Get the first patients by selling paid initial consultations with labs ordered, then launch local SEO, referral partners, and compliant outreach; for the cost side, see What Are Operating Costs For Testosterone Replacement Therapy Clinic? In Year 1, digital marketing and acquisition can run at 60% of revenue, so every lead has to move fast into a booked consult.
First patient sources
Launch local SEO in your service area
Use landing pages and call scripts
Sell evaluation, not outcome promises
Build compliant referral relationships
Track the funnel
Track lead-to-consult every week
Track consult-to-lab conversion
Track lab-to-plan conversion
Watch no-show rate by source
What are common mistakes when opening a TRT clinic?
Common mistakes when opening a Testosterone Replacement Therapy Clinic are weak protocols, missing informed consent, unclear prescribing authority, untrained intake staff, poor lab follow-up, and noncompliant marketing. If your EHR does not capture symptoms, labs, consent, treatment plan, refill timing, and follow-up, day-one operations can fail. With 1 Patient Coordinator and 1 Medical Receptionist in Year 1, missed calls and slow intake can cap revenue fast, especially with $218k in monthly fixed overhead.
Operations gaps
Write clinic protocols before launch.
Document informed consent every time.
Test EHR fields for every patient step.
Check prescribing authority in advance.
Front desk readiness
Train staff on eligibility and booking.
Use scripts for payment and privacy.
Confirm lab instructions before visits.
Test refill and follow-up workflows.
What licenses do you need to open a TRT clinic?
A Testosterone Replacement Therapy Clinic needs more than a business license: it needs the legal right to evaluate, diagnose, prescribe Schedule III testosterone, and manage follow-up care under state medical board rules. Confirm these items before modeling startup costs in What Are Operating Costs For Testosterone Replacement Therapy Clinic?, because unclear provider authority, DEA workflow, or ownership structure can block launch.
Core Licenses
State medical license for prescribers
DEA registration for controlled substances
Business registration and tax accounts
Medical director agreement, if required
Compliance Must-Haves
Check corporate practice of medicine rules
Document intake, labs, and medical necessity
Use HIPAA rules: 45 CFR Parts 160 and 164
Add CLIA coverage for in-house lab testing
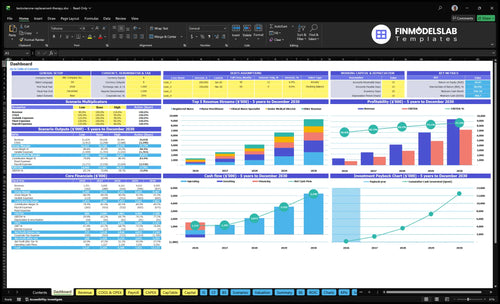
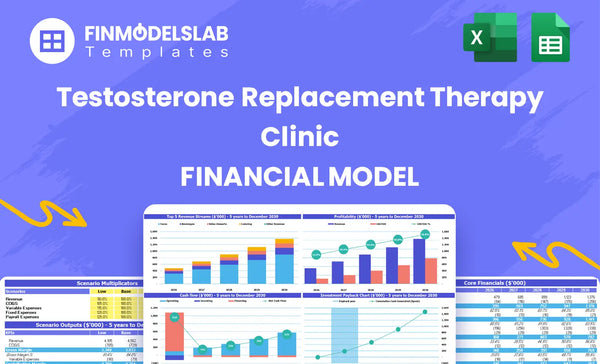
Testosterone Replacement Therapy Clinic Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
Confirm the clinic is ready before seeing patients
Launch readiness checklist
Use this go-live approval checklist before opening the testosterone replacement therapy clinic.
1Governance
Entity structure reviewedCritical
Match ownership and state medical rules before contracts, banking, and payer setup.
Medical director coverage confirmedCritical
Keep clinical oversight in place so orders, supervision, and signoff do not stall.
Provider licenses verifiedCritical
Each clinician must be licensed for the clinic's scope before any patient visit.
2Clinical
Intake and symptoms form approvedHigh
Capture low-testosterone symptoms, history, and labs the same way on every intake.
Informed consent finalizedCritical
Patients need a signed consent packet before hormone therapy starts.
Follow-up and refill rules setCritical
Define lab review, refill, and visit cadence so care stays consistent.
3Lab and meds
Lab vendor contractedCritical
Secure testing capacity before you book the first patient.
Turnaround process testedHigh
Results must return fast enough for prescribing and follow-up decisions.
Refrigeration and inventory readyHigh
Cold storage and stocked supplies prevent dose delays and waste.
4Systems
EHR templates builtHigh
Templates should cover intake, orders, notes, and lab review.
Scheduling and payments testedCritical
Patients need a clean path from booking to payment without staff workarounds.
HIPAA messaging procedures readyHigh
Protect patient data in texts, email, and portal replies from day one.
5Staffing
Year 1 care roster matchedCritical
Staff to 1 medical director, 1 NP, 1 PA, 1 CNS, and 2 RNs.
Admin coverage hiredHigh
Cover clinic admin, coordination, reception, and compliance before opening.
Training signoff completeHigh
Every role should know scripts, handoffs, escalation, and documentation rules.
6Finance
Month 2 cash floor fundedCritical
Hold the $781k minimum cash level the model shows in Month 2.
Marketing claims reviewedHigh
Ads and site copy must stay within compliant claims before spend starts.
Go-live approval signedCritical
Open only when consent, lab flow, prescribing authority, and follow-up ownership are set.
What six launch drivers decide readiness?
1Medical Compliance
DEA gate
State board review, active licenses, scope rules, and a DEA-controlled-substance workflow must be set before the clinic can legally evaluate or prescribe on day one.
2Patient Safety
10 steps
A written intake-to-follow-up workflow keeps consent, lab review, abnormal-result escalation, and refill checks clean, so first visits turn into safe treatment plans.
3Vendor Readiness
$137K
Signed lab, pharmacy, refrigeration, and inventory setup keeps consults from stalling after diagnosis, which protects the first revenue cycle.
4Facility Workflow
$21.8K/mo
Finished rooms, EHR templates, scheduling, payment, reminders, and security let staff run a full patient day without workarounds or missed charges.
5Staffing Plan
40-60%
Year 1 capacity runs about 40% to 60%, so coverage, training, and handoffs have to work before volume climbs.
6Acquisition Ramp
$1.35M
Local search, compliant ads, booking, and follow-up need to work before paid leads start, or demand will outrun the clinic's ability to schedule and close visits.
Medical Compliance And Provider Authority
Provider Authority
A TRT clinic’s launch is binary: if provider authority is not in place, the clinic cannot legally evaluate, prescribe, or manage testosterone treatment. Before opening, verify state medical board review, ownership review, active provider licenses, scope-of-practice map, and medical director coverage so day-one care is legal and not held up by a last-minute gap.
The biggest delay risk is non-physician authority tied to supervising or collaborating physician rules. If that chain is unclear, charting, prescribing, and follow-up can stall on opening week. The clean readiness signal is documented approval for prescribing workflow, telehealth rules if used, consent retention, HIPAA procedure, controlled-substance recordkeeping, and compliance training before the first patient is booked.
Pre-Open Compliance Check
Build the launch file before scheduling visits. Here’s the quick math: one missing license, permission, or workflow can stop all treatment activity, so the clinic should not rely on verbal sign-off.
Verify every active license.
Map who can prescribe.
Lock consent and HIPAA forms.
Set DEA-controlled-substance workflow.
Train staff on charting rules.
Also test role permissions in the EHR, confirm medical director coverage, and document how records are stored and retained. If telehealth is part of the model, check state telehealth rules first; otherwise, day-one operations can open with a legal gap and messy charts.
1
Clinical Protocol And Patient Safety Workflow
Clinical Workflow Readiness
For a testosterone replacement therapy clinic, this driver decides whether day one feels controlled or chaotic. The clinic needs a written workflow for intake, symptoms review, medical history, lab ordering, diagnosis support, informed consent, treatment planning, monitoring, refill review, and follow-up. If that chain is missing, visits may still happen, but charting gets messy fast and follow-up breaks down.
The launch risk is not just speed; it is safe consistency. Readiness depends on provider sign-off, lab partner setup, pharmacy process, and staff training. The early warning sign is simple: every patient task must route cleanly in the EHR, or the clinic can end up with revenue but no reliable follow-up. That is how 40% to 60% Year 1 capacity growth by role gets stuck.
Lock the Patient Flow Before Opening
Build the workflow around the exact handoffs staff will use on the first patient. Write the steps, assign owners, and test the path from inquiry to follow-up so no one is guessing in real time. Keep the process operational, not theoretical: who enters the intake, who reviews labs, who flags abnormal results, and who closes the loop on missed visits.
Here’s the quick checklist: EHR templates, consent forms, lab review routing, abnormal-result escalation, patient education scripts, and a missed-follow-up process. If any one of those is weak, chart gaps grow, visits take longer, and the team spends opening week fixing errors instead of serving patients.
Map each step to one owner.
Test lab-to-chart routing before launch.
Write the missed-follow-up process.
Train staff on consent and escalation.
Verify pharmacy handoff timing.
2
Lab, Pharmacy, And Supply Vendor Readiness
Lab, pharmacy, and supply readiness
Without a signed lab workflow and pharmacy handoff, a consult stays a consult. The clinic needs specimen collection, turnaround targets, result delivery into the EHR, and a clear refill path before day one, or patients wait and conversion stalls. No lab, no plan, no fill.
Plan cash for $85k in diagnostic lab equipment in Month 1 to Month 3, $12k for refrigeration in Month 1, and $40k in initial inventory in Month 5 to Month 6. Year 1 direct costs assume 65% lab fees and 55% for medical supplies and hormones, so delayed onboarding or weak vendor terms will hit early margin fast.
Lock the vendor flow before launch
Get the lab partner, pharmacy, and storage controls confirmed in writing before you open. Verify who orders tests, who receives results, who updates the chart, and who triggers the fill. Build the sequence around real lead times, not hope. If any step is unclear, first-day revenue slows because treatment plans can’t move forward.
Sign lab workflow and turnaround times.
Test EHR result routing.
Document refrigeration and security.
Set inventory controls and refill steps.
Also, assign one owner for lab follow-up and one for pharmacy issues. If results, fills, or supplies slip even by a few days, consult-to-plan conversion drops and staff spend time chasing missing items instead of seeing patients.
3
Facility, EHR, And Operating Workflow
Facility, EHR, and workflow readiness
Opening risk here is simple: staff must run a full patient day without workarounds. The clinic needs exam rooms, private intake space, EHR templates, HIPAA forms, scheduling, lab ordering, payment capture, reminders, and follow-up queues before first patients arrive. With $270k of buildout, furnishings, hardware, waiting area, and security work spread across Months 1-6, any delay pushes launch back while rent and IT burn keep running.
The fixed base is not light: $12k rent plus $25k EHR and IT infrastructure each month. Here’s the quick math: broken workflows do not just slow visits; they create missed charges, rework, and front-desk bottlenecks. The launch signal is clean if a new patient can check in, complete intake, get ordered labs, pay, and leave with follow-up already queued.
Build the day-one flow before the decor
Sequence the setup around patient flow, not furniture. Verify room count, network, devices, form templates, and payment steps in the exact order staff will use them. Test one full visit from booking to follow-up, and fix any handoff that requires a manual note, separate spreadsheet, or second login.
Lock EHR templates before go-live.
Test reminders and follow-up queues.
Confirm HIPAA forms and payment capture.
If the clinic opens with elegant rooms but weak routing, first-day care gets clumsy fast. That usually shows up as slower check-ins, chart gaps, missed lab orders, and charges that never get posted. The safer path is to train staff on the same workflow they will use on day one, then run a full mock day.
4
Staffing Plan And Training
Staffing Coverage And Training
This clinic can’t open cleanly without provider schedule coverage and clear handoffs. Year 1 staffing assumes 1 Senior Medical Director, 1 Nurse Practitioner, 1 Physician Assistant, 1 Clinical Nurse Specialist, and 2 Registered Nurses, so the real launch risk is not headcount alone, it’s whether intake, labs, payments, and follow-up are owned every day.
On the operating side, the clinic needs 1 Clinic Administrator at $85k, 1 Patient Coordinator at $55k, 1 Medical Receptionist at $42k, and a Compliance Officer at $95k annual salary basis. The bottleneck is simple: missed calls, slow lab routing, or no one owning follow-up can cut booked consults and create safety gaps before the first month is stable.
Pre-Open Coverage Checks
Before opening, verify the daily workflow in order: intake, symptom review, lab coordination, payment collection, patient communication, and follow-up. Here’s the quick test: if one person is out, does the clinic still have a named backup for each step? If not, day-one capacity is fragile and the schedule will slip.
Train staff on scripts, escalation rules, and who closes each task in the system. The Billing Specialist starts in Month 13, so early revenue depends on clean front-end work now. Test missed-call recovery, lab result routing, and follow-up ownership before launch; those are the first places where cash and patient trust leak.
Assign one owner per step.
Test backup coverage before opening.
Drill lab and follow-up routing.
Check payment flow on day one.
5
Patient Acquisition And Revenue Ramp
Patient Acquisition Ramp
Opening on time depends on turning inquiries into paid initial consultations and lab orders on day one. The launch is ready only when local search, compliant ad copy, landing pages, booking, call scripts, referral outreach, lead tracking, consultation payment, and follow-up all work together.
The model ties 60% of Year 1 revenue to digital marketing, with revenue assumptions of $1351M in Year 1, $2600M in Year 2, and $4161M in Year 3. Year 1 treatment price assumptions run from $150 to $450, so weak lead handling can slow cash flow fast.
Pre-Launch Conversion Checks
Test the full path before opening: search click, call, booking, payment, and follow-up. If ads generate leads before staff can answer, qualify, and schedule them, you burn spend and miss early revenue. That’s the core bottleneck.
Verify local search profiles first.
Approve compliant ad copy only.
Test booking and payment flow.
Train call scripts before launch.
Assign follow-up within 24 hours.
What this estimate hides is simple: a TRT clinic does not ramp on traffic alone. It ramps when the first consults are answered, paid, and routed into labs without gaps. If follow-up is slow, the first revenue cycle gets messy fast.
6
Testosterone Replacement Therapy Clinic Business Plan
Start with compliance, not marketing Confirm state medical rules, provider authority, DEA-controlled-substance workflow, consent forms, lab process, pharmacy workflow, and HIPAA procedures before booking patients The researched launch path assumes 3 to 6 months, Year 1 clinical coverage across 6 providers, and a financial model check showing $781k minimum cash in Month 2
A coordinated TRT clinic launch usually takes 90 to 180 days Buildout in the model runs from Month 1 to Month 6, while lab equipment starts in Month 1 to Month 3 and initial inventory lands in Month 5 to Month 6 Provider credentialing, EHR setup, lab agreements, and pharmacy workflow decide whether that timeline holds
No, not always, but the workflow must match your payment model The researched model starts with direct payment assumptions, including 25% credit card processing and no Billing Specialist until Month 13 If you add insurance billing earlier, you need eligibility checks, coding controls, claim follow-up, and a longer cash-collection process before opening
The big delays are provider licensing, DEA-controlled-substance workflow, lab agreements, pharmacy setup, EHR templates, and clinic buildout The model also carries $218k in monthly fixed overhead from Month 1, so delays burn cash before revenue starts If consent forms, lab routing, or follow-up ownership are unclear, the clinic is not ready
The first revenue step is a paid initial consultation with labs ordered That requires a compliant landing page, trained intake staff, scheduling, payment collection, provider availability, lab workflow, and follow-up The researched model reaches Month 1 breakeven under its assumptions, but that only works if leads move cleanly from inquiry to consult to labs
About the author
Ava Mitchell
Business Plan Writer
Ava Mitchell is a business plan writer at Financial Models Lab who helps early-stage founders choose realistic business ideas with founder-friendly numbers. She explains startup planning in plain English, with a focus on operating expense planning and on breaking down revenue, expenses, and profit so founders can make practical real-world decisions.
Choosing a selection results in a full page refresh.