Laser Eye Surgery Center Startup Costs for a 2-Surgeon Launch
The cost to start a laser eye surgery center is the sum of quote-based CAPEX, pre-opening spend, contingency, and working capital the supplied model does not include vendor quotes for lasers, buildout, or diagnostic equipment Based on researched planning assumptions, the opening operation has $210,000 in monthly revenue potential at Year 1 capacity, with $128,833 in known monthly payroll and fixed overhead before revenue-linked costs At the modeled Year 1 volume, technology fees, supplies, marketing, and payment processing add 160% of revenue, or about $33,600 per month A 3-month working-capital reserve for known payroll and fixed overhead alone equals about $386,500, before laser deposits, buildout, launch marketing, financing fees, or operating losses
Calculate Fuding Needs
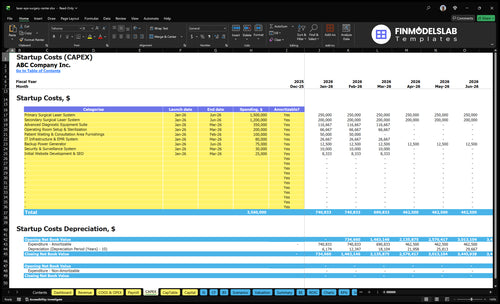
Startup cost summary
This table separates upfront equipment, buildout, and non-CAPEX cash needs for opening the clinic.
Highlighted CAPEX$3,430,000Base planning example
Excluded cash needs$2,439,000Outside CAPEX total
Funding need$5,869,000CAPEX + excluded cash needs
Cost Category
Base Estimate
Main Cost Driver
CAPEX Calculator
Laser systems
$2,700,000
Primary and secondary surgical laser systems
Yes
Diagnostic equipment suite
$350,000
Advanced diagnostic equipment and testing setup
Yes
Operating room buildout and sterilization
$200,000
Surgical room buildout, sterile finishes, and setup
Yes
IT infrastructure and EMR system
$80,000
Clinical software, records system, and network hardware
Yes
Patient area furnishings
$100,000
Waiting room and consultation area fit-out
Yes
Opening cash buffer
$2,439,000
Monthly payroll, rent, insurance, IT, and compliance before breakeven
No
Estimate Startup Costs with Calculator
Startup CAPEX Calculator
Estimates pre-opening capitalized assets for a laser eye surgery center only.
!
CAPEX scope This calculator covers pre-opening capital assets only. It excludes inventory, payroll runway, opening-month rent, working capital, debt service, taxes, marketing runway, and operating losses. Use a separate funding-need view for those cash items.
Launch scale changes the cash need fast: shared laser access and a smaller buildout can trim upfront spend, while a fuller clinic with more staff and marketing pushes the funding need higher.
Lean, base, and full launch funding bands
Scenario
Lean LaunchLower build
Base LaunchYear 1 plan
Full LaunchScale-up plan
Launch model
Use shared or leased laser access, keep the buildout small, and open with limited diagnostics and lighter marketing.
Use the Year 1 operating plan with 2 surgeons, 1 optometrist, $4,500 procedures, 40 monthly treatments per surgeon, and 55% surgeon capacity.
Build for a larger clinic with stronger marketing, fuller diagnostics, and growth toward 4 surgeons and 85% surgeon capacity by Year 5.
Typical setup
One surgeon-led start with a small support team and basic patient flow.
Fully owned laser systems, standard diagnostics, and the core Year 1 clinical team.
Bigger launch team, more diagnostic depth, and a wider patient funnel from day one.
Cost drivers
Shared laser access
smaller buildout
lean staffing
basic diagnostics
lighter marketing
Laser systems
diagnostic equipment
surgeon payroll
facility rent
patient acquisition
More surgeons
more technicians
stronger marketing
fuller diagnostics
more working capital
Planning rangeCAPEX only
Below base fundingLean funding
$6.0MBase funding
Above base fundingScale-up funding
Best fit
Founders testing demand before buying a full laser stack.
Operators who want the supplied Year 1 plan as written.
Teams that want faster volume growth and can fund a heavier launch.
!
Planning note: These scenario ranges are planning assumptions built from the model's quoted capex, staffing, and cash burn, not live vendor quotes or exact lender terms.
How much does it cost to open a LASIK center?
A Laser Eye Surgery Center should plan for at least $386,500 in working-capital reserve before laser deposits, buildout, vendor-quoted equipment CAPEX, and contingency. For performance tracking after launch, tie that funding plan to What Is The Most Important Metric To Measure The Success Of Your Laser Eye Surgery Center?, because revenue volume drives cash safety.
What hidden costs affect a laser eye surgery center opening budget?
The budget surprise is usually not the laser itself; it’s the cash-heavy setup around it. For a Laser Eye Surgery Center, hidden pre-opening costs like $4,000 monthly malpractice insurance, $1,000 general liability, $1,500 regulatory setup, and $1,200 legal/accounting hit before the first procedure. What this hides: launch marketing can run at 60% of Year 1 patient acquisition spend, and payment processing can take 20%, even though none of this is laser equipment.
Pre-opening cash costs
$4,000 monthly malpractice insurance
$1,000 general liability
$1,500 regulatory compliance
$1,200 legal and accounting
Launch items that drain cash
Staff onboarding, credentialing, training
Deposits and equipment service agreements
Patient financing setup fees
20% payment processing, 60% Year 1 marketing
What should a laser eye surgery center funding plan include?
A Laser Eye Surgery Center funding plan should show exactly where capital goes, when the center opens, and how long cash lasts before anyone calls it break-even. Lenders and investors should see a use-of-funds schedule, CAPEX quotes, startup expenses, launch timing, surgeon compensation, diagnostic volume, procedure pricing, patient financing assumptions, a working capital reserve, and a debt schedule, all tied to Year 1 assumptions of $4,500 per refractive surgery, 40 monthly treatments per surgeon, 100 optometry visits at $200 each, and the known $128,833 monthly payroll plus fixed overhead.
Money Uses
Use-of-funds by category
CAPEX quotes and timing
Startup and launch costs
Working capital reserve amount
Operating Assumptions
$4,500 Year 1 procedure price
40 monthly treatments per surgeon
100 optometry visits at $200
Show cash runway before break-even
Key Takeaways
Upfront laser and buildout costs sit outside monthly rent.
Usage fees and royalties drive cost of goods sold.
Monthly occupancy adds $17,500 before any procedures.
Payroll and launch marketing dominate first-year cash burn.
Laser Eye Surgery Center Core Five Startup Costs
Ophthalmic Laser Systems Startup Expense
Laser stack
An ophthalmic laser system is not one price. Budget separate quotes for the excimer laser, femtosecond laser, software, installation, calibration, warranties, and maintenance contracts; then track treatment cards, royalties, and per-click charges as usage-based cost of goods sold, not CAPEX. The model assumes technology fees and royalties of 50% of revenue in Years 1 and 2, 48% in Year 3, and 45% in Years 4 and 5.
Buy or lease
Use separate lines for upfront CAPEX and usage-based COGS. Compare purchase, financed purchase, lease, and shared-use by asking for the equipment quote, install fee, service terms, and per-click schedule. Shared-use lowers cash at launch, but it can raise unit cost if case volume is light.
Get itemized vendor quotes
Price per-click usage separately
Match terms to case volume
Watch the margin
Don’t bury royalties inside equipment cost. If revenue is small in Year 1, a 50% technology fee and royalty burden can eat cash fast, so the real question is not just what the laser costs, but how often it is used and what each click costs. Lock service response times and warranty coverage before signing.
Separate fixed and variable costs
Check warranty and service limits
Model low-volume months first
Cost split
For this startup, the clean budget split is simple: CAPEX for the laser platform, software, install, and calibration; COGS for treatment cards, royalties, and per-click fees. That split keeps launch funding honest and makes gross margin usable from day one, especially when equipment is acquired through lease or shared-use rather than cash purchase.
Diagnostic and Clinical Equipment Startup Expense
Diagnostic Scope
Diagnostic readiness is a separate startup line, not part of the laser buy. It covers corneal topography, wavefront measurement, pachymetry, autorefractors, slit lamps, dry eye tools, exam lanes, patient screening systems, planning software, and follow-up care gear.
Cost Inputs
Build the estimate from units × quote, then add installation, maintenance, and IT integration. The model should fit 150 diagnostic technician appointments per month at 500% capacity and 100 optometrist visits at $200 in Year 1, so underbuying gear can choke throughput.
Control Spend
Save money by buying only what supports Year 1 flow, then stage extras later. Ask vendors to break out purchase price, installation, and service terms, and avoid rolling these assets into laser pricing. The mistake is paying for features you won't use; the risk is weak exam flow and longer patient waits.
Volume Match
This spend should scale with clinic throughput, not just the procedure room. If diagnostic capacity lags the Year 1 plan, the center loses screening speed before surgery starts. Keep the equipment list tied to visit volume and separate every quote into capital, maintenance, and software lines.
Staffing, Launch Marketing, and Opening Supplies Startup Expense
Pre-Opening Payroll
Before the first procedures, cover recruiting, onboarding, credentialing, and clinical training for 2 refractive surgeons, 1 optometrist, 2 surgical technicians, 1 diagnostic technician, 1 patient coordinator, and 1 clinic manager. The Year 1 payroll floor is at least $100,833 per month, so opening cash must fund hiring time, not just day-one wages.
What It Must Cover
This bucket also pays for front-desk setup, patient counseling, and the patient financing workflow, plus surgical consumables, medications, and sterile supplies used before the first case. Estimate it with headcount × training months, then add quoted supply packs and onboarding tools. It sits on top of rent and equipment, not inside them.
Marketing Reserve
Launch marketing is a variable startup cost, not a fixed ad fee. Use 60% of revenue as the source assumption, so the budget scales with planned patient volume and procedure mix. One clean rule: if revenue ramps late, the ad spend reserve still has to bridge lead generation and follow-up work.
Supply Reserve
Disposable medical supplies are modeled at 30% of revenue, so the opening budget must fund sterile packs, medications, and case-day consumables before collections catch up. Here’s the quick math: planned first-month revenue × 30% for supplies, plus 60% for launch marketing, before adding the $100,833 monthly payroll floor.
Licensing, Compliance, Insurance, and Professional Setup Startup Expense
Compliance Setup
Licensing, insurance, and professional setup is a launch gate, not a small admin task. Price one-time items like entity setup, contracts, legal review, accounting setup, HIPAA and OSHA policies, and accreditation support separately from recurring fees. The source monthly fixed cost base is $7,700.
Monthly Run Rate
Here’s the quick math: $4,000 malpractice insurance + $1,000 general liability + $1,500 regulatory compliance and licensing + $1,200 professional services = $7,700 per month. That excludes one-time entity formation, permits, and policy drafting, so keep setup costs off the monthly P&L.
What To Quote
Build the one-time budget from quotes for state medical facility requirements, physician licensing alignment, payer or patient financing setup, and any accreditation support. Use vendor and counsel bids for each workstream, then add monthly coverage for malpractice, liability, and compliance. If you blur setup and run rate, you’ll underfund opening.
Quote counsel by workstream.
Separate setup from renewal fees.
Map each license to one state.
Cost Control
Keep the fixed monthly load tight by reviewing coverage limits, only paying for needed services, and aligning contracts before opening. Don’t skip HIPAA and OSHA work to save cash; that usually costs more later. The real savings come from clean entity setup, right-sized insurance, and avoiding duplicate legal or accounting work.
Facility and Surgical Suite Buildout Startup Expense
Buildout Scope
A LASIK center buildout is not rent. It covers procedure room specs, consultation rooms, diagnostic lanes, a waiting area, sterile workflow, electrical load, HVAC stability, ADA access, leasehold improvements, permits, and inspections. Keep $15,000 monthly rent and $2,500 utilities out of CAPEX unless you show them in a separate funding-needs schedule.
Estimate Inputs
Here’s the quick math: buildout cost depends on square feet, room count, code upgrades, landlord allowance, permit fees, and inspection timing. Ask for contractor bids by room type, then add tenant improvements tied to medical use. The clean output should show buildout, deposits, and monthly occupancy costs as separate lines.
Quote room-by-room costs
Check landlord allowance first
Price permits and inspections
Keep It Separate
Don’t bury rent in startup CAPEX. Monthly occupancy should stay visible at $15,000 rent plus $2,500 utilities, while lease deposits stay in a funding-needs line if you include them. That split keeps startup cash needs honest and avoids overstating buildout.
Exclude ongoing rent from CAPEX
Track deposits separately
Show monthly occupancy costs
Budget Split
A clean budget shows three lines: facility buildout, lease deposits, and monthly occupancy. That structure helps lenders and founders see what is one-time cash versus recurring overhead, and it keeps the startup model aligned with the actual lease and permitting work.