Residential Treatment Center clients usually come from referral relationships, not ads alone, so the fastest path to census is steady intake from hospital discharge planners, therapists, psychiatrists, intervention professionals, employee assistance programs, payer case managers, and private-pay inquiry channels. For operating cost context, see What Are Residential Treatment Center Operating Costs?; with 17 rooms and 45% Year 1 occupancy, early admissions have to be qualified and available, not just numerous. Every referral still needs clinical screening, admission-criteria review, payer authorization or a private-pay agreement, and bed availability, and Year 1 marketing plus referral spend is modeled at 8% of revenue while staying compliant with healthcare rules.
Best referral sources
Hospital discharge planners
Therapists and psychiatrists
Intervention professionals
Employee assistance programs
Admission must pass checks
Clinical screening first
Match admission criteria
Confirm payer or private-pay
Check bed availability
What mistakes delay opening a residential treatment center
The biggest delays come from leasing or buying a site before zoning and the license path are confirmed, then opening with no staff, policies, EHR, or payer setup ready. With a 17-room lease and $70,500 in monthly fixed costs, every month before admissions starts burns cash fast, so model 45% Year 1 census, not full occupancy. Clear inspection gaps, recruit leadership early, and don’t market a start date until referrals and payers are ready.
Main delay mistakes
Pick the site before zoning
Underestimate licensing time
Hire leadership too late
Write weak clinical policies
Launch blockers to clear
Test the facility for inspection
Build medication workflows early
Set up the EHR before opening
Confirm payer and referral readiness
How long does it take to open a residential treatment center
A Residential Treatment Center usually takes 9 to 18+ months to open, and it can run longer if the building needs major life-safety work or the state review queue is slow. The critical path is site selection, zoning, renovation, clinical policies, license application, inspections, hiring, payer setup, and referral readiness; if onboarding drags, first admissions slip and cash runway tightens.
Open faster
Lock site and zoning early
Finish life-safety work first
Submit license papers on time
Start payer and referral setup early
Plan capacity
Use the 17-room capacity plan
Model a 45% Year 1 ramp
Hire for ramp, not day one full occupancy
Protect cash if admissions start slow
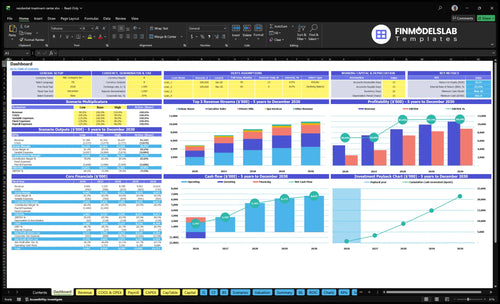
Residential Treatment Center Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
Confirm the center is operationally ready before accepting residents
Launch readiness checklist
Use this go-live approval checklist to confirm the center is ready before opening.
1Licensing
State license approvedCritical
No resident can admit until the state license is active.
Policies and procedures signedHigh
Staff need one approved playbook for care, safety, and escalation.
Staff credentials verifiedCritical
Licenses and certifications must match the roles on site.
Incident reporting rules loadedHigh
A clear reporting path protects residents and the license.
Renewal tracker setMedium
Missed renewals can stop admissions later.
2Facility
Zoning and occupancy clearedCritical
The site must allow residential treatment use before opening.
Fire and accessibility passedCritical
Safety and access issues can block the first resident.
Security system installedHigh
Locked entry and monitoring help protect residents and records.
Medication storage lockedCritical
Controlled meds need secure storage from day one.
3Vendors
Clinical vendors contractedHigh
Food, supplies, and support vendors must be in place before go-live.
Food supplier lockedHigh
Meal service needs a steady source on day one.
EHR workflows configuredHigh
Notes, logs, and charts must work before intake.
Housekeeping service readyMedium
Clean rooms and common areas are part of treatment.
4Staffing
Medical director onboardedCritical
Clinical oversight has to start with a named owner.
Therapist coverage staffedCritical
Therapy hours need to match the resident load.
Nurse schedule filledCritical
Medication and monitoring need nursing coverage.
Direct-care shifts coveredCritical
Unfilled shifts create safety gaps and bad handoffs.
5Admissions
Admissions criteria approvedCritical
Clear criteria keep unsuitable residents out.
Referral pipeline documentedHigh
You need a compliant source of first residents.
Payer verification liveHigh
Coverage checks and authorizations must happen before admission.
Private-pay packet readyMedium
Self-pay terms should be signed before arrival.
6Cash
Room count matches 17 roomsCritical
The model assumes 10 deluxe, 5 executive, and 2 villa rooms.
Year 1 occupancy setCritical
The plan uses 45% occupancy in Year 1.
Monthly fixed costs loadedCritical
The model carries $70,500 a month in fixed expenses.
Clinical payroll matches modelHigh
Therapist, nurse, and support staffing must tie to the forecast.
Cash runway covers launchCritical
Minimum cash hits $662k in Month 5, so opening needs that buffer.
Want the six launch drivers that decide opening readiness
1Licensing Path
License gate
No license, no admissions; clear approval path cuts rework and keeps opening on track.
2Facility Readiness
17 rooms
Written zoning and life-safety approval protects the opening schedule and avoids idle lease burn.
3Clinical Policies
Care rules
Clear care rules speed review, reduce admission confusion, and build trust with referrers.
4Staffing Model
24/7 cover
Hired leadership and 24/7 coverage let first residents enter safely without last-minute recruiting.
5Referral Pipeline
45% Y1 occ
Active referral and payer workflows turn licensed beds into qualified census faster.
6Cash Runway
$70.5K/mo
Working billing, supply, and cash tracking limit early burn while census ramps.
Licensing and Compliance Path
Licensing Path
Licensing is the first go/no-go gate. A residential treatment center cannot admit residents until the state license category matches the facility type, resident acuity, bed count, medication handling, and any payer standards. If you sign a property first and the use does not fit the license, you can lose time, trigger redesign work, and burn the $45,000 monthly facility lease before day one.
The readiness signal is simple: confirmed license category, complete application checklist, policy package, staff credential map, inspection plan, and renewal calendar. That mix keeps opening tied to the approval path, not to guesswork. With 17 rooms and $70,500 in monthly fixed expenses, even a short delay pushes cash pressure up fast.
Sequence the approval work first
Start with state research, then lock the license path before lease signing, buildout, or hiring. Put the application, policies, insurance review, and inspection booking on one owner and one timeline so nothing sits half done.
Verify these inputs early:
Facility type and allowed use
Bed count and resident acuity
Medication storage and handling rules
Staff credentials and coverage map
Inspection timing and renewal dates
When the license file is clean, inspections move faster and you cut rework. That matters because opening with empty rooms still means paying fixed costs, and Year 1 occupancy is only 45%, so the first admit date drives the whole ramp.
1
Facility, Zoning, and Life-Safety Readiness
Facility and Life-Safety Readiness
The property can stop the opening clock. This center can’t admit residents until the site matches local zoning, the occupancy approval path is clear, and fire and life-safety items pass review. For a 17-room facility with a $45,000 monthly lease, every delayed month means real cash burn before first revenue. One bad site choice can force redesign, reinspection, and lease drag before day one.
This driver covers room mix, kitchen readiness, medication storage, security, utilities, accessibility, and maintenance coverage. The opening risk is simple: renovating before confirming allowed use. That’s how operators end up with a finished space that still fails code. Here’s the quick math: 1 month of delay = $45,000 in idle lease cost, before payroll, supplies, or inspection fixes.
Verify the Site Before Buildout
Start with written clearance, not design work. Confirm zoning approval, occupancy path, and state facility rules before you spend on buildout. Then lock the inspection punch list, resident safety review, and vendor access plan. That sequence cuts rework and helps the team open with the right room setup, safe storage, and working utilities from day one.
Confirm allowed use in writing.
Match room mix to rules.
Test fire and life-safety items.
Check accessibility and egress paths.
Map medication and security storage.
Schedule utility and maintenance coverage.
Use a punch list before moving in furniture. If the kitchen, storage, or fire systems fail late, the opening slips and residents can’t be served safely. Keep vendors on site windows, track fixes by date, and recheck every item that affects occupancy approval. That keeps the launch tied to real readiness, not a hopeful finish date.
2
Clinical Program and Policies
Program and Policy Readiness
Clinical program design is the day-one proof that the center knows who it treats and how care will run. That means clear admission criteria, level-of-care rules, treatment schedules, documentation rules, crisis steps, medication management, discharge planning, and quality review. If these are vague, admissions stall and reviewers can push back before opening.
This work has to fit the license category, staffing coverage, payer expectations, and referral standards. In a residential setting, weak policies can slow inspection review, confuse staff, and weaken trust with referring clinicians. Safer care and cleaner records start here, not after the first resident arrives.
Lock the Care Playbook
Before opening, verify the full pathway from intake to discharge: who gets admitted, what care they receive, how often they are seen, what gets documented, and when escalation happens. Build the resident handbook, incident response steps, and audit process together so staff use one set of rules from day one.
Test the policy package against real cases, not theory. Confirm medication handling, crisis coverage, and handoff rules work with the actual staffing plan. If policies take too long to approve or are hard to follow, opening slips and first-day operations turn messy fast.
Define admission criteria clearly
Map level of care
Write crisis protocols
Set discharge triggers
Assign quality oversight
3
Qualified Staffing Model
Qualified Staffing
Staffing is what lets a residential treatment center admit safely on day one. You need 24/7 coverage, a licensed Medical Director, therapists, registered nurses, direct-care staff, admissions, and case management in place before the first resident arrives. The disclosed clinical base alone is $905,000 a year: $280,000 for the Medical Director, 3 therapists at $95,000 each, and 4 registered nurses at $85,000 each.
What this hides is the risk of a weak census ramp. Staffing has to match state staffing rules, resident acuity, and medication protocols, not just an opening budget. If credential files, background checks, or coverage plans are late, admissions can slip even after the facility is ready. One gap in overnight coverage can stop safe intake, delay first revenue, and create compliance problems fast.
Hire and credential early
Build the schedule from the admission standard, not from full occupancy. Start with the roles that protect first-day care: licensed leadership, Medical Director coverage, nurses, therapists, and direct-care staff. Then verify credential files, background checks, and on-call coverage before inspection. If you wait until the inspection notice to recruit, the opening date can move.
Use a simple readiness check: who covers nights, who signs off on medications, who handles admissions, and who steps in if census runs below plan. That keeps staffing aligned to the actual ramp instead of overhiring for a full house. It also helps you open with safe admissions while preserving cash during the first months.
Confirm 24/7 coverage first.
Document licenses and background checks.
Match staff to acuity and census.
4
Referral, Payer, and Admissions Pipeline
Referral and Admissions Pipeline
A licensed center can still miss opening day if the intake side is not ready. The admissions pipeline needs active referral outreach, payer verification, and a clear authorization process before the first resident arrives, or the building opens with empty rooms and slow cash flow.
This driver covers referral sources, admission screening, denial criteria, private-pay packets, and discharge planner relationships. It depends on clinical program clarity, bed capacity, payer mix, and compliant communication rules. The launch goal is a steady ramp toward 45% Year 1 occupancy, not a facility that is open but quiet.
Build the intake desk first
Before opening, verify who can send cases and who can approve them. Outreach should be live with hospitals, therapists, psychiatrists, intervention professionals, employee assistance programs, payer contacts, and family inquiry channels, with one owner for each path. If screening rules are unclear, admissions stall and staff spend time on unqualified leads.
Set up a simple first-day workflow: referral received, eligibility checked, benefits verified, authorization tracked, private-pay packet sent, and admission decision documented. One clean lane matters. Use denial criteria early so the team can say no fast, protect compliance, and keep beds available for the right resident mix.
Assign referral owners by source.
Test verification before launch.
Document denial rules and timing.
Track every inquiry to decision.
5
Operations, Census Ramp, and Cash Runway
Operations and Cash Runway
Opening day is not a license milestone; it is a working system. The center needs the EHR live, billing workflow, medication logs, incident reporting, and live handoffs for vendors, housekeeping, food, security, maintenance, and finance reporting before the first resident arrives.
Here’s the quick math: with 17 rooms and 45% Year 1 occupancy, the average load is about 8 occupied rooms. That ramp sits under $70,500 in monthly fixed expenses, so weak census timing turns into cash strain fast. Add 6% food and beverage supplies, 3% clinical medical supplies, and 3% housekeeping and amenities, and the early months need tight control.
Test the full money flow
Before opening, run a full test from admission to billing. If a resident is admitted, charted, billed, and posted without manual fixes, the system is ready. If not, cash gets delayed and staff spend time cleaning up paperwork instead of caring for residents.
Use a simple launch pack: census dashboard, staffing schedule, cash runway, and vendor handoff log. Lock in delivery dates for food, clinical supplies, and housekeeping items, then confirm who owns each backup plan. One missed handoff can hit same-week operations, not next month.
Start by defining the program model, resident acuity, license category, and facility requirements before signing a lease This planning case uses 17 rooms, a 9 to 18+ month opening range, and 45% Year 1 occupancy Your next step is to confirm state licensing and zoning so the property, staffing, and policies fit the approval path
Plan on 9 to 18+ months before first admissions, depending on state licensing, zoning, renovations, inspections, staffing, and payer setup A 17-room center rarely opens at full census on day one This model uses 45% Year 1 occupancy, then 65% in Year 2, so runway matters during the ramp
Maybe, but it depends on your state rules, payer strategy, and program type Some launches need state licensing first, while accreditation or payer standards may come later or run in parallel The model includes a $2,500 monthly licensing and accreditation planning line, but you should verify the required sequence before committing to inspections or contracts
Licensing and facility compliance usually delay launch the most Common blockers include zoning mismatch, failed fire or occupancy inspection, incomplete clinical policies, missing credential files, and late hiring The risk is costly because the model carries $70,500 in monthly fixed expenses, including a $45,000 facility lease, before stable admissions
First revenue comes from converting qualified referrals into admitted residents with payer authorization or private-pay agreements Build referral relationships before opening with hospitals, therapists, psychiatrists, intervention professionals, and payer contacts With 17 rooms and 45% Year 1 occupancy, the practical goal is a steady census ramp, not a one-week marketing spike
About the author
Grace Hall
Startup Planning Writer
Grace Hall is a startup planning writer at Financial Models Lab, where she creates simple financial projections that help founders make business ideas easier to evaluate. She focuses on the numbers behind everyday businesses, especially for people planning to open a physical location. Grace writes about cost and income assumptions in a clear, practical way, helping readers understand what it really takes to open a business and build a realistic plan.
Choosing a selection results in a full page refresh.