Estimate the capitalized startup assets for a mandibular advancement device provider, not monthly operating spend or working capital.
!
Excluded items This calculator covers capitalized startup assets only. It excludes inventory, payroll runway, rent deposits, debt service, working capital, marketing, monthly operating expenses, and non-capitalized legal or regulatory fees.
What should the CAPEX and startup funding schedule show?
Open the Mandibular Advancement Device Provider Financial Model Template to see CAPEX by category, startup costs, launch timing, depreciation, and amortization. Then check whether runway covers $460,000 payroll, variable costs, remakes, onboarding, and slow collections.
Key screenshot highlights
Equipment, tech, furniture
Legal, training, payroll
$460k runway test
Mandibular Advancement Device Provider Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
How much money do I need to start a mandibular advancement device provider?
You need to fund the full launch, not just equipment; for a Mandibular Advancement Device Provider, the known Year 1 operating base is already $778,000, made up of $460,000 payroll plus $26,500 monthly fixed overhead. For the deeper profit logic, see How Increase Profits Mandibular Advancement Device Provider?, but treat all startup ranges as planning assumptions, not vendor quotes.
Known Funding Base
5,700 Year 1 units planned
$178 million Year 1 revenue model
$460,000 known annual payroll
$318,000 annual fixed overhead
Startup Cost Drivers
Outsourced fabrication lowers production CAPEX
Hybrid adds digital intake and CAD/CAM
In-house lab adds benches and technicians
Still fund compliance, insurance, software, runway
What hidden costs can underfund a mandibular advancement device provider?
A Mandibular Advancement Device Provider gets underfunded fast if you only budget for equipment and miss pre-opening and working capital. The big hidden costs are 15% quality testing, 10% sterilization compliance, 5% regulatory filing fees, 5% production waste, and 55% variable selling and card fees; if onboarding runs long, cash runway becomes the pressure point. For a deeper profit check, see How Increase Profits Mandibular Advancement Device Provider?
Cash before launch
Separate CAPEX from working capital
Budget pre-opening before first sale
Cover regulatory docs and labeling review
Expect provider onboarding delays
Hidden operating drag
Reserve 15% for testing
Reserve 10% for sterilization
Plan for 5% waste
Hold cash for shipping and card fees
Should a mandibular advancement device provider outsource fabrication or build a lab?
Outsource fabrication first for a Mandibular Advancement Device Provider. At 5,700 Year 1 units, in-house production already carries $12,000 monthly rent, $3,200 monthly maintenance, and two certified dental technicians at $85,000 each, before equipment, quality checks, and facility setup.
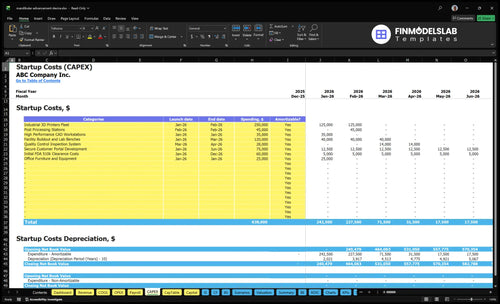
This table summarizes launch equipment, software, compliance, and the non-CAPEX cash needed to open and absorb early losses.
Highlighted CAPEX$550,000Base planning example
Excluded cash needs$744,000Outside CAPEX total
Funding need$1,294,000CAPEX + excluded cash needs
Cost Category
Base Estimate
Main Cost Driver
CAPEX Calculator
Industrial 3D Printers Fleet
$250,000
Printer count, install, and calibration
Yes
Facility Buildout and Lab Benches
$120,000
Lab buildout, benches, and utility work
Yes
Secure Customer Portal Development
$75,000
Custom workflow and patient data setup
Yes
Initial FDA 510(k) Clearance Costs
$60,000
Regulatory filing and launch compliance work
Yes
Post Processing Stations
$45,000
Finishing, curing, and inspection equipment
Yes
Working Capital Reserve
$744,000
Payroll, fixed overhead, and launch losses before breakeven
No
Mandibular Advancement Device Provider Core Five Startup Costs
Regulatory And Professional Setup Startup Expense
Formation Fees
Pre-opening setup covers entity formation, tax registrations, and state filings for a dental device business. Model regulatory filing fees at 0.5% of revenue as an operating cost, not CAPEX. One clean rule: if the entity is wrong, every contract and filing gets harder.
Docs And Review
This covers quality documents, labeling review, contract templates, supplier agreements, and privacy-aware workflows if patient data is handled. Treat drafting and review as pre-opening expense; only a specific software or tool gets capitalized. One sentence: build access limits and record rules before launch.
Advisor Run-Rate
Budget $500 per month for professional association dues as an operating expense starting at launch. Add advisor checks, filing support, and compliance planning to the same run rate. Here’s the quick math: annual dues total $6,000, so fixed overhead starts before the first sale.
Keep It Lean
Use templates, one qualified review pass, and supplier forms that match your real process. Keep FDA-related planning as a validation item with qualified counsel and compliance pros, not a guess. One sentence: spend on clean records and usable contracts, not heavy paperwork.
Physical Setup And Production Equipment Startup Expense
Lab Build-Out
If you build in-house, the big cost is the lab shell plus the machines. Budget for benches, curing or finishing tools, storage, ventilation, packaging space, and leasehold improvements, then add 3D printing or milling only if your workflow needs it. At $12,000 monthly rent, this is a fixed-cost bet on volume, not a light test.
Right-Sized Equipment
Use the Year 1 mix to size equipment depth: 5,700 total units, including 2,400 mandibular advancement devices, 800 tongue stabilizing devices, 400 premium adjustable splints, 1,500 cleaning kits, and 600 replacement liner sets. The $3,200 monthly maintenance contract belongs in operating cost, because uptime protects throughput.
Outsource low-volume steps first.
Buy only needed finishing tools.
Match storage to daily output.
Hybrid Setup
Don’t build a full lab just to look complete. Start with the gear that supports your real mix, then add milling or printing only when turn times or case complexity justify it. A smaller in-house finish area plus outside lab overflow can cut capex and keep maintenance tied to actual use.
Process Layout
Leasehold improvements should fit the flow: receiving, scan intake, fabrication, finishing, packing, and shipment. If the layout causes backtracking, labor costs rise fast. Treat the $3,200 monthly maintenance contract as a floor, then use preventive service so Year 1 volume does not get hit by downtime.
Digital Workflow And Software Startup Expense
Workflow Stack
The digital stack is mostly recurring spend, not equipment. Budget $2,500 per month for the CAD/CAM license starting Month 1, plus case tracking, secure file storage, provider portal, CRM, billing tools, computers, cybersecurity, and practice or lab integrations. Treat monthly subscriptions as operating or pre-opening expenses, not CAPEX, unless implementation is capitalized.
Cost Build
Build this cost from software months, user seats, setup work, and payment fees. The key inputs are months of coverage, number of users, and whether direct sales trigger 25% credit card processing fees and 30% sales commissions. Keep intraoral scanner spend conditional, since many referring dentists may already own scanners.
Count software months from Month 1.
Separate setup from recurring fees.
Use practice-owned scanners first.
Trim Spend
Do not buy the full stack before workflow is proven. Start with only the tools needed to scan, track cases, store files, and invoice, then add integrations after referral volume is real. The biggest trap is paying for hardware and subscriptions at the same time when a referring dentist already has the scanner.
Launch Burn
For launch budgeting, tie the software line to sales mix. If the workflow supports direct sales, the 25% payment fee and 30% commission can outrun the software bill fast, so model them as variable cost per dollar of revenue. That keeps the monthly burn honest before you scale case volume.
Initial Materials And Packaging Startup Expense
Opening stock
Stock the first buy as inventory, not equipment CAPEX. Use 2,400 mandibular advancement devices, 800 tongue stabilizing devices, 400 premium adjustable splints, 1,500 cleaning kits, and 600 replacement liner sets. Add labels, instructions for use, sample kits, and shipping supplies as separate supply lines.
Unit cost
Here’s the quick math: mandibular advancement device materials and handling are $50 before revenue-based costs, plus $300 medical-grade packaging, so $350 per unit. Premium adjustable splints are $75 plus $500 packaging, so $575. Tongue stabilizing devices are $40, cleaning kits $620, and replacement liner sets $1,350.
Quote labels by run.
Quote IFUs by kit count.
Quote shipping supplies by carton.
Remake reserve
Keep a separate remake allowance so defects do not hit gross margin. This reserve is an inventory buffer, not a machine purchase, and it should sit beside the opening buy until actual remake rates are known. The lean move is to hold the reserve in units, then convert it to dollars only after supplier quotes and pilot case data.
Do not mix it with equipment.
Do not bury it in payroll.
Reprice it after pilot runs.
COGS line
What this estimate hides: packaging, samples, and remake stock can move fast, but unit costs stay clean if you track them as cost of goods sold (COGS) inputs. That keeps startup cash honest and makes it easier to spot when a supplier quote change, not volume, is driving burn.
Commercial Launch Staffing And Insurance Startup Expense
Launch setup costs
Before the first sale, budget for website, SEO, provider outreach, sample materials, sales collateral, trade shows if used, technician training, operations training, customer support setup, and product liability planning. Treat these as pre-opening expenses, not CAPEX. The source model gives $6,500 per month for digital marketing and SEO and $1,800 per month for general liability insurance.
Staffing budget
Pre-opening payroll is the big ticket. Known annual salaries total $460,000: $175,000 for the chief executive officer, $115,000 for the lead biomedical engineer, and $85,000 each for two certified dental technicians. That is about $38,333 a month before commissions, so opening cash must cover staffing long before revenue lands.
Track payroll by launch month.
Train staff before first orders.
Keep support ready on day one.
Variable launch spend
Once revenue starts, use 30% sales commissions as a variable launch cost. Here’s the quick math: every $100,000 in sales brings $30,000 in commission expense, before product and delivery costs. That makes early gross margin discipline critical, especially while marketing, support, and insurance are still fixed.
Expense classification
Put launch marketing, payroll before opening, training, and setup in pre-opening expenses. Reserve CAPEX for long-life assets only. That keeps the startup budget clean, avoids mixing operating spend with equipment cost, and makes the first months of burn easier to read when insurance, commissions, and payroll all start hitting at once.
This model starts at 5,700 Year 1 units, $1.779 million Year 1 revenue, and $26,500 monthly fixed overhead, so launch scale mainly changes equipment, staffing, and working cash.
Lean, Base, and Full launch paths with different cash needs.
Scenario
Lean LaunchLowest CAPEX
Base LaunchBalanced control
Full LaunchHighest control
Launch model
Outsource fabrication and keep the team small while you focus on provider onboarding.
Run a hybrid digital workflow with internal case management and selective production tools.
Build an in-house lab with deeper compliance systems and a larger service team.
Typical setup
Use lighter equipment, less in-house production, and more vendor capacity for overflow.
Keep core production in house, add provider onboarding, and hold moderate working capital.
Add more equipment, facility buildout, technicians, maintenance, and a bigger cash reserve.
Cost drivers
Outsourced fabrication
lower equipment spend
smaller team
vendor fees
lean working capital
Hybrid workflow
selective production tools
provider onboarding
moderate payroll
working capital
In-house lab buildout
compliance systems
more equipment
technicians
reserve cash
Planning rangeCAPEX only
$450k - $750kLowest cash need
$750k - $1.2MMiddle cash need
$1.4M - $2.0MLargest cash need
Best fit
Fits founders with limited cash and strong vendor access.
Fits operators who want control without a full lab buildout.
Fits founders with high volume confidence, strong operations experience, and a direct provider sales channel.
!
Planning note: Ranges are researched planning assumptions, not exact quotes or bids.
Mandibular Advancement Device Provider Business Plan
The researched model supports $178 million in Year 1 revenue across 5,700 units The largest line is 2,400 mandibular advancement devices at $450 each, or $108 million The premium adjustable splint adds 400 units at $750 each, or $300,000 Use this as a sales ramp target, not a guaranteed outcome
Plan enough working capital to cover the early ramp-up period, especially because fixed overhead starts at $26,500 per month before known payroll Known salaries total $460,000 per year for the chief executive officer, lead biomedical engineer, and two certified dental technicians If provider onboarding or collections lag, the business can burn cash even with orders in the pipeline
No, not every mandibular advancement device provider needs an in-house lab at launch Outsourcing can reduce equipment CAPEX and technician hiring, while an in-house lab gives more control over turnaround, quality, and capacity The tradeoff matters because the model assumes 5,700 total Year 1 units and includes $12,000 monthly facility rent plus $3,200 monthly maintenance
Model production choice first because it affects CAPEX, staffing, facility cost, quality systems, and gross margin A mandibular advancement device carries $50 in direct per-unit costs before revenue-based costs, while a premium adjustable splint carries $75 Add 40% of revenue for testing, utilities, sterilization, waste, and regulatory filing assumptions, then add 55% for commissions and card fees
Yes, budget for insurance early and validate coverage with a qualified broker The model includes general liability insurance at $1,800 per month, but a regulated dental device provider may also need product liability, cyber coverage, and professional coverage depending on its role If patient data flows through your systems, cyber and privacy controls become part of the cost plan
About the author
Matthew Clarke
Founder Support Writer
Matthew Clarke is a founder support writer at Financial Models Lab, where he helps non-finance readers understand practical profit planning and how small businesses make a profit. He focuses on clear, research-based guidance before money is invested, including startup cost estimates and early planning basics. His work makes business planning easier, more practical, and less intimidating.
Choosing a selection results in a full page refresh.