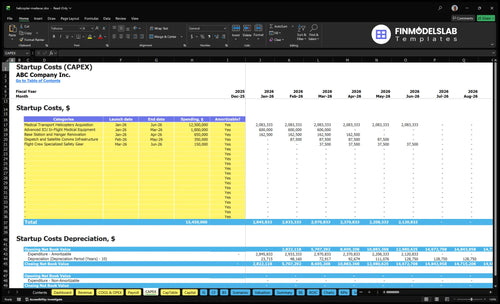
Helicopter Medevac Startup Costs: $1545M CAPEX Plan
It takes a large, staged funding plan to start a helicopter medevac service because the aircraft, clinical fit-out, insurance, staffing, and certification work all hit before collections are steady In this researched startup cost estimate, planned CAPEX totals $1545M, led by $125M for medical transport helicopter acquisition and $18M for advanced ICU in-flight medical equipment The first operating year assumes 400 emergency transports, 250 inter-facility transfers, and 10 industrial standby retainers, producing $157M in revenue The model’s lowest cash point is -$11425M in Month 6, so the real funding need must include working capital, not just equipment
Estimate Startup Costs with Calculator
Startup CAPEX Calculator
Estimates capitalized startup assets only for a helicopter medical evacuation service, including launch-month build items and Month 6 readiness spend.
!
CAPEX only This calculator covers capitalized startup assets only. It excludes payroll runway, working capital, debt service, reimbursement lag, maintenance reserves, inventory, deposits, and other operating expenses.
Helicopter Medical Evacuation Service Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
How much money do you need to start a helicopter medevac service?
Plan on funding more than equipment: the Helicopter Medical Evacuation Service model needs $15.45M in planned CAPEX plus pre-opening costs and working capital to cover a Month 6 cash low of -$11.425M; see What Are Operating Costs For Helicopter Medical Evacuation Service? for the operating cost stack. Here’s the quick math for Year 1 revenue: 400 emergency transports × $25k = $10M, 250 transfers × $18k = $4.5M, and 10 standby retainers × $120k = $1.2M, or $15.7M total.
Startup funding
Planned CAPEX: $15.45M
Month 6 cash low: -$11.425M
Separate equipment from total funding
Figures are assumptions, not quotes
Major cost drivers
Insurance: $55k/month
Hangar/base lease: $185k/month
Dispatch systems: $65k/month
Year 1 payroll: about $2.127M
What hidden costs come with starting a helicopter medevac service?
The hidden costs in a Helicopter Medical Evacuation Service start before the first flight: FAA Part 135 timing, state EMS licensing, clinical protocols, pilot and clinical payroll, and insurance deposits tied to about $55k in monthly cost. Working capital is the bigger trap, with billing setup at 35% of Year 1 revenue, medical consumables and pharmaceuticals at 25%, and aviation fuel and oil at 65%. For launch steps, see How Do I Launch A Helicopter Medical Evacuation Service?; the model also shows minimum cash of -$11425M in Month 6 despite Month 1 breakeven.
Pre-open cash
FAA Part 135 timing can delay launch.
State EMS licensing and protocols cost upfront.
Pay pilot and clinical payroll before revenue.
Insurance deposits tie to about $55k monthly cost.
Run-rate cash
Hold maintenance reserves above the 70% model.
Build dispatch, satellite tracking, and hospital coordination.
Billing setup takes 35% of Year 1 revenue.
Consumables and pharmaceuticals can take 25%, fuel and oil 65%, and payer lag worsens cash.
Should you buy or lease a medical helicopter?
Don’t pick buy or lease on cash alone. For a Helicopter Medical Evacuation Service, the real choice is whether ownership, leasing, or outsourced aircraft partnerships best fit your $125M helicopter plan across Month 1 to Month 6, because lease deposits cut upfront cash but do not remove maintenance, hull insurance, training, conformity, or downtime risk.
Buy only if the math fits
Used vs new changes cost and readiness.
EMS completion and avionics add spend.
Utilization target must cover fixed cost.
One aircraft may miss coverage promises.
Lease or partner when risk is high
Lease deposits do not erase aircraft economics.
Lender covenants can limit flexibility.
Service area range shapes the right setup.
Geography, payer mix, and hospital networks differ.
Calculate Fuding Needs
Startup cost summary
This table summarizes startup CAPEX and excluded launch cash for a helicopter medical evacuation service.
Month 6 cash trough from launch timing, staffing, insurance, and overhead
No
Helicopter Medical Evacuation Service Core Five Startup Costs
Aircraft Acquisition and EMS Configuration Startup Expense
Fleet CAPEX
Aircraft and EMS fit-out is the biggest launch check. The model carries $125M for medical transport helicopters from Month 1 to Month 6, covering purchase or lease deposits, used vs. new aircraft, interior completion, stretcher systems, oxygen, avionics, satellite comms, night gear, conformity work, and lender or lessor rules. This is CAPEX-heavy.
Cost build
Build this from aircraft count × unit price or deposit, plus completion quotes and conformity work. New aircraft cost more up front; used aircraft may cut cash but still need EMS conversion and approval work. To size it, define service radius, 24/7 coverage, backup aircraft, and downtime coverage before you lock the fleet plan.
Count aircraft by base and backup need
Separate deposit, completion, and approvals
Ask for lender and lessor terms
Cash control
Leasing can shift cash timing, but it does not remove aircraft economics, hull insurance, downtime exposure, or maintenance reserve needs. The cleanest control is to match fleet size to call volume and service area, then set reserves for scheduled maintenance and backup coverage. Under-sizing the fleet saves cash now and can hurt response reliability later.
Use leases for timing, not cheaper ownership
Budget downtime and reserve costs
Plan a backup aircraft
Sizing checks
Before you finalize the budget, pin down how many aircraft you need, the service radius, whether coverage is 24/7, and if one backup aircraft is required. Those four answers change the CAPEX line fast, because they drive purchase timing, conversion scope, and the amount of spare capacity you must hold.
Medical Equipment and Clinical Readiness Startup Expense
ICU Loadout
$18M covers the advanced in-flight ICU setup across Month 1 to Month 3: stretcher loading systems, monitors, defibrillators, ventilators, infusion pumps, oxygen, suction, trauma supplies, medications, infection-control supplies, and clinical checklists. Treat durable gear as CAPEX and split it from consumables so you can track what lasts versus what gets used on every flight.
Cost Build
Build this line with two inputs: durable equipment CAPEX and initial consumables. Durable items are the fixed launch spend; consumables and pharmaceuticals sit in COGS, or direct supply cost. The model uses 25% of Year 1 revenue for consumables and drugs, then 20% from Year 3 onward. One clean rule: buy the plane kit once, restock the patient kit every month.
Quote each device by unit count.
Separate one-time from used-up items.
Model by month, not just year.
Restock Plan
To keep quality tight without wasting cash, set a monthly restock budget at 25% of Year 1 revenue ÷ 12. Then reset the run rate to 20% of Year 3 revenue ÷ 12 once volume and buying power improve. Don’t mix spare durable gear into supply spend, or you’ll overstate burn and hide real flight-by-flight usage.
Stock for flight volume, not hope.
Track expiry dates on meds.
Reorder before critical stock-outs.
Launch Readiness
Keep the startup budget clean by tagging each item as CAPEX, initial stock, or monthly restock. That split shows how much cash is locked into durable gear versus what turns over with each mission, and it keeps the month-to-month supply burn visible before service ramps.
Regulatory Certification and Professional Setup Startup Expense
Cert Stack
This bucket covers FAA Part 135, state EMS air ambulance licensing, operations manuals, safety management systems, medical director oversight, legal support, compliance consultants, insurance documents, and accreditation planning. It is a cash cost and a timing risk. If approval slips, pre-revenue payroll and insurance keep burning while major CAPEX still runs through Month 6.
Cost Inputs
Estimate this from quote-backed work: FAA operating authority, manual drafting, SMS setup, state filings, medical oversight, and accreditation prep. Add the months of consultant time plus the payroll and insurance burn before launch. The key question is not just price; it is how many weeks of delay you can absorb before cash tightens further.
Quote each compliance workstream
Track approval months
Add pre-launch burn
Trim Burn
Start manuals and SMS work before aircraft delivery, and run federal and state steps in parallel. Keep one owner on compliance so you do not pay twice for edits. The mistake to avoid is locking in payroll and insurance before the launch date is firm.
Parallelize filings early
Use one document owner
Avoid duplicate reviews
Delay Risk
Certification is not just a fee; it decides when you can bill. If approval slips, you still carry pre-revenue payroll and insurance, so the cash gap widens fast. With major CAPEX running through Month 6 and minimum cash at -$11425M, even a short delay can force more bridge capital.
Base Infrastructure, Communications, and Dispatch Startup Expense
Base Build
Base infrastructure is the launch point for safe, 24/7 service. Budget $650k from Month 1 to Month 4 for station and hangar renovation, plus $350k from Month 2 to Month 5 for dispatch and satellite communications. That covers helipad access, crew quarters, maintenance space, weather tools, radios, tracking, and hospital coordination.
What To Budget
Estimate this with line items, quotes, and timing. Use leasehold work, helipad access, fuel arrangements, crew quarters, maintenance space, weather tools, dispatch software, radios, satellite tracking, and hospital systems. The upfront budget is $1.0M total across both workstreams, spread over Month 1 to Month 5.
Keep It Lean
Phase noncritical upgrades and buy only what launch needs. The trap is ignoring recurring burn: $185k monthly hangar and base lease, $65k monthly communications and dispatch, and $42k for utilities and security. Keep the site sized to service coverage, not excess square footage.
Monthly Burn
This line item ties directly to uptime. If the base cannot support helipad access, fuel, crew space, and dispatch coverage at once, response times slip. The recurring fixed load is $292k per month, so the buildout should match aircraft schedule and hospital call flow, not a bigger footprint than demand needs.
Insurance, Staffing Readiness, and Training Startup Expense
Insurance Burn
$55k per month for aviation and liability insurance is about $660k a year before payroll, training, or gear. For a helicopter EMS launch, this is a fixed cost, so it starts before revenue and keeps burning until aircraft and crew are active. Count 12 months of coverage in the opening budget.
Year 1 Crew
Year 1 staffing totals $2.127M in annual payroll before taxes and benefits: chief pilot $185k, 4 flight nurses at $115k each, 4 flight paramedics at $98k each, 4 line pilots at $145k each, 2 maintenance technicians at $105k each, and 4 dispatchers at $75k each. That is about $177.3k per month.
Use headcount times salary.
Exclude taxes and benefits.
Budget by month, not year.
Training Cash
This bucket also covers recruitment, recurrent training, medical protocols, and $150k of safety gear CAPEX. Separate durable gear from consumables, because launch payroll and training cash sit in working capital until reimbursements arrive. The practical check is whether you can fund at least one full crew cycle before first collections.
Keep gear and payroll separate.
Plan for reimbursement lag.
Track pre-opening cash closely.
Timing Risk
Classify this cost as pre-opening or working-capital-heavy unless you capitalize part of it. The risk is timing: insurance, hiring, and recurrent training start before patient revenue, so any delay widens the cash gap. If you move one month later, add another month of $55k insurance plus roughly $177k payroll.
Compare 3 Startup Cost Scenarios
Scenario table
Air ambulance costs swing hard with aircraft strategy, crew depth, and insurance. Lean keeps cash lighter with one aircraft or a partner; full adds 24/7 coverage, backup capacity, and heavier staffing.
Lean, base, and full launch paths for air ambulance setup and funding.
Scenario
Lean LaunchCash light
Base LaunchBalanced control
Full LaunchCoverage depth
Launch model
Runs a single-aircraft or partner-backed setup to test limited coverage with lower upfront aircraft cash.
Uses the source model: $15.45M CAPEX, $15.7M Year 1 revenue, and minimum cash of -$11.425M in Month 6.
Builds a multi-aircraft, 24/7 coverage model with backup capacity and more on-call crews.
Typical setup
Uses fewer crews, lighter hangar needs, and more outsourced lift support.
Includes helicopter acquisition, ICU gear, hangar work, dispatch systems, and a full clinical crew.
Adds more pilots, nurses, paramedics, mechanics, hangar space, and insurance to keep response times open.
Cost drivers
Aircraft access
certification timeline
insurance
smaller crew
partner dependency
Helicopter acquisition
ICU equipment
insurance
clinical staffing
hangar and dispatch
Extra aircraft
higher insurance
larger crew
hangar space
certification timeline
Planning rangeCAPEX only
Under $15.45MLow cash
$15.45M planned CAPEXBalanced control
Above $15.45MCoverage depth
Best fit
Best for founders testing one route, one region, or a partner-led launch with tight cash.
Best for operators using the source model to balance control, coverage, and funding needs.
Best for dense markets, hospital networks, and contracts that need constant coverage.
!
Planning note: Scenario ranges are researched planning assumptions, not exact quotes or bids.
Helicopter Medical Evacuation Service Business Plan
The researched model shows $1545M in planned CAPEX The largest line is $125M for medical transport helicopter acquisition, followed by $18M for advanced ICU in-flight medical equipment Base renovation adds $650k, dispatch and satellite communications add $350k, and flight crew specialized safety gear adds $150k
The model shows payback in 25 months, with breakeven in Month 1 That does not mean cash risk is gone The lowest cash point is -$11425M in Month 6 because aircraft, medical equipment, base work, staffing, and insurance need cash before collections fully mature
Yes, a US helicopter medevac operator generally needs Federal Aviation Administration operating authority, commonly tied to Part 135 commercial air carrier rules, plus state EMS licensing Budget for manuals, safety systems, legal support, medical director oversight, and compliance work Certification timing matters because delays extend payroll, insurance, and lease burn
The best strategy depends on coverage needs, control, and cash Buying gives more control but the model carries $125M of aircraft acquisition CAPEX Leasing can reduce upfront cash but adds deposits, lease obligations, maintenance rules, and insurance requirements Partnering can help test demand but may limit response control
The first-year staffing plan includes 1 chief pilot, 4 flight nurses, 4 flight paramedics, 4 line pilots, 2 maintenance technicians, and 4 dispatchers Base salaries total about $2127M annually before payroll taxes and benefits Staffing depth must match coverage hours, rest rules, clinical protocols, and aircraft availability
About the author
Martin Fletcher
Founder Support Writer
Martin Fletcher is a founder support writer at Financial Models Lab, focused on practical profit planning for founders writing a business plan. He helps small business owners understand how profit works, with clear guidance on startup cost estimates and the numbers to check before money is invested. His writing keeps the focus on useful figures and realistic expectations.
Choosing a selection results in a full page refresh.