IV Ketamine Therapy Clinic Startup Costs With $93k Monthly Fixed Burn
IV Ketamine Therapy Clinic
You’re opening a medical clinic, so the real budget is more than chairs and monitors This startup cost breakdown separates IV ketamine clinic CAPEX from pre-opening expenses, working capital, and the first operating year model, where researched assumptions show $932k in monthly payroll plus fixed overhead before revenue-linked costs The planning outcome is a total funding need that covers buildout, equipment, compliance, launch costs, and cash runway until patient volume reaches break-even
IV Ketamine Clinic CAPEX Calculator
Startup CAPEX Calculator
Estimates capitalized startup assets only for an IV ketamine therapy clinic.
!
What this leaves out This calculator includes only capitalized startup assets. It excludes payroll ramp, marketing launch, licensing fees, insurance premiums, EHR subscriptions, exam and supply inventory, deposits, debt service, and working capital.
Labor is the biggest cost driver in an IV Ketamine Therapy Clinic; room count, chair count, equipment, and compliance matter, but staffing and ramp matter most. With 1 medical director, 1 nurse practitioner, 2 registered nurses, 1 clinical psychologist, 1 clinic administrator, and 1 medical assistant in Year 1, labor scale hits about $742k per month. Here’s the quick math: Year 1 utilization brings in about $856k monthly revenue against $932k of fixed payroll and overhead, so opening too fast can squeeze cash.
Core cost drivers
Treatment rooms set buildout cost.
Infusion chairs cap daily volume.
Monitoring gear adds fixed spend.
Emergency readiness raises setup cost.
Scale and cash pressure
Labor is the largest fixed driver.
Lease condition changes startup cash.
Location shifts rent and staffing.
Payer strategy affects payback speed.
How should I build an IV ketamine clinic funding plan?
For an IV Ketamine Therapy Clinic, build the plan as a clean sources and uses table: fund CAPEX, pre-opening costs, deposits, startup supplies, recruiting and training, legal and compliance, launch marketing, and working capital. Here’s the quick math: if fixed payroll and overhead are $932k and contribution is 80%, Year 1 break-even revenue is about $1.165M per month ($932k ÷ 0.80). That means you should tie launch timing to Month 1 expenses and a 60-month model before any lender or investor review.
Sources and uses
Founder cash covers early outlays
Investor capital funds launch gaps
Lender debt supports fixed build costs
Equipment financing lowers upfront cash
Model checks
Validate Year 1 assumptions first
Compare $856k monthly implied revenue
Test against $179k full scheduled volume
Keep an operating reserve in cash
What hidden costs should I expect when opening an IV ketamine clinic?
Hidden costs for an IV Ketamine Therapy Clinic are mostly compliance and operating setup, not just equipment. If you want to track the right numbers from day one, use What Are The 5 Core KPIs For IV Ketamine Therapy Clinic Business? and keep these costs separate from CAPEX. A realistic monthly base case is about $48,800 for malpractice, general liability and property insurance, training, EHR, utilities, and medical waste, before legal and licensing work.
Monthly burn
$35,000 malpractice coverage
$600 general liability and property insurance
$400 staff training
$800 EHR setup and use
Setup items
DEA registration where applicable
State controlled-substance rules
Healthcare attorney review
Medical director and protocol work
Clinic buildout
Written consent documents
Policy development and onboarding
Billing workflows and credentialing
Medical waste setup
Cash risk
$12,000 monthly utilities and medical waste
Costs vary by state
Costs vary by ownership model
Keep runway separate from CAPEX
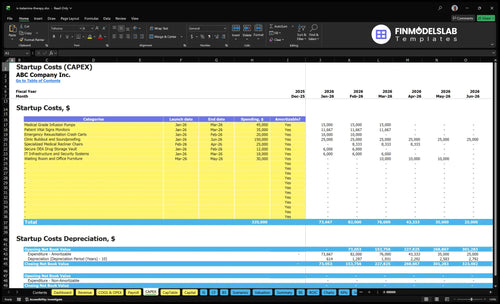
IV Ketamine Clinic Startup Cost Breakdown Table
Startup Cost Summary
This table shows the main clinic buildout, equipment, and operating cash needed to open and fund early care.
Highlighted CAPEX$275,000Base planning example
Excluded cash needs$657,000Outside CAPEX total
Funding need$932,000CAPEX + excluded cash needs
Cost Category
Base Estimate
Main Cost Driver
CAPEX Calculator
Clinic Buildout and Soundproofing
$150,000
Suite construction, acoustic treatment, and patient-room finish work
Yes
Medical Grade Infusion Pumps
$45,000
Number of infusion pumps and medical-grade specification
Yes
Patient Vital Signs Monitors
$35,000
Monitor count, alarm features, and clinical monitoring standard
Yes
Specialized Medical Recliner Chairs
$25,000
Chair count and durability for infusion-room use
Yes
Emergency Resuscitation Crash Carts
$20,000
Emergency readiness setup and cart specification
Yes
Operating Cash Reserve
$657,000
Year 1 payroll, lease, insurance, and launch cash gap to the Month 12 trough
No
IV Ketamine Therapy Clinic Core Five Startup Costs
Leasehold Improvements and Clinical Space Setup Startup Expense
Buildout Scope
For an IV ketamine clinic, leasehold improvements cover treatment rooms, reception, intake, recovery, staff space, ADA access, privacy, signage, plumbing, electrical, secure medication storage, and patient flow. Cost changes sharply with square footage, landlord delivery, market rent, and whether the suite already works as a medical office. Use $12k/month as the lease anchor.
Cost Inputs
Separate the startup space budget into lease deposit, renovations, signage, furniture, and ongoing rent. At $12k per month, rent is $144k a year before any other occupancy costs. The key inputs are square feet, tenant improvement scope, and the landlord’s delivery condition.
Cost Control
The lowest-risk path is a suite that already functions as a medical office, because plumbing, electrical, privacy, and controlled-medication storage are closer to spec. That trims rebuild work and shortens time to open. Don’t overspend on cosmetic finishes; spend where compliance and patient flow depend on it.
Rent Anchor
Treat $12k/month as fixed facility overhead from day one, or $144k a year. If the landlord delivers a shell, buildout can outrun rent; if the suite is near medical-ready, the first cash need shifts to deposit, furniture, and working capital. That one split drives most of the budget gap.
Infusion Equipment, Monitoring, and Emergency Readiness Startup Expense
Room Set
Budget this as a per-room set plus a shared clinical pool. For each active infusion room, count one chair or recliner, one IV pump, one vital sign monitor, one pulse oximeter, exam supplies, and treatment furniture. Match the count to the room count and Year 1 coverage from 2 registered nurses plus provider coverage. Vendor quotes are still needed because unit prices were not provided.
Shared Kit
Oxygen setup, emergency cart items, and clinical storage are usually shared across the suite, not bought room by room. Add signage, privacy items, and backup supplies once, then map them to opening-day patient volume. The budget input you need is quantity by room plus one shared set, not a single lump sum.
Count active rooms first
Split shared from room-level
Get written vendor quotes
Phased Buy
Buy the opening-day equipment first, then expand as patient flow and staffing support more rooms. That keeps spend aligned with the schedule that 2 RNs and provider hours can cover. The common mistake is buying for future scale before the clinic has steady volume.
Reserve
Set a replacement reserve for wear items and a contingency for shipping, install, or quote gaps. Since this research has no unit prices, keep the launch budget flexible until you have vendor bids for chairs, pumps, monitors, oxygen, and emergency gear.
Licensing, Compliance, Legal Setup, and Medical Governance Startup Expense
Governance Setup
If you’re opening an IV ketamine clinic, this bucket covers entity formation, healthcare attorney review, state medical board checks, DEA registration where needed, controlled-substance rules, storage policies, consent forms, operating protocols, the medical director agreement, and physician oversight. Use $320k for a 1 FTE medical director in Year 1; costs vary by state, ownership model, and scope. This isn’t legal advice.
Cost Inputs
Estimate this line by pricing formation, counsel, filing fees, policy drafting, and oversight documents, then add 12 months of director coverage. Here’s the quick math: 1 FTE × $320k sets the governance floor before state-specific filings and reviews.
Get filing quotes first
Price counsel separately
Map state rules early
Keep It Tight
Keep one clean policy set, one consent package, and one oversight structure. That cuts rework without cutting compliance. The biggest mistake is launching with generic forms or a loose storage policy, then paying counsel again after the state or board flags a gap.
Review state rules first
Finalize storage policies early
Use one oversight owner
Medical Director Anchor
The anchor here is the medical director: $320k for 1 FTE in Year 1. Treat that as the fixed governance cost, then layer in formation, attorney review, DEA registration, board work, and policy drafting. If scope changes, revisit oversight before opening.
Staffing Readiness, Recruiting, Training, and Pre-Opening Payroll Startup Expense
Pre-Open Payroll
Before the first infusion, this clinic pays for recruiting, credential checks, onboarding, training, clinical policies, scheduling, front desk intake, and billing setup. The core cost is people, not supplies. For Year 1, the staffing plan totals $890k, so this line item should be funded as pre-opening payroll, not mixed into normal operating cash.
Year 1 Staffing
Budget from headcount times salary, plus hiring and training time. The Year 1 model includes 1 medical director at $320k, 1 nurse practitioner at $145k, 2 registered nurses at $95k each, 1 clinical psychologist at $110k, 1 clinic administrator at $75k, and 1 medical assistant at $50k.
Control Burn
Keep hiring tight and stage start dates so payroll turns on only when the suite, policies, and workflows are ready. The common mistake is carrying full team payroll too early. With $890k annual payroll, every month of delay matters, so lock the open date, use contract help where allowed, and separate pre-opening payroll from ongoing working capital.
Runway Split
Pre-opening payroll is a startup cash need; ongoing payroll is an operating expense. On a straight-line basis, $890k a year averages about $74.2k per month. Fund enough cash to cover recruiting, training, and early staffing before patient volume stabilizes, then move payroll back into normal monthly operating cash.
Technology, Insurance, Initial Supplies, and Launch Infrastructure Startup Expense
Tech and insurance
This bucket is both a setup cost and a monthly burn. Expect $800 a month for EHR and scheduling, $35,000 a month for malpractice, and $600 a month for general liability and property insurance. Add one-time phone, website, payment system, branded materials, and patient intake setup.
What to budget
Price it in two parts: fixed subscriptions plus launch spend. Variable costs are tied to revenue: 45% for pharmaceuticals and ketamine supply, 30% for disposable supplies and IV kits, 100% for digital marketing and referral outreach, and 25% for payment processing. You need a revenue forecast to size this line.
Setup items
One-time setup covers the phone system, website, payment tools, branded pieces, and patient intake materials. These are small next to insurance, but they hit cash early. Treat them as launch cash, not overhead, so you can separate day-one spend from month-to-month operating cost.
Watch renewals
Flag malpractice, general liability, and property insurance renewals as recurring obligations, not one-time fees. That keeps the runway honest and avoids a cash crunch when coverage renews. If marketing is front-loaded and supply use tracks revenue, the launch budget needs enough cash for the first months, not just the opening week.
Lean, Base, and Full-Service IV Ketamine Clinic Startup Cost Scenarios
Scenario table
Lean cuts rooms and staff, Base matches the Year 1 model, and Full adds rooms, coverage, and marketing. Fixed payroll plus overhead is about $93.2k/month before variable costs.
Lean, Base, and Full launch cost comparison
Scenario
Lean LaunchLower capital risk
Base LaunchBalanced launch
Full LaunchHigher fixed-cost risk
Launch model
Starts with fewer treatment rooms and lighter staff coverage than the Year 1 model, so it depends on high room use.
Matches the Year 1 staffing plan and keeps the service mix balanced across infusions, psych support, and admin.
Adds more rooms, broader staffing, and heavier launch spend to push volume earlier, but fixed costs rise fast.
Typical setup
One or two rooms, tighter scheduling, and only the core equipment needed to start.
Standard clinic flow with the Year 1 team, core infusion gear, and enough space for steady throughput.
Multiple rooms, stronger patient flow, more support staff, and extra buffer for the opening ramp.
Cost drivers
Smaller buildout
fewer treatment rooms
lean staffing
lower launch marketing
smaller working capital
Year 1 staff mix
standard buildout
core infusion equipment
normal launch marketing
month 12 cash buffer
More treatment rooms
larger buildout
broader staffing coverage
heavier launch marketing
larger working capital
Planning rangeCAPEX only
$700,000 - $900,000Lower risk
$900,000 - $1,100,000Balanced launch
$1,200,000 - $1,600,000Higher risk
Best fit
Best for founders testing demand with lower capital risk and a narrow local catchment.
Best for operators who want the Year 1 plan with a measured cash buffer and balanced risk.
Best for funded teams that want faster brand build and can carry higher fixed-cost risk.
!
Planning note: These scenario ranges are researched planning assumptions, not exact quotes, and they should be used as launch bands rather than vendor bids.
Reserve enough to cover the gap between fixed costs and stable patient volume The model shows about $932k per month in payroll plus fixed overhead before revenue-linked costs At Year 1 utilization, implied monthly revenue is about $856k, so early cash reserve matters CAPEX, debt service, and owner draws are separate
The launch ramp can affect cash needs through the first operating year Year 1 capacity assumptions range from 400% for the clinical psychologist to 500% for several roles, while later years rise toward 800% to 850% If patient volume builds slowly, working capital must cover payroll, rent, insurance, and software before break-even
More rooms can help only if demand and staffing support them The base model already includes 1 medical director, 1 nurse practitioner, 2 registered nurses, 1 clinical psychologist, 1 administrator, and 1 medical assistant in Year 1 Adding rooms raises buildout and equipment costs, so it should be tied to scheduled treatments, utilization, and provider coverage
Treat buildout, equipment, furniture, IT hardware, and signage as CAPEX Treat legal setup, licensing, insurance deposits, EHR setup, recruiting, training, launch marketing, and startup supplies as pre-opening expenses Then add working capital for monthly obligations, including the $12k facility lease, $35k malpractice insurance, and $800 EHR subscription
Using the researched Year 1 model, break-even revenue is about $1165k per month before debt service and owner draws The math is $932k in fixed payroll plus overhead divided by 80% contribution after 75% clinical supply costs and 125% marketing plus processing At Year 1 utilization, implied revenue is about $856k per month
About the author
Gregory Ford
Launch Planning Specialist
Gregory Ford is a launch planning specialist at Financial Models Lab who helps first-time entrepreneurs judge whether a business idea is financially realistic. He focuses on operating cost estimates and turns broad business questions into clear planning assumptions and practical next steps. Gregory writes about opening and running small businesses in a straightforward, easy-to-understand way.
Choosing a selection results in a full page refresh.