Radiofrequency Ablation Clinic Startup Costs: $134M+ CAPEX Plan
Radiofrequency Ablation Clinic
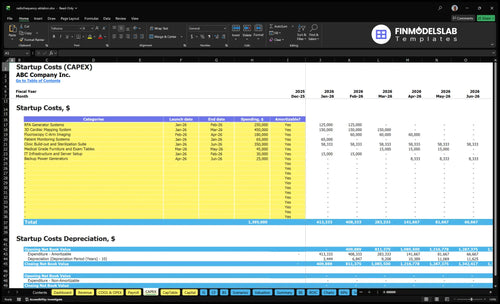
The cost to open a radiofrequency ablation clinic should be planned as at least $134M in identified equipment and buildout CAPEX before pre-opening expenses, working capital, financing costs, and owner draws The biggest modeled CAPEX items are the $450k 3D cardiac mapping system, $350k clinic build-out and sterilization suite, $250k RFA generator systems, and $180k fluoroscopy C-arm imaging In the first operating year, the model also carries $386k per month in fixed overhead and $622k per year in salaries, so reimbursement timing can move the total funding need fast Treat these figures as researched startup-budget assumptions, not guaranteed purchase prices or payer outcomes
Estimates capitalized startup assets only for a radiofrequency ablation clinic launch.
!
CAPEX only This calculator covers capitalized startup assets only. It excludes payroll runway, inventory, deposits, debt service, working capital, malpractice premiums, consumables, and reimbursement lag; add those in separate funding plans if needed.
How should a radiofrequency ablation clinic financial plan be built?
Build the Radiofrequency Ablation Clinic plan from the bottom up: estimate startup costs, time CAPEX, pre-opening spend, and working capital, then add reimbursement lag and staffing ramp so cash needs are visible. Model Year 1 capacity at 450% for cardiac electrophysiology, 500% for interventional pain, 400% for nurse practitioner services, and 500% each for registered nurse and radiology technician activity. Tie revenue to volume and price with 25 monthly cardiac treatments at $155k, 60 pain procedures at $32k, and lower-priced support visits, because lenders want cash runway not just profit.
Startup cash
Stage CAPEX by opening date.
Book pre-opening spend early.
Fund reimbursement lag.
Ramp staff with volume.
Revenue build
Model 25 cardiac treatments.
Model 60 pain procedures.
Add lower-priced support visits.
Show lender-ready runway.
What hidden costs come with starting a radiofrequency ablation clinic?
The biggest hidden costs in a Radiofrequency Ablation Clinic are the pre-opening items that don’t show up in buildout: payer enrollment, physician credentialing, state licensing, policies, malpractice deposits, billing setup, coding workflows, sterile supplies, launch marketing, and staff training. For the profit side, see How Increase Radiofrequency Ablation Clinic Profits? Monthly fixed expenses can already run $386k, including $185k rent, $98k malpractice insurance, $42k maintenance contracts, and $15k EHR and practice management software. If onboarding or payer setup runs long, cash burn rises before collections stabilize.
Hidden pre-opening costs
Payer enrollment delays cash flow
Credentialing can take weeks
State licensing adds upfront work
Policies and billing setup need cash
Working-capital drag
$28k utilities and medical waste
$600 office supplies
$12k accreditation fees
Training and malpractice hit before revenue
How much money do you need to start a radiofrequency ablation clinic?
A Radiofrequency Ablation Clinic should plan for more than $134M in startup funding, because identified CAPEX is only the base, not the full cash need. Add licensing, credentialing, insurance deposits, staffing, supplies, IT, billing setup, launch marketing, and cash runway; see How Increase Radiofrequency Ablation Clinic Profits? for the profit-side math.
This table covers the clinic's main startup equipment, build-out, and the separate opening cash reserve needed before launch.
Highlighted CAPEX$1,295,000Base planning example
Excluded cash needs$128,000Outside CAPEX total
Funding need$1,423,000CAPEX + excluded cash needs
Cost Category
Base Estimate
Main Cost Driver
CAPEX Calculator
3D Cardiac Mapping System
$450,000
Mapping hardware, installation, and setup
Yes
Clinic Build-out and Sterilization Suite
$350,000
Leasehold build-out, sterilization, and room prep
Yes
RFA Generator Systems
$250,000
Procedure generator units and commissioning
Yes
Fluoroscopy C-Arm Imaging
$180,000
Imaging system purchase and installation
Yes
Patient Monitoring Systems
$65,000
Monitoring equipment and bedside setup
Yes
Opening Cash Reserve
$128,000
Fixed overhead, Year 1 salaries, and reimbursement lag
No
Radiofrequency Ablation Clinic Core Five Startup Costs
Facility and Procedure-Room Buildout Startup Expense
Buildout Scope
The modeled buildout is $350k and runs from Month 1 to Month 6. It covers exam rooms, procedure rooms, recovery space, storage, accessibility, electrical work, infection-control flow, imaging accommodation, sterile processing, and safety items. Put this line early in the startup budget, because it happens before revenue starts.
Cost Drivers
Refine the estimate by square footage, number of procedure rooms, landlord allowance, and local contractor bids. A pain-focused clinic and a cardiac RFA clinic can need different room layouts, power, imaging, and sterile workflow, so one standard buildout does not fit every model. The key input is the scope you actually plan to open.
Cost Control
Use the landlord allowance first, then spend on the rooms and systems that affect safety and flow. Avoid overbuilding for cardiac capability if launch is pain-focused, but do not cut accessibility, sterile processing, or imaging accommodation. The cleanest savings come from right-sizing the shell before finish work starts.
Launch Timing
Because the model spreads this work across 6 months, the cash need is front-loaded long before collections. If permits or contractor work slip, opening slips too, so schedule buildout with procurement and staffing together.
RFA Equipment, Imaging, and Monitoring Startup Expense
Big Ticket Tech
RFA equipment is the largest technical CAPEX line. The model includes $250k for RFA generator systems, $450k for a 3D cardiac mapping system, $180k for fluoroscopy C-arm imaging, $65k for patient monitoring systems, and $45k for medical-grade furniture and exam tables.
What It Covers
This spend covers durable equipment, not disposable probes, cannulae, and catheters. Include installation, training, service agreements, and maintenance contracts in the cash plan. The model also carries $42k per month for equipment maintenance, so launch cash needs are not just the purchase price.
Keep disposables out of CAPEX
Budget install and training
Plan monthly maintenance cash
How to Size It
Use room count, cardiac versus pain procedures, imaging modality, and utilization ramp to size the package. A cardiac setup needs the 3D mapping system; a pain-only model may not. Get quotes by room and compare total cost, not just sticker price.
Control the Spend
Start with the minimum equipment set that matches first-year case mix. Ask vendors to break out hardware, installation, training, and service. That keeps you from overbuying imaging or monitoring capacity before utilization builds, and it makes it easier to see which line item is driving the budget.
Licensing, Insurance, Credentialing, and Compliance Startup Expense
Coverage and setup
This bucket covers state licensing, physician credentialing, payer enrollment, malpractice coverage, general liability, compliance consulting, legal formation, written policies, and accreditation where needed. In this model, monthly costs include $98k for medical malpractice insurance and $12k for professional accreditation fees, but requirements change by state, ownership, procedure mix, and payer strategy.
Cost inputs
Here’s the quick math: use quotes for each license, enrollment filing, policy, consulting hour, and accreditation cycle, then multiply by the number of states, physicians, and months of coverage. Credentialing delays matter because cash can go out before claims get paid, so this line belongs in startup runway, not just legal spend.
Count every licensed state.
Price each payer enrollment.
Budget months before reimbursement.
Keep it tight
Use one compliance lead and get written policies done early, then ask vendors for bundled quotes on insurance, consulting, and accreditation. Don’t skip malpractice or general liability to save cash; that just shifts the risk. The real savings come from avoiding rework when ownership rules, payer rules, or scope of practice change.
Bundle policy drafting.
Start payer work early.
Verify state rules first.
Cash timing
Plan for the gap between launch costs and first collections. If payer enrollment or credentialing slips, you still pay malpractice, consulting, and accreditation costs, so build extra runway before scheduling volume ramps.
Staffing Readiness and Launch Payroll Startup Expense
Payroll runway
Treat this as two costs: hiring setup and cash to carry payroll before collections start. The Year 1 staffing model is $622k a year, or about $51.8k a month, for 1 Medical Director, 1 Clinic Manager, 1 Patient Navigator, 2 Medical Assistants, and 1 Front Desk Coordinator. That burn belongs in launch cash, not just operating expense.
Headcount cost
Estimate it from headcount times annual pay. Here the named roles total $622k: $350k Medical Director, $95k Clinic Manager, $55k Patient Navigator, $84k for 2 Medical Assistants, and $38k Front Desk Coordinator. Use this to size recruiting, onboarding, and first payroll before patient revenue settles.
Cash gap
Don't mix recruiting with cash runway. Hiring fees, credentialing, and onboarding are one-time launch costs; payroll is a monthly burn. For Year 1, plan coverage for training, scheduling coverage, billing coordination, and the gap before collections stabilize. If you underfund this layer, payroll stress shows up before clinical volume does.
Clinical mix
Staff the service line around 1 cardiac electrophysiologist, 1 interventional pain physician, 1 nurse practitioner, 2 registered nurses, and 1 radiology technician. That mix supports both pain and cardiac RFA, but it also raises the need for cross-coverage, scheduling discipline, and enough working capital to carry the ramp.
Clinical Supplies, IT, Billing, and Launch Operations Startup Expense
Launch inventory
Opening day needs sterile packs, procedure supplies, medications, and disposables before the first case. Size it by case count, units per case, vendor quotes, and delivery timing. Keep initial inventory separate from recurring items like $15k/month EHR and practice management SaaS, $600/month admin supplies, and $28k/month utilities and medical waste.
Setup stack
Budget the launch stack for EHR, practice management setup, coding and billing workflows, phones, website, signage, referral outreach, and launch marketing. Estimate by user seats, setup fees, vendor onboarding, and launch-month spend. In the Year 1 model, billing runs at 50% and patient acquisition at 30%, so these costs should not be treated as one-time.
Control waste
Cut spend by matching orders to scheduled cases, not hope. The model assumes 120% for disposable RFA catheters and kits and 25% for medical gases and sterile supplies, so overbuying fast ties up cash. Use case-by-case par levels, track expiries, and avoid carrying more sterile stock than the next launch window needs.
Launch cash
What this estimate hides is timing. Software, utility, waste, and marketing bills start before collections, so the clinic needs cash for the gap between setup and steady volume. If credentialing or billing workflows slip, the first month of revenue can lag while $15k SaaS and $28k monthly operations continue.
Lean, Base, and Full-Scope RFA Clinic Startup Cost Scenario Table
Startup cost scenarios
The base case anchors to $1.395M of identified CAPEX, $386k monthly fixed costs, and $622k Year 1 salaries. Lean trims cardiac items; Full adds mapping, imaging, staffing, and more working capital.
Lean, Base, and Full launch bands for a radiofrequency ablation clinic.
Scenario
Lean LaunchLower cash need
Base LaunchCore clinic build
Full LaunchHighest complexity
Launch model
Focus on pain-management RFA first, and delay higher-acuity cardiac work until demand and licensing support it.
Run a standard outpatient RFA clinic with both pain and cardiac capability built into the first launch.
Launch with full cardiac capability, tighter compliance, and more staffing depth from day one.
Typical setup
Use core procedure rooms, a smaller team, and postpone 3D cardiac mapping and related complexity.
Fund the identified equipment stack, the Year 1 staffing plan, and normal build-out and launch cash.
Include 3D mapping, imaging, specialist coverage, added maintenance, and a larger cash buffer.
Cost drivers
Core RFA generator
smaller clinical team
lower compliance load
leaner working capital
Identified CAPEX
Year 1 salaries
monthly fixed costs
billing and marketing
working capital
3D mapping
imaging systems
specialist staffing
compliance and maintenance
extra working capital
Planning rangeCAPEX only
$950,000 - $1,200,000Lean band
$1,395,000 - $1,850,000Base band
$2,000,000 - $2,750,000Full band
Best fit
Best for founders who want a pain-first launch with lower reimbursement and staffing risk.
Best for operators who want the model's full base case and can carry the cash gap to Month 4.
Best for experienced founders with cardiac referrals, stronger payer mix, and more risk tolerance.
!
Planning note: These scenario ranges are researched planning assumptions from the model data, not exact vendor quotes or guaranteed prices.
The model identifies at least $134M in CAPEX before working capital and pre-opening costs The largest items are $450k for 3D cardiac mapping, $350k for buildout and sterilization, $250k for RFA generator systems, and $180k for C-arm imaging That number excludes debt service, owner draws, taxes, and any missing IT total not shown in the data
Runway should cover the early ramp-up period, especially if payer enrollment or claims timing runs long The model carries $386k in monthly fixed overhead and $622k in Year 1 salaries, or about $904k per month before variable clinical costs A three-month reserve on those two lines alone is about $271k, before supplies and billing costs
Not always, but the provided model treats major equipment as purchased CAPEX It includes $250k for RFA generator systems, $450k for 3D cardiac mapping, $180k for fluoroscopy imaging, and $65k for monitoring Leasing could reduce upfront cash but would add recurring payments, and that financing structure must be modeled separately
Budget cardiac capability as a higher-complexity scenario, not a small add-on The model includes a $450k 3D cardiac mapping system and assumes 1 cardiac electrophysiologist in Year 1 at 450% capacity Cardiac treatment capability can also raise staffing, facility, compliance, monitoring, maintenance, and working-capital needs
A lender budget should include CAPEX, pre-opening expenses, operating reserves, and exclusions Start with the $134M identified CAPEX, then add licensing, insurance, credentialing, launch payroll, supplies, billing setup, and reimbursement lag Also show monthly fixed overhead of $386k, Year 1 salaries of $622k, and variable costs equal to 225% of Year 1 revenue
About the author
George Lawson
Small Business Advisor
George Lawson is a small business advisor at Financial Models Lab who focuses on startup cost planning for local business owners preparing to launch. He studies common expenses, revenue drivers, and launch requirements to help turn a business idea into a basic, workable plan. George also writes about pricing and profitability basics in a practical, plain-spoken way, with a focus on helping readers make smarter decisions before they open their doors.
Choosing a selection results in a full page refresh.