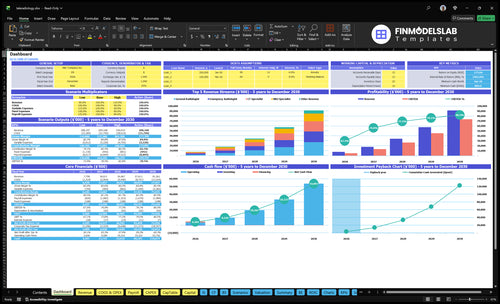
How to Start a Teleradiology Business in 3 to 9 Months
Teleradiology
You’re building a clinical service before revenue starts, so the launch plan must prove licensing, radiologist coverage, secure image flow, and client contracts before go-live This guide covers the teleradiology launch steps, startup requirements, and business checklist across a 5-year model period, with Year 1 assumptions of 13 radiologists and up to $646,500 in monthly revenue at modeled capacity Startup costs, funding, and owner compensation matter, but they support the launch plan rather than drive this page
Time to Open3-9 monthsLaunch runwayLaunch Sequence6 stagesCompliance firstKey BottleneckWorkflow gateApproval pathFirst Revenue StepSigned clientReading contract
Launch timeline
This is a short web summary; the XLSX export holds the detailed Gantt Chart.
What do you need to start a teleradiology business?
To start a Teleradiology business, you need state medical licensing, facility credentialing, radiologist privileges, malpractice coverage, HIPAA-ready systems, payer/client contracts, and a controlled pilot before reading 1 client study; this is where What Is The Main Goal Of Teleradiology's Growth Strategy? ties growth to safe capacity, not just sales. Treat this as an operating checklist, not legal advice, and confirm requirements with qualified counsel, payers, and each client facility.
Start-Up Must-Haves
Verify licensing across required US states
Complete facility credentialing before client reads
Bind malpractice insurance before operations
Confirm 24/7 coverage hours and escalation paths
Launch Order
Meet Health Insurance Portability and Accountability Act requirements
Define modality scope: X-ray, CT, MRI
Sign client, payer, and radiologist contracts
Run pilot reads before full go-live
How long does it take to launch a teleradiology service?
Teleradiology usually takes 3 to 9 months to launch, and the clock is driven by state licensing, facility credentialing, payer or client onboarding, PACS/RIS integration, reporting workflow testing, and radiologist coverage. There’s no fixed guarantee because outside approvals control part of the schedule. Start credentialing packets early, pick launch modalities first, and test DICOM image transfer before go-live.
Main timing drivers
3 to 9 months is the planning range.
State licensing can slow launch.
Credentialing and onboarding add delays.
PACS/RIS testing needs time.
How to speed it up
Send credentialing packets first.
Choose launch modalities early.
Test DICOM transfer before launch.
Put service-level terms in the first contract.
How do you get teleradiology clients?
You get teleradiology clients by selling to facilities with clear coverage gaps—imaging centers, urgent care groups, rural hospitals, outpatient clinics, and mobile imaging providers—and leading with after-hours reads, overflow reads, defined modalities, and a tight turnaround-time promise. For a quick starting point, see How Much Does It Cost To Open, Start, Launch Your Teleradiology Business?
Start with pain
Imaging centers need overflow help.
Urgent care needs fast reads.
Rural hospitals need 24/7 coverage.
Mobile imaging needs dependable handoff.
Close the first deal
Get a signed reading agreement.
Complete the credentialing packet.
Set the go-live schedule.
Test workflow, then hand off reporting.
Teleradiology Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
Confirm what must be ready before accepting studies
Launch readiness checklist
Use this go-live approval checklist to confirm the business is ready to open before launch.
1Licensing
State licensing reviewed with counselCritical
State rules vary, so counsel must clear the launch state before reads start.
Credentialing files approvedCritical
Hospitals and facilities need approved privileges before cases can route to radiologists.
Malpractice policy boundCritical
Coverage must be active before the first interpretation is delivered.
2Systems
DICOM transfer testedCritical
DICOM is the image transfer standard, and failed handoffs break turnaround time.
Viewer and archive liveCritical
Radiologists need a stable viewer and archive before remote reads start.
Reporting template validatedHigh
Consistent report fields reduce rework and support clean client delivery.
3Coverage
Year 1 roster filledCritical
The model needs 13 radiologists in Year 1 to cover forecast volume.
Specialty backup coverage signedHigh
CT, MRI, PET, and emergency backup keeps cases from stalling.
Coverage schedule publishedHigh
Clients need clear coverage windows before they send studies.
4Quality
Turnaround policy approvedHigh
Turnaround time sets client expectations and keeps urgent reads from slipping.
Critical results escalation testedCritical
Urgent findings need a live path to the ordering site.
QA review process setHigh
Quality review catches report errors before they reach clients.
5Contracts
Client contracts signedCritical
Signed contracts lock scope, rates, and service terms before go-live.
Billing workflow testedHigh
Claims or invoices need to move cleanly on day one.
Rate card approvedHigh
Prices must match the modeled treatment mix and special-case work.
6Go-live
Minimum cash fundedCritical
The model shows minimum cash of $885k, so launch needs that buffer.
Capex spend approvedHigh
Platform, hardware, security, and license buildout should be funded before launch.
Final go-live signoffCritical
Do not open until licensing, transfer, coverage, and reporting are all ready.
Want the six launch drivers that matter most?
1Licensing
License gate
No credentialing means no safe study acceptance, so approvals control the go-live date.
2Secure Stack
DICOM test
A tested DICOM transfer and access flow cuts failed handoffs and speeds pilot acceptance.
3Staffing Mix
13 radiologists
Year 1 staffing needs 13 radiologists, so capacity gaps can block promised coverage hours.
4Contract Start
1 signed deal
One signed reading contract turns interest into first revenue and locks the go-live scope.
5QA Flow
QA pass
A tested end-to-end case proves turnaround time and critical-result handling before clients trust the service.
6Runway
$646.5K/mo
Year 1 revenue is $646.5K/month, but 195% variable costs make slow onboarding a cash risk.
Regulatory and Credentialing Readiness
Credentialing Gate
No credentialing means no safe study acceptance. For teleradiology, radiologists must be licensed, credentialed, insured, and approved by the client before the first read. That includes state license coverage, malpractice coverage, facility approval, and HIPAA-aligned workflows. If any one of those is missing, go-live slips because the service cannot legally or safely start.
The real launch risk is delay, not demand. Each hospital, imaging center, or payer can add its own review queue, so the startup needs a complete packet ready before scheduling reads. One missing document can stall day-one operations, block billing, and force the team to hold cases instead of turning them around.
Front-Load Approval
Build the credentialing packet first: licenses, board status, malpractice certificate, IDs, and facility forms. Then verify which states each radiologist can read for, and match that list to the first client’s footprint. The launch signal is simple: approved readers, approved facility, and written permission to start.
Checklist before go-live:
Complete credentialing packet
Verified state license coverage
Active malpractice coverage
Facility approval on file
HIPAA workflow signed off
If approval is still pending, keep the launch date soft. A signed client without credentialing still can’t accept studies, so the business may look open on paper but stay shut in practice.
1
Secure Imaging Technology Stack
Secure Imaging Stack
This driver decides whether studies move cleanly from client intake to radiologist read and back into the chart on day one. In teleradiology, PACS (Picture Archiving and Communication System) is the core imaging storage and retrieval layer, so if DICOM image transfer, secure access, or report delivery is shaky, opening slips and first reads stall.
Readiness means a tested DICOM transfer, user access controls, reporting flow, a downtime plan, and fit with the client workflow. Weak uptime or loose data protection usually shows up as failed handoffs, delayed reports, and slower pilot acceptance.
Pre-Launch Tech Check
Before go-live, run one end-to-end case through the full stack: image intake, secure login, reading, report delivery, and archive. Verify the client can send studies into your PACS, the radiologist can open them without workarounds, and the report lands where the facility expects it. Keep ownership clear for every handoff.
Document the fallback path for downtime, access failures, and delayed reports. If the workflow needs extra steps at launch, fix them before the first pilot, because a clean first case is what gets the account to accept your service fast.
Test DICOM transfer with live files.
Confirm role-based access limits.
Check report delivery into workflow.
Write the downtime escalation path.
Match client intake and read steps.
2
Radiologist Staffing and Coverage Model
Match Coverage to Staff Mix
If the staffing plan does not cover the promised hours, modality mix, and subspecialty reads, the business cannot open cleanly on day one. The Year 1 model uses 5 general radiologists, 3 CT specialists, 2 MRI specialists, 1 PET scan specialist, and 2 emergency radiologists, so launch only works if the intake promise stays inside that coverage map.
The risk is overselling reads before backup coverage is in place. Modeled capacity ranges from 45% for PET to 65% for emergency in Year 1, which means the launch plan has to stay conservative on volume, turnaround times, and after-hours commitments. One gap in coverage can delay go-live or force service changes after contracts are signed.
Build the Coverage Matrix First
Before opening, map each client promise to a named radiologist pool, backup layer, and turnaround target. Verify the schedule by modality and hour, then test whether the team can absorb peak demand without missing reads. That means matching coverage hours, specialty coverage, and escalation rules before the first study arrives.
Use a simple launch check: hours covered, modality covered, subspecialty covered, backup covered. If any of those are short, narrow the launch scope instead of promising full-service coverage. That keeps first-day operations credible and prevents a staffing miss from becoming a patient-delay problem.
Confirm coverage by hour and modality
Assign backup radiologists in writing
Test peak-volume turnaround times
Limit launch scope to staffed reads
3
Client Acquisition and Contract Pipeline
Signed Contract Gate
Teleradiology is not launch-ready until at least one signed reading agreement locks the study types, service levels, credentialing packet, pricing, coverage hours, and go-live schedule. Until then, you have sales interest, not an open business, so first revenue stays out of reach.
The real risk is a pipeline full of hospitals, urgent care networks, outpatient clinics, imaging centers, or mobile imaging providers that want service but have not approved terms. A pilot agreement plus a tested workflow is the readiness signal; without both, opening slips because reads cannot start on day one.
Pilot Before Go-Live
Before opening, get the contract into a form that operations can run. Here’s the quick check: define the exam mix, service window, escalation rules, pricing, and who signs off on each step. If any one of those is missing, the launch plan is too loose and the first paid cases can stall.
Document study types and turnaround targets.
Confirm coverage hours and backup coverage.
Attach credentialing packet requirements.
Test the pilot workflow end to end.
Set the go-live date in writing.
One clean rule: no signed contract, no safe start. If the workflow is tested but the agreement still says “in discussion,” you can’t staff confidently, bill cleanly, or promise day-one service without risking delay and cash strain.
4
Workflow, QA, and Turnaround-Time Operations
Workflow and QA Readiness
Workflow has to cover study intake, prioritization, reporting, critical-results communication, QA review, and escalation rules before the first read. If the team cannot move a case cleanly from image receipt to report delivery, you may open on paper but not in practice, especially for 24/7 coverage and urgent findings.
The biggest launch risk is unclear ownership when a critical result needs action. If no one is assigned to call, document, and confirm receipt, the service is not ready for day one. Clients will judge the operation on whether it protects patient safety, not just whether a report was sent.
Test the Full Read Path
Before go-live, verify one complete case path: intake, priority set, read completed, critical result escalated, and report delivered. Document who owns each handoff, what triggers escalation, and how QA review is logged. That is the readiness signal, not a slide deck.
Build the launch checklist around measurable turnaround time, QA sign-off, and after-hours coverage. If the team cannot show a tested end-to-end case with clear response times and documented review, delay launch until the process works without manual rescue.
5
Financial Ramp and Cash Runway Validation
Cash Ramp Check
This launch driver decides whether the service can open and keep running before cash gets tight. The model shows $646,500 per month at stated capacity, but the disclosed variable-cost pieces add to 33%, while the driver also says variable costs total 195%. That gap has to be resolved before go-live, because pricing, staffing, and runway all depend on it.
If 195% is the real burden, monthly variable cost is about $1.26 million, which would be cash-negative before $15,700 of fixed overhead and before any CEO salary. If the line items are the full stack, variable cost is about $213,345 a month. Either way, slow onboarding and billing lag can push cash out faster than cash in.
Runway Test Plan
Before launch, lock the first-90-day assumptions in writing and test them against real client timing. Verify study volume, per-scan pricing, radiologist pay, cloud and data transfer fees, malpractice, and sales commissions. Then model how many days of lag sit between a read, an invoice, and cash collected. One clean rule: don’t open until the runway can absorb slow ramp without missing payroll or coverage.
Start with licensing, credentialing, secure systems, and one launchable client The practical sequence is compliance, PACS/RIS or viewer setup, radiologist scheduling, client contract, pilot reads, then go-live The researched model assumes 13 Year 1 radiologists and a 3 to 9 month opening range, but outside approvals can move the schedule
Plan on 3 to 9 months for a US teleradiology launch The slow parts are usually state licensing checks, facility credentialing, client onboarding, and secure image workflow integration If PACS/RIS testing or credentialing packets start late, the service can be staffed but still unable to accept studies
Not always, but clinical reads must be performed by properly licensed and credentialed radiologists Ownership, corporate practice of medicine rules, payer rules, and facility requirements vary by state and client type, so verify structure with qualified healthcare counsel Your launch plan still needs malpractice coverage, HIPAA safeguards, and a responsible clinical workflow
Credentialing and secure image transfer are the main delays A founder may line up 5 general radiologists and specialists in the model, but still miss go-live if facilities have not approved readers or the reporting workflow fails testing Start credentialing, DICOM transfer tests, access controls, and critical-results procedures early
First revenue starts with a signed reading agreement, not a website or software account Aim for one imaging center, urgent care group, rural hospital, outpatient clinic, or mobile imaging provider with defined study types, coverage hours, turnaround times, credentialing needs, and a pilot go-live date Then test reads before scaling volume
About the author
Jonathan Bell
First-Time Founder Guide Writer
Jonathan Bell is a Financial Models Lab writer focused on launch budget planning, helping aspiring small business owners estimate startup needs before opening. As a first-time founder guide writer, he explains business costs in simple language and offers simple launch planning insights that help readers compare business opportunities realistically and make grounded real-world decisions.
Choosing a selection results in a full page refresh.