How to Start a Pharmacovigilance Service in 8–16 Weeks
You’re building a drug safety monitoring business where trust comes before sales This 5-year launch plan covers PV service setup, SOPs, safety database readiness, staffing, first clients, and a model check using $1248 million Year 1 revenue and Month 19 breakeven assumptions
Time to Open8-16 weeksSetup windowLaunch Sequence7 stagesScope firstKey BottleneckSafety workflowAudit-ready docsFirst Revenue StepPilot contractRetainer live
Launch timeline
This is a short web summary of the launch plan, and the XLSX export contains the detailed Gantt chart.
What launch mistakes create the biggest PV service risks?
The biggest launch risks for a Pharmacovigilance Service are weak SOPs, unvalidated workflows, unclear sponsor-versus-vendor reporting ownership, and undertrained case processors. If onboarding takes 14+ days without clear workflow ownership, churn and audit risk rise, so fix mock case processing, escalation tests, seriousness review, follow-up documentation, access control, and vendor file completion before live cases.
Main launch risks
Weak SOPs slow decisions
Unvalidated workflows create errors
Unclear ownership delays reporting
Poor data security raises exposure
Readiness checks
Run mock case processing
Test escalation paths
Review seriousness assessments
Verify backup reviewers and files
How do you get first pharmacovigilance clients?
First clients usually come from small biotech sponsors, emerging pharma companies, and CRO overflow, not broad outreach. The fastest close is a pilot or audit-ready proof package around Basic Monitoring at $4,500 per month, and you can anchor the sales talk with What Are The 5 KPIs For Pharmacovigilance Service Business?.
Best first buyers
Small biotech sponsors need speed.
Emerging pharma needs compliance help.
CRO overflow needs backup capacity.
Literature monitoring sells as a retainer.
Offer and proof
Basic Monitoring: $4,500 monthly.
Professional Suite: $11,000 monthly.
Enterprise Platform: $24,000 monthly.
Year 1 budget: $250,000; CAC: $12,500.
Trust signals matter in the first sale: SOP index, validation summary, training matrix, security controls, sample metrics, and named medical review coverage. At a $12,500 CAC, the Year 1 budget of $250,000 supports about 20 clients if acquisition stays on plan.
Sales motion
Lead with a pilot.
Show audit-ready documents.
Offer case processing support.
Use analytics add-on at $3,500.
Buyer hooks
Sell retainers for literature monitoring.
Bundle professional services next.
Position enterprise for scale.
Start with one product, then expand.
How long does it take to start a pharmacovigilance service?
A Pharmacovigilance Service usually takes 8–16 weeks to launch, and it moves faster when the scope is narrow, like literature monitoring or case processing support. If the safety database is already set up and SOP approval, staff training, medical reviewer availability, client audits, contracts, and test-case validation are lined up, you can stay near the low end. In month 1, plan for payroll, fixed expenses, cloud hosting, data fees, and the software stack.
Fast launch path
8–16 weeks is the practical range.
Narrow scope starts faster.
Use literature monitoring first.
Use case processing support first.
What slows setup
Validated software adds time.
Vendor qualification adds time.
Security review adds time.
Sponsor audit prep adds time.
Month 1 cost setup
Payroll starts in month one.
Fixed expenses start in month one.
Cloud hosting starts in month one.
Data fees and software stack start early.
Planning checks
Approve SOPs before launch.
Book reviewer time early.
Lock client contracts early.
Validate test cases before go-live.
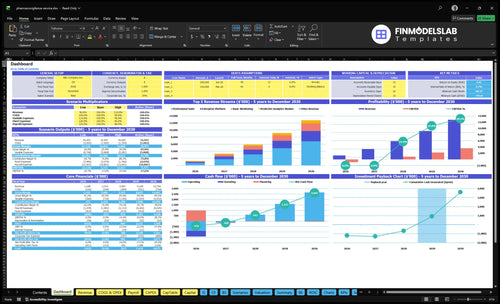
Pharmacovigilance Service Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
Confirm what must be ready before accepting live cases
Launch readiness checklist
Use this go-live approval checklist to confirm the service is ready before opening.
1Legal
Entity registeredCritical
The legal entity must exist before contracts, invoices, and filings start.
MSA and SOW signedCritical
Signed terms define scope, timelines, and liability before work starts.
SOPs and QMS approvedCritical
SOPs and the quality system keep intake, review, and escalation consistent.
2Safety
Safety database validatedCritical
Validation proves the safety database can hold case records without errors.
Case intake testedHigh
Test cases show intake works before real adverse event reports arrive.
FDA timelines mappedCritical
A reporting matrix cuts missed deadlines and late safety submissions.
3Security
Security controls documentedHigh
Security proof matters because case data is sensitive and regulated.
Vendor access approvedHigh
Only approved vendors should touch data or reporting workflows.
Audit file createdHigh
An audit file shows who changed what and when.
4Staff
PV staff trainedCritical
Trained staff reduce case errors and missed adverse-event reviews.
Medical review coverage setCritical
Medical review coverage keeps clinical decisions from stalling.
Backup reviewer assignedHigh
Backup coverage limits downtime if the lead reviewer is out.
5Revenue
Pricing packages setHigh
Pricing must cover the service mix and support sales deals.
Sales pipeline qualifiedHigh
A real pipeline proves launch demand beyond internal plans.
Sponsor roles confirmedCritical
Clear sponsor roles prevent gaps on data, timelines, and approvals.
6Cash
Cash runway reviewedCritical
Cash must cover build, payroll, and slow client onboarding.
Spend plan approvedHigh
The spend plan keeps capex and overhead within the model.
Go-live signoff completeCritical
Final signoff confirms the service can open with known risks.
Which launch drivers matter most before go-live?
1Quality System
Audit gate
Usable SOPs and training records cut audit delays and make sponsor onboarding cleaner.
2Safety Database
Validated DB
Validated workflows and access controls reduce rework and speed sponsor review at go-live.
3Staffing Plan
1 FTE + backup
Trained reviewers and backup coverage keep time-sensitive cases moving without missed approvals.
4Intake Workflow
Live flow
Clear intake, triage, and reporting steps prevent missed cases and reporting gaps.
5Client Contracts
$250K budget
Defined offers and contracts turn audit-ready capability into first retainers and service revenue.
6Audit Security
Trust gate
Security controls and audit files shorten vendor reviews and build buyer trust.
Compliance and Quality Management System
Quality System Ready
A pharmacovigilance quality management system is what tells sponsors and audit teams you can run safely from day one. If SOPs, training records, deviation handling, and quality review steps are not usable, the team may have policies on paper but no real operating control.
Build this before opening, not after. The key dependency is compliance content before staff training, because training on draft rules creates rework and gaps in case processing standards. Weak execution here usually shows up as audit delays, slower client onboarding, and more back-and-forth when a sponsor asks how work is controlled.
Build the SOP Base
Start with an SOP library, document control, a CAPA process, a training matrix, quality metrics, and clear escalation rules. Those inputs set the baseline for day-one operations, because they define how cases are handled, reviewed, corrected, and signed off. If the written process does not match daily work, the quality system will not hold in an audit.
SOP library for core workflows
Document control for version tracking
CAPA for corrective actions
Training matrix for role coverage
Quality metrics and escalation rules
Use a short oversight cadence from the start so issues surface early, not after a sponsor review. What this setup hides is the time cost of fixing policy gaps after training begins; that is when onboarding slows and the opening date starts to slip.
1
Validated Safety Database
Validated Safety Database
A pharmacovigilance safety database has to be ready before first case intake, because it drives case capture, processing, report formats, access control, and traceability. If those workflows are not validated, the team cannot trust the system for sponsor-facing adverse event work, and opening slips while people rework outputs during review.
This launch driver covers database selection, configuration, validation scripts, user acceptance testing, data migration rules, and reporting workflow checks. The bottleneck is unvalidated adverse event reporting software: it can look ready in a demo, but still fail on audit trail, access rights, or report output when the first client sends live cases.
Validate Before Any Live Case
Lock the workflow map first, then test the database with sample cases from intake to submission. User roles, backup procedures, and report outputs should all be signed off before go-live, so the first day is about service, not fixes.
Load migration rules before any client data.
Match reports to sponsor templates.
Test outage backup and restore steps.
Keep test cases and approvals together.
If validation evidence is thin, sponsor review usually slows down and the launch team gets pulled into rework. That hurts first-day capacity, delays case processing, and can push the first billable month to the right.
2
PV Staffing and Medical Review Coverage
Medical Review Coverage
Day-one coverage is the gate here. This launch depends on trained case processors, quality reviewers, a Pharmacovigilance Director, and medical reviewer backup, so the business can’t open safely if any of those roles are still informal. With a $165,000 annual Director and a $115,000 Customer Success Engineer starting in Month 1, base payroll is about $280,000 per year, or $23,333 per month before overhead.
The risk is simple: time-sensitive cases with no qualified reviewer can stall reporting, slow client onboarding, and hurt credibility on day one. The launch plan needs named people for primary review, backup review, training records, and quality sign-off. If those assignments are missing, the service may be technically open but not actually able to process cases at the speed clients expect.
Set coverage before go-live
Lock the hiring plan, role definitions, and backup coverage before the first client starts sending cases. The founder should confirm who does first review, who does quality review, who covers the Pharmacovigilance Director, and who steps in when a medical reviewer is unavailable. That keeps the launch from being delayed by one absence or one unfilled seat.
Document onboarding, training records, and quality review assignments in a simple matrix. Test the handoff with at least one mock case so the team proves it can move from intake to qualified review without delay. The real readiness check is not headcount alone; it is whether the team can clear cases on time with no gaps in oversight.
Assign primary and backup reviewers.
Record training before first case.
Test medical review handoffs early.
Track coverage for urgent cases.
3
Case Intake, Triage, and Reporting Workflow
Case Intake and Triage Workflow
This driver decides whether adverse event cases move from inquiry to live operations without gaps. If intake channels, seriousness assessment, follow-up, duplicate checks, and quality review are not documented, the team can miss cases, miss deadlines, and slow sponsor reporting on day one.
The key dependency is a validated database plus SOPs. If ownership for the FDA adverse event reporting timeline is unclear, the launch can stall in handoff and query loops, which pushes back first-day capacity and raises compliance risk before the service is stable.
Set the intake path before go-live
Before opening, lock the intake forms, mailbox or portal setup, triage rules, sponsor handoff, and query tracking. Then run mock case tests so the team can prove the workflow works with real case volume, not just in a checklist.
Assign one owner for expedited or periodic reporting support and write the escalation step for any serious case. A clean handoff cuts rework, keeps staffing focused, and protects launch timing when the first live cases arrive.
Confirm case intake channels
Test duplicate check logic
Document reporting ownership
Review failed handoff points
4
Client Acquisition and Contracts
Client Acquisition and Contracts
This launch driver decides whether the firm can open with paid work or just a pitch deck. For pharmacovigilance, defined offers, a target sponsor list, an MSA (master service agreement), SOW (statement of work), service levels, and audit proof must be ready before outreach turns into revenue.
The Year 1 price points are $4,500 monthly for Basic Monitoring, $11,000 for Professional Suite, $24,000 for Enterprise Platform, and $3,500 for the analytics add-on. With a $250,000 marketing budget and $12,500 CAC, the plan only supports about 20 customers if spend converts as assumed. No contract pack, no launch-day cash.
Pre-Launch Contract Setup
Before opening, lock the sellable package first: what each tier includes, who approves scope changes, and what evidence proves audit readiness. That means a clean sponsor list, pricing sheet, redline-ready MSA and SOW, plus service-level terms for case turnaround, reporting, and escalation. Otherwise, sales calls create custom promises that slow launch and risk compliance gaps.
Sequence the work so the first close can move straight into onboarding. Verify the audit file, assign one owner for contract edits, and test the handoff from signed SOW to service delivery. If a sponsor asks for proof you cannot show, the sale slips and the first revenue becomes outsourced pharmacovigilance work or pilot retainers instead of a standard subscription.
Confirm offer scope before outreach.
Prebuild MSA and SOW templates.
Attach audit proof to each proposal.
Set service levels and escalation rules.
5
Audit Readiness and Data Security
Audit Proof and Data Security
For a pharmacovigilance service, this is what gets you past buyer due diligence and into contract close. If a sponsor cannot see a vendor qualification file, training records, access controls, and an audit response owner, sales can stall even if the platform works.
Here’s the quick math: $4,200 per month for cybersecurity and insurance plus $6,500 per month for regulatory compliance audits equals $10,700 per month of launch spend tied to trust and control. What this estimate hides is the time cost of weak evidence; a failed sponsor vendor assessment can push opening risk into the sales cycle and delay first revenue.
Build the Audit Binder Early
Before launch, lock the proof set: security review, vendor risk assessment, audit binder, incident procedure, permission testing, secure data handling, and backup procedures. One clean binder can cut review back-and-forth and shorten the path to approval.
Assign one owner for audit replies and make sure the file shows who approves access, how incidents are handled, and how backups are tested. If onboarding takes longer than planned, the buyer still sees control, not risk. That keeps day-one operations credible while the sponsor checks the file.
Start with service scope, SOPs, validated safety workflow, trained staff, and first-client proof A practical launch range is 8–16 weeks The model assumes Year 1 revenue of $1248 million, Year 1 marketing of $250,000, and breakeven in Month 19, so validate sales timing before hiring too far ahead
Plan on 8–16 weeks before handling live adverse event cases The main delays are SOP approval, database validation, staff training, medical reviewer coverage, and sponsor audits Financially, Month 1 already carries payroll, software, cloud hosting, and $34,500 in fixed monthly expenses before marketing
You can use outsourced medical reviewers if responsibilities, turnaround times, training, and quality review are documented That is often safer than overhiring before volume is proven The staffing plan already includes a Pharmacovigilance Director at $165,000 annually, so outsourced review can fill gaps while demand builds
Validation and audit evidence usually delay launch more than sales materials Weak SOPs, missing test cases, unclear FDA reporting support, and incomplete data security files slow client approval The model’s cash low point is -$764,000 in Month 19, so delays can hit runway right when breakeven is expected
Sell a narrow pilot before pitching a full-service contract Good first offers include Basic Monitoring at $4,500 per month, Professional Suite at $11,000 per month, or a case processing retainer Use audit-ready SOPs, validation notes, training records, and response-time commitments as proof, not broad claims
About the author
Grace Hall
Startup Planning Writer
Grace Hall is a startup planning writer at Financial Models Lab, where she creates simple financial projections that help founders make business ideas easier to evaluate. She focuses on the numbers behind everyday businesses, especially for people planning to open a physical location. Grace writes about cost and income assumptions in a clear, practical way, helping readers understand what it really takes to open a business and build a realistic plan.
Choosing a selection results in a full page refresh.