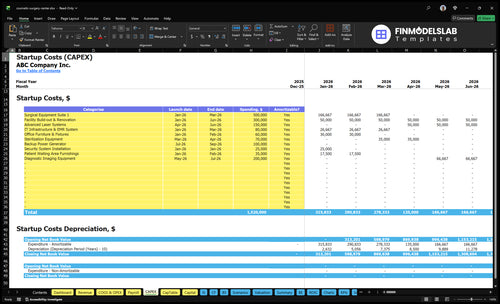
Cosmetic Surgery Center Startup Costs With $92K Opening-Month Overhead
This cosmetic surgery center startup budget covers facility CAPEX, pre-opening expenses, opening-month overhead, and working capital for the early ramp-up period The provided model shows $92,250 in monthly fixed overhead before variable procedure costs, based on $56,000 in fixed facility and insurance costs plus $36,250 in administrative payroll It excludes real estate purchase, surgeon acquisition, financing fees, owner distributions, and post-opening expansion
Estimate Startup Costs with Calculator
Startup CAPEX Calculator
Estimates capitalized startup assets only for a cosmetic surgery center: build-out, equipment, furniture, IT, and contingency.
!
Excludes runway and operating costs This calculator covers capitalized startup assets only. It excludes working capital, payroll runway, deposits, inventory, debt service, owner compensation, marketing after launch, and monthly fixed overhead. Depreciable assets are the build-out, equipment, furniture, and IT items; runway funding still needs a separate source.
Calculate Fuding Needs
Startup cost summary
This table summarizes the main startup assets and the excluded working capital reserve for a cosmetic surgery center.
Highlighted CAPEX$1,100,000Base planning example
Excluded cash needs$493,000Outside CAPEX total
Funding need$1,593,000CAPEX + excluded cash needs
Cost Category
Base Estimate
Main Cost Driver
CAPEX Calculator
Surgical Equipment Suite
$500,000
Operating-room equipment and surgical setup
Yes
Facility Build-out & Renovation
$300,000
Leasehold improvements and procedure-room build-out
Lean, base, and full launch change startup cost fast because room count, equipment depth, and staffing drive the build. The base case matches the Year 1 model; full launch adds more capacity for later growth.
Lean, base, and full launch cost comparison
Scenario
Lean LaunchLower CAPEX
Base LaunchBalanced launch
Full LaunchExpansion-ready
Launch model
An office-based surgical setup with fewer rooms, limited equipment depth, and tighter working capital.
This matches the Year 1 model with 2 surgeons, 1 anesthesiologist, 3 nurses, 1 injectables specialist, and 1 laser technician.
A multi-room surgical facility built for higher staffing depth and growth toward Year 5 provider counts.
Typical setup
Keeps the core surgical flow but trims nonessential rooms and support layers.
It uses the model's $92,250 monthly fixed overhead and $3.924 million modeled Year 1 revenue.
It is designed to scale toward 6 surgeons, 3 anesthesiologists, 7 nurses, 4 injectables specialists, and 3 laser technicians.
Cost drivers
Fewer rooms
smaller team
limited equipment
tighter working capital
Surgical equipment
facility build-out
staffing
malpractice insurance
patient acquisition
Multi-room build-out
deeper staffing
more equipment
backup power
imaging systems
Planning rangeCAPEX only
$900,000 - $1,200,000Lower CAPEX
$1,400,000 - $1,700,000Balanced launch
$1,800,000 - $2,500,000Expansion-ready
Best fit
Best for founders testing demand with a smaller opening footprint.
Best for operators who want the model's planned setup without a heavier build.
Best for teams opening at fuller capacity and planning for faster scale.
!
Planning note: These scenario ranges are researched planning assumptions from the model, not exact vendor quotes or fixed bids.
What are the biggest cosmetic surgery center cost drivers?
The biggest cost drivers for a Cosmetic Surgery Center are the accredited operating room buildout, anesthesia and recovery capacity, and the procedure mix you choose. A Year 1 plan with 2 surgeons, 1 anesthesiologist, 3 nurses, 1 injectables specialist, and 1 laser technician gets expensive fast if it leans surgical, since higher surgical mix raises buildout, equipment, supplies, insurance, and working capital.
Facility cost drivers
Accredited OR scope drives buildout cost
Recovery bays add space and staffing
Sterilization space raises square footage needs
HVAC, plumbing, electrical, medical gas matter
Volume and staffing drivers
Capacity runs 60% for surgeons and anesthesia
Injectables and laser run at 75%
Pricing spans $500 laser to $15,000 surgery
Premium tech and surgeon ownership shape cash need
What hidden costs of opening a cosmetic surgery center get missed?
If you’re opening a Cosmetic Surgery Center, the hidden costs are the cash items outside CAPEX—see How Much Does The Owner Of A Cosmetic Surgery Center Typically Make?—and they can hit before the first procedure is booked. Think accreditation prep, legal formation, healthcare compliance counsel, surgeon and medical director agreements, credentialing, recruiting, training, deposits, and launch spend. The big recurring anchors alone can include $15,000 for malpractice, $1,000 for general liability, $3,000 for professional fees, and $2,000 for admin software and EMR, plus 7% of Year 1 revenue for marketing, or about $274,680.
Pre-open setup
Accreditation prep and legal formation
Compliance counsel and contract drafting
Credentialing, recruiting, and staff training
Malpractice and workers’ comp setup
Launch cash needs
Initial implants, pharmaceuticals, dressings
Injectables, photography, and website
Launch marketing and payment systems
Cash cushion for the revenue ramp
How much capital do you need to start a cosmetic surgery center?
For a Cosmetic Surgery Center, don’t fund only buildout and equipment: your raise should cover CAPEX, pre-opening spend, and operating runway. Based on the model, first-year operating need before CAPEX and pre-opening costs is $1.813 million: $1.107 million fixed overhead plus $706,320 variable costs; see What Is The Current Growth Trajectory For The Cosmetic Surgery Center? for the growth context.
Core Funding Math
Monthly fixed overhead: $92,250
Annual fixed overhead: $1.107 million
Modeled Year 1 revenue: $3.924 million
Variable costs: 18%, or $706,320
Runway Risk
Facility and insurance: $56,000/month
Admin payroll: $36,250/month
Supplies and implants: 6% of revenue
Cover volume below 60%–75% capacity
Key Takeaways
Buildout is usually the biggest startup cash need.
Equipment should match Year 1 procedure volume.
Licensing and insurance can delay opening and raise cash needs.
Pre-opening payroll needs funding before first patient revenue.
Cosmetic Surgery Center Core Five Startup Costs
Surgical Facility Buildout Startup Expense
Buildout Scope
Surgical facility buildout is usually the biggest location expense because it has to cover procedure rooms, operating rooms, recovery, sterilization, HVAC, plumbing, electrical, medical gas, patient flow, reception, staff space, storage, accessibility, and life-safety. Size the layout for Year 1: 2 surgeons, 1 anesthesiologist, 3 nurses, 1 injectables specialist, and 1 laser technician.
What To Estimate
Here’s the quick math: estimate by room count, contractor quotes, and the condition of the leasehold, plus state rules and accreditation needs. A shell suite, a prior medical office, and a near-ready surgical space price very differently. Avoid a universal per-square-foot guess; the same center may need more rooms or future expansion if it is built for Year 5 growth to 23 clinicians.
How To Control Spend
Keep the first phase tight: build only the rooms needed for the opening schedule, then reserve space for later buildout. The main mistake is overbuilding a premium suite before volume proves it. One clean rule: design for flow first, looks second. Good savings come from phased construction, not from cutting HVAC, plumbing, electrical, medical gas, or life-safety work.
Growth Trigger
If the center is meant to scale by Year 5, plan now for more procedure rooms or an easier future expansion path, because the clinical team rises to 6 surgeons, 3 anesthesiologists, 7 nurses, 4 injectables specialists, and 3 laser technicians. Room count should follow that staffing plan, or you’ll bottleneck patient flow long before demand runs out.
Licensing, Accreditation, Insurance, And Professional Setup Startup Expense
Licensing Setup
Plan this as a cash-and-timing item, not just paperwork. State licensing, accreditation readiness, policies, legal formation, compliance counsel, medical director or surgeon agreements, and credentialing can all hit before revenue starts. The model anchors are $15,000 a month for malpractice, $1,000 for general liability, and $3,000 for legal and accounting, before workers’ compensation deposits.
What Drives Cost
Use quotes and required months of coverage to build the estimate. State rules, the anesthesia model, ownership structure, and facility type can change both the approval path and the cash needed upfront. The core math is simple: required filings plus pre-opening insurance plus professional fees. One setup can be light; another can lock up a lot of cash.
Check state filing steps first.
Price insurance by month.
Confirm credentialing lead times.
Control The Spend
Start with the exact service mix and ownership model, then buy only the compliance work you need now. Ask for fixed-fee legal and accounting quotes, and separate one-time setup work from ongoing monthly coverage. Don’t overbuild policies or agreements before the facility type and anesthesia model are locked, because that can push cash out with no revenue benefit.
Get fixed-fee quotes.
Separate one-time vs monthly costs.
Delay nonessential extras.
Before Revenue Starts
What this cost hides is timing risk. If licensing, accreditation, or credentialing takes longer than planned, you keep paying $19,000 a month in anchored legal and insurance costs before the first procedure. The cash need rises fast when the facility needs more state review, more agreements, or a stricter anesthesia setup.
Initial Supplies, Technology, And Launch Marketing Startup Expense
Launch Stock
At $3.924 million Year 1 revenue, launch stock is not monthly replenishment. Use 6% for medical supplies and implants, 2% for pharmaceuticals, 7% for marketing and patient acquisition, and 3% for external anesthesia and lab fees; that is about $706,320 total.
Tech Stack
Initial tech should cover the electronic medical record, practice management, payments, website, photography, and customer relationship management. Price it from setup quotes and months of coverage, then add surgical disposables, dressings, injectables, and skincare only for the first cases you plan to book.
Market Push
Opening marketing should fund patient acquisition before the schedule fills. Tie spend to booked consults, not vanity clicks, and match inventory depth to the procedure mix, since a surgery-heavy launch needs more disposables and implants than an injectables-heavy one. One clean rule: stock to booked cases, not to wishful demand.
Cash Plan
The cash risk is timing. Buy launch supplies once, then keep a separate reorder budget for month-to-month use; otherwise, the opening budget gets blurred and true startup need is understated. If the mix shifts toward implants or higher-volume injectables, the initial buy grows fast, so track each category line by line.
Surgical And Medical Equipment Startup Expense
Core launch kit
Your launch set should cover OR tables, surgical lights, monitors, anesthesia equipment, electrosurgical units, sterilizers, recovery beds, emergency equipment, procedure carts, photography setup, injectable storage, and procedure-specific devices. In Year 1, that stack needs to support $15,000 surgical cases, $3,000 anesthesiology, $1,200 nursing-supported procedures, $800 injectables, and $500 laser treatments.
Price the room
Estimate cost by unit count × vendor quote, then add install, training, and service terms. Separate must-have launch gear from optional premium devices so the budget reflects actual use, not wishful planning. Here’s the quick math: a room only needs devices that match its first-year procedure mix, not a full menu on day one.
Quote each critical item
Track install and service
Match units to rooms
Buy in stages
Premium devices belong in a later purchase plan unless volume clearly supports them. A laser or specialty device can look nice in an empty room, but if it only serves low-volume $500 treatments, it can tie up cash fast. Start with shared equipment first, then add procedure-specific gear when scheduled cases prove the return.
Delay low-use devices
Reuse shared systems
Expand after case volume
Match mix to gear
Procedure mix should drive equipment depth. Higher-priced surgical cases at $15,000 justify a deeper core setup than injectables at $800 or laser work at $500. What this estimate hides: service contracts, calibration, and replacement parts can quietly lift cash needs, so keep a spare list and buy only what your first-year schedule can absorb.
Staffing Readiness And Pre-Opening Payroll Startup Expense
Launch Payroll
Before the first case, this cost covers surgeon support, anesthesia coverage, registered nurses, surgical techs, front desk, patient coordinators, billing, recruiting, onboarding, credentialing, training, and launch scheduling. The model’s Year 1 administrative payroll is $435,000, or $36,250/month, and it should be tracked separately from post-opening payroll and working capital.
Core Team
Use the staffing anchor to price the launch team: 2 surgeons, 1 anesthesiologist, 3 nurses, 1 injectables specialist, and 1 laser technician. For admin support, the model lists a $150,000 center director, $60,000 patient coordinator, 2 medical assistants at $45,000 each, a $80,000 marketing manager, a $55,000 billing specialist, and a $40,000 receptionist.
Cash Control
Keep pre-opening payroll lean by phasing hires to the opening schedule, not the wish list. The biggest mistake is paying full staff before credentialing, training, and patient bookings are ready. One clean rule: hire for the first launch tasks first, then add roles as volume proves out.
Hire in booking order.
Finish credentialing before opening.
Delay noncritical admin roles.
Budget Split
Pre-opening payroll is a setup cost, not day-one operating payroll. Keep it separate from post-opening working capital so you can see how much cash is needed just to get the center staffed, trained, and ready. If hires happen too early, cash burns before revenue starts; if they happen too late, the opening slips.