entity and licenses approvedCritical
The clinic must be legally set up and licensed before any patient care or billing starts.
Physician licenses verifiedCritical
Each surgeon's license and scope must match the services planned at launch.
Malpractice coverage boundCritical
Coverage should be active before the first appointment, procedure, or consult.
HIPAA workflows signedHigh
Privacy workflows must protect patient data from day one.
OSHA controls postedHigh
Exposure controls lower staff risk and support inspection readiness.
2Facility readiness
Lease and buildout approvedCritical
The lease and buildout need signoff before move-in and equipment install.
ADA access confirmedHigh
Patients and inspectors need safe access to the clinic entry and rooms.
Exam rooms clearedHigh
Exam rooms must be ready for intake, exams, and procedures.
Imaging room testedHigh
If imaging is part of launch, the room must pass test use before opening.
3Staffing
Year 1 surgeons hiredCritical
Year 1 staffing assumes 2 surgeons, so clinical coverage must be locked first.
Support staff hiredCritical
The model calls for 4 PAs, 1 radiologist, 3 therapists, and 5 nurses in Year 1.
Payer credentialing completeCritical
Claims cannot start cleanly until payers have approved the clinic and clinicians.
Clinical training completedHigh
Staff need workflow practice before the first patient day.
4Equipment
MRI installed and testedCritical
Major imaging gear must work before clinical scheduling opens.
X-ray ready if offeredHigh
X-ray should only open if imaging is in the launch scope.
Sterile supplies stockedHigh
Cast, brace, and procedure supplies must be on hand before opening.
Cleaning vendor activeMedium
Rooms stay usable only if cleaning follows the opening schedule.
5Patient flow
Referral scripts approvedHigh
Referrals are the first revenue path, so scripts need to be clear and ready.
Scheduling liveCritical
Patients need a live way to book visits and confirm times.
Directories updatedHigh
Insurance directories and online listings help patients find the clinic.
Intake and auth testedCritical
Intake, prior auth, coding, and collection steps must work before claims start.
6Cash and signoff
Billing tests passedCritical
Billing services are modeled at 5% of revenue, so test claims must pass.
Cash covers troughCritical
Cash must cover the Month 25 trough and Month 26 breakeven.
Capacity plan approvedHigh
The launch plan should hold at 60% of Year 1 capacity before opening.
Go-live signoff completeCritical
Final signoff should confirm staff, billing, referrals, and cash are ready.
Want to test the launch plan before signing the lease?
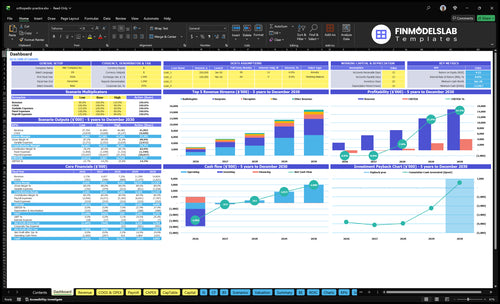
Open the Orthopedic Clinic Financial Model Template; its dashboard and assumptions tabs test launch timing, payer mix, volume ramp, staffing, runway, and break-even. Year 1 at 60% capacity can reach about $228,000/month.
Financial model highlights
60% capacity revenue ramp
18% variable cost load
Runway and break-even path
How long does payer credentialing take for an orthopedic practice?
Payer credentialing for an Orthopedic Clinic usually takes 6 to 12 months in launch planning, so treat it as a sequence, not a guaranteed approval date. Office buildout, leasehold improvements, imaging setup, staff hiring, and EHR billing configuration often decide the open date too. Start credentialing as soon as provider, entity, NPI, malpractice, and location details are set.
What slows it down
Payer contracts must be in place
Provider enrollment can lag
Billing IDs need setup first
Prior auth rules can delay claims
What to line up early
Finish claim testing before opening
Confirm directory listings are live
Plan for revenue lag
Use cash-pay only if compliant
What orthopedic clinic launch mistakes cause opening delays?
If your Orthopedic Clinic opens before the buildout, payer setup, and billing flow are ready, the launch slips fast. The biggest delays come from signing the lease too early, underestimating credentialing time, adding imaging before workflow is ready, hiring too late, skipping test claims, and opening with no cash runway visibility. Here’s the quick math: model 60% Year 1 capacity, $228,000 monthly revenue, and 18% variable expense load, then block launch if any gap stops scheduling, treatment, billing, or follow-up.
Prelaunch blockers
Lease before buildout check
Credentialing takes longer than planned
Imaging added without workflow
Hiring starts too late
Go-live checks
Exam rooms and imaging path confirmed
ADA access, malpractice, and EHR ready
Billing test claims and coding workflow set
Prior auth, referral pipeline, scripts in place
What do you need to open an orthopedic clinic?
To open an Orthopedic Clinic, you need licensed physicians, a compliant entity, National Provider Identifier records, payer enrollment, malpractice coverage, clinical space, EHR, billing, staff, policies, referral channels, and a workflow that passes the full patient journey test; for operating metrics, start with What Is The Most Important Metric To Measure The Success Of Your Orthopedic Clinic?.
Credentialing first, or first visits won’t turn into cash.
Facility flow must match imaging, access, and discharge needs.
Staff coverage and billing setup protect day-one capacity.
Pre-opening referrals prevent an empty schedule on launch.
Payer Enrollment And Credentialing Readiness
Payer Credentialing Ready
Payer enrollment is a launch gate for an orthopedic clinic because patients can show up before the clinic can bill cleanly. If provider enrollment, commercial payer contracts, Medicare participation where relevant, and billing IDs are not finished, opening-day visits can turn into unpaid claims and delayed cash.
The work includes NPI setup, malpractice proof, provider files, location details, fee schedules, payer portal access, insurance directory listings, prior authorization rules, and test claims. In a 6 to 12 month opening window, slow credentialing can push first collections back and raise opening-month claim failures.
Bill Before You Book
Start with the payer list and work backward from the first visit date. Confirm each provider’s entity record, NPI, malpractice documents, and location data are complete, then verify portal access and test claim flow before scheduling opens.
Use a simple readiness check:
Provider enrollment filed
Commercial contracts active
Medicare set, if needed
Prior auth rules mapped
Test claims accepted
If directory listings lag or a payer portal is not live, cash flow slows fast and staff spend opening week fixing denials instead of serving patients.
1
Facility, Imaging, And Clinical Workflow Readiness
Clinic Buildout Readiness
Opening on time depends on more than a signed lease. An orthopedic clinic is ready only when exam rooms, any procedure area, X-ray or imaging flow, cast and brace supplies, sterilization, storage, ADA access, check-in, and discharge all work together for real patient traffic.
Here’s the quick math: fixed facility burn is $19,300/month ($15,000 lease + $2,000 utilities + $1,500 maintenance + $800 cleaning). If imaging, power, shielding, room layout, or inspection slips, the clinic can still pay rent but can’t serve patients cleanly on day one.
Dry-Run Patient Flow
Before opening, map the full path from check-in to discharge and test it with staff, not just contractors. Verify that equipment is installed, rooms are labeled, supplies are stocked, and any imaging or shielding work is signed off before the first appointment is booked.
Use a simple launch checklist: confirm power and imaging setup, stage cast and brace stock, test sterilization, check ADA access, and run one mock patient day. If any step adds delay, the first week will show it as slower visits, more handoffs, and provider downtime.
Lock equipment dates before opening.
Test room flow with staff walkthroughs.
Document inspection sign-offs in one file.
Stage supplies for first-day volume.
2
Provider And Staff Coverage
Provider and Staff Coverage
An orthopedic clinic cannot open on time if the surgeons, PAs, nurses, therapists, and billing team are not already scheduled. Day-one readiness means enough staff to see patients, complete documentation, and keep claims moving, instead of pushing intake and prior auth work onto clinicians.
The staffing plan is clear: Year 1 calls for 2 surgeons, 4 PAs, 1 radiologist, 3 therapists, and 5 nurses. By Year 5, that scales to 6 surgeons, 8 PAs, 3 radiologists, 7 therapists, and 10 nurses. If hiring slips, the clinic may open with lower schedule capacity and slower claims cleanup.
Lock Coverage Before the First Clinic Day
Build the schedule around surgeons or specialists, physician assistants, nurse practitioners where used, medical assistants, radiology techs if imaging is offered, schedulers, and billing staff. Add launch-week training so the team can handle intake, documentation, and authorizations without slowing the visit flow.
Test the first-week roster before opening. If one role is missing, providers end up covering admin work, which hurts patient throughput and claim quality. The cleanest signal is a full coverage matrix for clinic hours, imaging hours, and billing follow-up, with backups listed for every key shift.
Confirm coverage by role and shift.
Train before opening, not after.
Assign billing support on day one.
Stress test intake and claims flow.
3
EHR, Billing, Coding, And Revenue Cycle Readiness
EHR, Billing, And Coding Ready
This matters because orthopedic care can start before the money flow is ready, and that creates a cash gap fast. The clinic needs working scheduling, intake forms, orthopedic documentation templates, diagnosis and procedure coding, prior authorization workflow, claim testing, patient payment collection, and reporting dashboards before first visits. If patients are seen before claims can be coded and sent, cash conversion slows right when launch costs start hitting.
Here’s the quick math: modeled EHR is $1,000/month, billing services are 5% of revenue, and other variable costs add 7% medical supplies, 4% pharmaceuticals, and 2% marketing. That is an 18% total variable load before fixed costs. The launch win is simple: get first visits into clean claims and faster collections from day one.
Test Claims Before First Patients
Set up the revenue cycle in the same order the clinic will use it on opening day: schedule, register, document, code, authorize, submit, collect, report. The key check is whether a real patient encounter can move through the full chain without staff improvising or rework. That is the launch readiness signal.
Verify orthopedic templates before go-live.
Test diagnosis and procedure coding.
Run prior authorization steps end to end.
Submit test claims and fix errors.
Confirm card and patient payment collection.
Review dashboards for daily cash and denials.
If those pieces are not live, the clinic may be open in name but not in billing. That can force delayed submissions, missed charges, and weak early cash flow exactly when the practice needs speed.
4
Referral Pipeline And Pre-Opening Demand
Pre-Opening Referral Pipeline
For an orthopedic clinic, the launch risk is not just opening the doors. It’s opening with staff, rooms, and no booked visits. The first real revenue step is booked consultations from referral partners, urgent injury follow-up, sports medicine demand, and direct scheduling, so outreach has to start before the opening month.
This is mostly a time bottleneck, not a cash one. Modeled marketing is only 2% of revenue, but the founder and providers still have to build relationships with primary care, urgent care, physical therapy, sports, employer injury, workers’ compensation, and hospital contacts. If that work slips, the clinic can open on paper and still miss day-one demand.
Book Demand Before Day 1
Set the referral plan before the buildout is done. Verify who owns each channel, what message they send, and how every lead lands in the schedule. In plain terms: make sure a partner can send a patient and that patient can book fast.
Active outreach to referral sources
Open online scheduling early
Complete local search profiles
Finish insurance directory listings
Track booked consults weekly
The goal is simple: have first appointments lined up so the clinic can move into a stronger 60% Year 1 capacity ramp instead of starting with empty time slots.
5
Compliance, Malpractice, And Opening Controls
Compliance and Opening Controls
An orthopedic clinic can’t open safely if HIPAA, OSHA, malpractice coverage, and state board rules are still loose. The real launch risk is treating patients before consent, prescription, sharps, incident, and record-retention rules match the care model. With modeled malpractice insurance at $5,000/month, weak controls can turn a normal opening into an avoidable cash and legal problem.
Here’s the quick check: who can access records, prescribe, approve procedures, handle sharps, report incidents, and talk with referral partners? If those roles are unclear on day one, staff will improvise, and that’s where delays, exposure, and documentation gaps start. One clean one-liner: no policy match, no patient flow.
Lock Down Day-One Rules
Before opening, confirm the clinic has written controls for privacy, exposure handling, informed consent, incident reporting, and document retention. Train every role before schedule load starts, not after. If the care model includes procedures, make sure approval steps, consent forms, and referral communication paths are tested in advance.
Use a simple access map so each person knows their lane. Confirm record access, prescribing rights, procedure approval, sharps handling, and incident reporting in writing. If onboarding takes longer than planned, delay first patients until training and policy sign-off are complete; otherwise, launch-day errors become compliance events.