Home Infusion Therapy Startup Costs: $905K Opening Cash Plan
Key Takeaways
Licensing delays can pressure payroll and receivables fast.
Reusable equipment costs differ from consumable supplies.
Hardware is upfront; software and claims fees recur.
Hiring should follow referral growth, not run ahead.
Estimate Startup Costs with Calculator
Startup CAPEX Calculator
Estimates capitalized startup assets only for launch, plus an optional contingency reserve.
!
Exclusions This calculator includes only capitalized startup assets. It excludes inventory, payroll runway, deposits, debt service, working capital, rent, insurance premiums, billing delays, receivables, marketing runway, and other operating expenses.
How should founders build a home infusion business funding plan?
For a Home Infusion Therapy Service, the funding plan should tie launch timing, patient ramp-up, reimbursement lag, and nurse utilization to cash needs before you raise money. Here’s the quick math: the base case uses 29 Year 1 clinicians and specialists, 40 to 60 monthly treatments per clinician, $350 to $750 per treatment, and a Year 1 capacity funding plan that must cover $240,000 CAPEX, $905,000 minimum Month 1 cash, $18,100 monthly fixed overhead, and about $39,750 in admin payroll.
Build the ramp model
Map launch by week, not quarter.
Link visits to clinician count.
Use 40 to 60 treatments monthly.
Test reimbursement lag in cash flow.
Set the raise size
Fund $240,000 CAPEX first.
Keep $905,000 minimum cash ready.
Cover $18,100 fixed overhead monthly.
Protect against variable cost swings.
How much does it cost to start a home infusion business?
A Home Infusion Therapy Service needs about $1.145 million to start: $240,000 in CAPEX plus $905,000 minimum Month 1 cash, not just equipment; see What Are The Operating Costs Of Home Infusion Therapy Service? for the cost stack behind that runway.
Startup Funding
$240,000 CAPEX base plan
$905,000 Month 1 cash need
$1.145 million total opening funding
Separate buildout from payroll runway
Year 1 Model
$5.467 million first-year revenue
29 field clinicians and specialists
$350–$750 per treatment
Fund claims lag, supplies, insurance, compliance
What hidden costs of starting a home infusion business get missed?
The biggest miss in a Home Infusion Therapy Service is working capital, not CAPEX: the model shows $905,000 minimum cash in Month 1, plus $18,100 in monthly fixed costs and $39,750 in monthly management payroll. If you’re planning the launch, read How To Write A Business Plan To Launch Home Infusion Therapy Service? with this in mind. Receivables float is separate from startup assets, and Year 1 also carries 85% medical consumables and IV kits, 45% specialty pharmacy procurement fees, 50% nurse travel and mileage reimbursement, and 30% billing and claims processing fees.
Cash needs first
$905,000 Month 1 cash floor
$18,100 monthly fixed costs
$39,750 monthly management payroll
Pay staff before reimbursement
Costs people miss
Credentialing delays slow cash
Malpractice coverage adds cash load
24/7 on-call readiness costs real money
Cold-chain and audit work creates waste
Calculate Fuding Needs
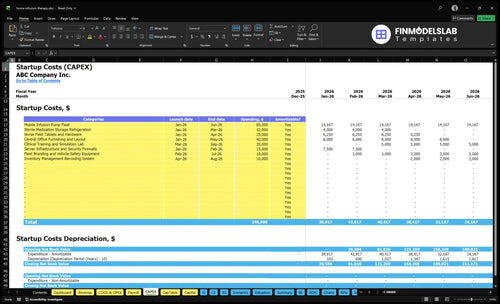
Startup cost summary
This table shows startup CAPEX and excluded launch cash for a home infusion therapy service.
Highlighted CAPEX$240,000Base planning example
Excluded cash needs$905,000Outside CAPEX total
Funding need$1,145,000CAPEX + excluded cash needs
Cost Category
Base Estimate
Main Cost Driver
CAPEX Calculator
Mobile infusion pump fleet and clinical equipment
$85,000
Pump count and deployment scope
Yes
Facility setup and office furnishing
$40,000
Buildout scope and furniture needs
Yes
Staff readiness and simulation training
$35,000
Training depth and onboarding volume
Yes
Field technology and security setup
$40,000
Tablet count and security hardware
Yes
Sterile storage, fleet safety, and inventory systems
$40,000
Cold storage, vehicle gear, and tracking tools
Yes
Month 1 cash buffer
$905,000
Fixed overhead, billing lag, and payroll runway
No
Home Infusion Therapy Service Core Five Startup Costs
Regulatory Setup, Licensing, Accreditation, and Payer Enrollment Startup Expense
Licensing Scope
State licensure, home health or nursing agency rules, pharmacy permits if you dispense, accreditation prep, Medicare supplier enrollment if applicable, commercial payer credentialing, policies, and clinical protocols can’t be priced with one national number. State, payer mix, clinical scope, and pharmacy model set the cost and timeline.
Budget Drivers
Build it from state filing fees, consultant hours, policy and protocol drafting, survey prep, and enrollment work. Get quotes by state and payer, then budget months of coverage for delayed approvals. This expense lives inside the $905,000 minimum Month 1 cash plan because revenue can lag the hire and launch date.
Cash Timing
Approval timing matters as much as the fee. Delayed credentialing can leave nurses on payroll before claims are paid, which strains receivables and cash. Keep quality assurance and compliance audits at $1,200 per month, and stage launch dates only after the slowest license and payer path is mapped.
Payer Delay Risk
If payer enrollment slips, payroll still goes out and receivables arrive late. That is why licensing, accreditation readiness, and credentialing belong in launch cash, not in a future bucket. Tie the budget to the slowest approval path and keep enough runway for the first claim cycle.
Clinical Equipment, Infusion Devices, and Patient-Care Asset Startup Expense
Reusable assets
Separate one-time gear from disposables. Reusable CAPEX totals $160,000: $85,000 pump fleet, $12,000 sterile refrigeration, $35,000 training lab, $18,000 fleet branding and safety gear, and $10,000 barcoding. That base covers infusion pumps, ambulatory pumps, IV poles, emergency kits, PPE setup, sharps containers, secure storage, and cold-chain assets.
What to price
Price the fleet by unit count, quote, and service life. Add calibration, maintenance, and spare-unit assumptions for infusion pumps and refrigeration, plus cold-chain checks for medication storage. One clean rule: if it touches medication or the patient, it needs an asset record, a service plan, and a replacement path.
Count devices by nurse route
Quote service intervals separately
Track spares as backup stock
Keep disposables in ops
Do not load IV kits, PPE, sharps containers, and single-use supplies into startup CAPEX. Put them in operating costs, with Year 1 medical consumables and IV kits at 85% of revenue. That keeps spend tied to visits, so higher volume raises supply cash need and slower ramp lowers it.
Cash timing
Buy reusable assets before the first home visit, then fund disposables as treatments start. Secure storage, barcoding, and safety gear reduce waste, but they do not remove cash pressure. If calibration or onboarding slips, cash gets stuck in idle equipment while supply orders still start with the first patient.
Technology, Billing, Scheduling, and HIPAA Systems Startup Expense
Core Stack
A home infusion start needs electronic health record, electronic medication administration record, scheduling, route planning, secure messaging, billing, and HIPAA controls. This budget separates hardware CAPEX from subscriptions: $25,000 for nurse field tablets and hardware, $15,000 for servers and firewalls, and $1,800 per month for EHR and HIPAA-compliant software.
Budget Build
Build this line item from units × unit price, plus implementation fees and months of coverage. The Year 1 software run rate is $21,600 at $1,800 per month, before claims processing. Billing and claims fees run at 30% of revenue in Year 1, so cash needs rise fast as volume grows.
Count devices by nurse count.
Get firewall and server quotes.
Model 12 months of software.
Trim Waste
Keep the hardware list tight and buy only what field staff need on day one. Tie tablets, phones, and access rights to roles, not headcount guesses. Ask vendors to itemize implementation, training, and support separately, and avoid signing for extra modules before dispatch, charting, and claims are live.
Cash Risk
Secure messaging, billing tools, and route data all carry protected health information, so firewalls and access logs matter from day one. The real squeeze is timing: 30% of revenue goes to billing and claims in Year 1, while software still costs $1,800 each month, so slow collections can hit payroll fast.
Staffing Readiness, Recruiting, Training, and Pre-Opening Payroll Startup Expense
Startup Scope
Recruiting, RN onboarding, competency validation, infusion training, clinical director time, administrator time, background checks, credentialing, and on-call setup belong in startup expense, not CAPEX. The Year 1 plan needs 29 clinicians and specialists across five service lines, so these costs hit cash before first reimbursement and should be funded up front.
Payroll Build
Management payroll is based on a Clinical Director at $145,000, an Operations Manager at $95,000, two Patient Care Coordinators at $65,000 each, a Billing Specialist at $55,000, and an Intake Coordinator at $52,000. That totals about $39,750 per month before taxes and benefits, or $477,000 a year.
Add payroll taxes separately.
Fund pre-opening coverage.
Track credentialing lead time.
Hire Pace
Capacity starts at 450% to 700%, so hiring should follow referral flow, not the org chart. Start with the staff needed for first-day coverage, then add people as patient starts rise. The real drag is payroll sitting ahead of collections, so every early hire adds working-capital pressure.
Match hires to referral ramp.
Use temporary help first.
Delay nonessential roles.
Budget Inputs
Estimate this startup line from headcount, onboarding hours, credentialing quotes, background check fees, training days, and months of pre-opening coverage. What this estimate hides is timing: if payer cash comes late, payroll lands first. That is why staffing readiness belongs in startup cash, alongside the other launch costs.
Insurance, Professional Services, and Risk-Management Startup Expense
Coverage Stack
Insurance and legal setup here includes general liability, professional liability, malpractice, workers’ compensation, cyber liability, policy manuals, accounting, billing compliance review, and contracting support. Price it from quotes, not a national average: clinical risk, state rules, staff count, service mix, payer contracts, and claims history all move the number. This model carries $4,200/month for malpractice and professional liability plus $1,200/month for quality assurance and compliance audits.
Quote Inputs
Build the estimate from policy lines and annual reviews. Separate one-time legal setup and policy writing from recurring premiums and audits. Ask for quotes that show state-specific rules, staff count, service mix, and payer contract terms.
Compare each coverage line separately.
Check renewal timing before launch.
Keep audit and legal fees visible.
Keep It Tight
Keep the spend tight by updating policies when scope changes, training nurses on documentation, and reviewing billing before claims go out. Don’t cut limits just to save cash; one gap in worker injury, malpractice, or cyber coverage can cost more than the policy. Clean files also help at renewal.
Review denials every month.
Log incidents right away.
Refresh contracts yearly.
Cyber Control
Cyber risk is real because field tablets, secure messaging, billing systems, and protected health information all touch one workflow. The $1,200/month audit line should test access controls, device rules, and billing compliance before a breach or claim turns into a bigger repair bill.
Compare 3 Startup Cost Scenarios
Scenario table
Lean trims assets and territory; Base matches the researched model; Full adds inventory, infrastructure, and staff, so cash needs rise fast as scope expands.
Lean, Base, and Full show how launch scope changes startup cash need.
Scenario
Lean LaunchSetup light
Base LaunchPayer ready
Full LaunchAsset heavy
Launch model
Uses a partnered pharmacy, a limited territory, and a smaller first-pass care team.
Uses owned core equipment, a central office, and the full Year 1 staffing plan.
Adds broader service lines, larger staff, owned inventory, and more infrastructure for wider reach.
Typical setup
Runs with a light office, fewer pumps, and tight referral focus.
Uses $240,000 CAPEX, $905,000 minimum Month 1 cash, 29 Year 1 clinicians and specialists, $18,100 monthly fixed costs, and $5.467 million Year 1 revenue.
Runs with expanded clinical coverage, pharmacy-related buildout, and more working capital.
Cost drivers
Partnered pharmacy
smaller pump fleet
lighter office setup
referral development
working capital
Pump fleet
office and storage
liability insurance
staffing
EHR and billing
Owned medication inventory
pharmacy infrastructure
larger staff
more working capital
broader service lines
Planning rangeCAPEX only
Lower funding bandLow cash risk
$240,000Owned assets
Higher funding bandHigh cash risk
Best fit
Fits founders who want a narrow launch with less owned equipment and a lighter office.
Fits teams that want the full modeled launch and clear payer operations.
Fits operators ready to fund scale and absorb more startup risk.
!
Planning note: Ranges are researched planning assumptions, not vendor quotes or fixed funding offers.
Use the model’s $905,000 minimum cash in Month 1 as the base funding target, not just the $240,000 CAPEX number That reserve covers more than equipment It protects payroll, compliance setup, insurance, supplies, and billing lag while first-year revenue ramps toward the $5467 million planning assumption
Not always it depends on state rules and your service model This plan includes specialty pharmacy procurement fees at 45% of revenue and $12,000 for sterile medication storage refrigeration, but it does not include a full pharmacy buildout If you own dispensing or sterile compounding, budget scope changes materially
The data does not give a fixed payer-enrollment timeline, so treat it as a cash-risk item The model starts costs in Month 1, including $18,100 in monthly fixed overhead and about $39,750 in monthly management payroll If billing approval lags, the $905,000 cash cushion becomes the safety net
Start with patient-care assets that directly support safe visits and billable treatments The largest line is the $85,000 mobile infusion pump fleet, followed by $40,000 for office layout, $35,000 for the clinical training and simulation lab, and $25,000 for nurse field tablets Keep disposable supplies separate from CAPEX
The base model assumes $5467 million in first-year revenue That comes from 29 clinicians and specialists, Year 1 treatment prices from $350 to $750, and capacity assumptions from 450% to 700% depending on service line The key test is whether referrals can fill that utilization without overhiring
About the author
Victor Shaw
Practical Business Analyst
Victor Shaw is a practical business analyst at Financial Models Lab who writes about small business budgeting and estimating what a business can earn. He helps aspiring small business owners build realistic assumptions, understand break-even points, and compare business opportunities with greater clarity. His work focuses on simple, credible financial analysis that turns rough ideas into grounded expectations for real-world decision-making.
Choosing a selection results in a full page refresh.