Veterinary Hospital Startup Costs: $133K Monthly Readiness Before Launch
Veterinary Hospital
Key Takeaways
Facility buildout is CAPEX-heavy beyond the $25,000 lease anchor.
Equipment should match Year 1 specialty service mix.
Diagnostics setup should balance in-house and outsourced testing.
Pre-opening costs need clear CAPEX versus working-capital splits.
Estimate Startup Costs with Calculator
Startup CAPEX Calculator
Estimates capitalized startup assets only for a veterinary hospital, from buildout through equipment and furniture.
!
Excludes operating cash This calculator covers capital assets only. It excludes inventory, payroll runway, deposits, debt service, working capital, licenses, insurance premiums, and launch marketing. Contingency applies only to buildout, equipment, IT hardware, and furniture.
How does the Veterinary Hospital CAPEX forecast work?
What hidden costs do founders miss when opening a veterinary hospital?
Founders usually miss the non-equipment launch spend, so the trick is to separate operating costs from capital assets. If you’re also sizing owner pay, see How Much Does The Owner Of A Veterinary Hospital Typically Earn?; the hidden load is real, with $89,167 in monthly support payroll, plus $1,500 cleaning, $1,000 security, and $2,000 marketing. Year 1 medical COGS can also run at 140% from specialized pharmaceuticals, surgical implants, and disposables.
Launch costs
Recruiting and staff training
Pre-opening payroll before revenue starts
Insurance binders and software setup
DEA compliance, supplies, and deposits
Cash drain items
Initial medical supplies and pharmaceuticals
Food, cleaning supplies, and utility deposits
Security setup and cash reserves
Monthly support payroll at $89,167
How should a veterinary hospital funding plan be built?
Build the Veterinary Hospital funding plan in layers: first CAPEX, then pre-opening costs, then working capital and reserve months. Start with buildout, equipment, diagnostics, and IT hardware, then add licenses, insurance, inventory, payroll readiness, and deposits. Here’s the lender-ready anchor: the confirmed monthly burn floor is $133,167 before variable medical costs, and Year 1 should tie to about 200 effective treatments per month and $303,600 in monthly revenue under 500% to 600% service-line capacity assumptions.
Funding stack
CAPEX: buildout first
Add equipment and diagnostics
Include IT hardware and licenses
Fund insurance, inventory, deposits
Lender math
Use $133,167 monthly burn floor
Exclude variable medical costs
Model 200 effective treatments monthly
Map revenue to $303,600 monthly
How much does it cost to open a veterinary hospital?
Opening a Veterinary Hospital requires funding beyond buildout and equipment; the confirmed pre-opening readiness load is $133,167 per month before medical inventory, pharmaceuticals, debt service, or owner draws, which ties directly to What Is The Most Critical Metric To Measure The Success Of Your Veterinary Hospital?. Here’s the quick math: $44,000 fixed overhead plus $89,167 support payroll.
Known Monthly Need
$133,167 monthly readiness cost
$44,000 fixed overhead
$89,167 support payroll
Excludes inventory, drugs, debt, draws
Still To Quote
9 clinical specialists planned
5 service lines in Year 1
17 support FTE planned
Quote buildout, surgery, diagnostics, kennels, IT
Calculate Fuding Needs
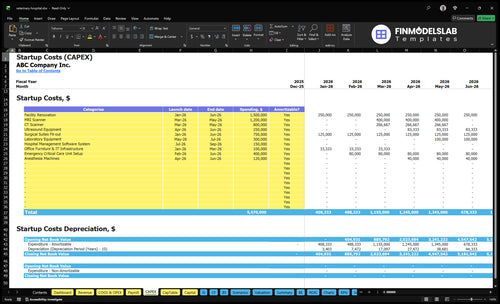
Startup cost summary
This table summarizes the main startup assets and the non-CAPEX cash reserve needed to open and bridge early losses.
Highlighted CAPEX$5,320,000Base planning example
Excluded cash needs$3,996,000Outside CAPEX total
Funding need$9,316,000CAPEX + excluded cash needs
Cost Category
Base Estimate
Main Cost Driver
CAPEX Calculator
Facility renovation and medical buildout
$1,500,000
Tenant improvements, clinical rooms, and core buildout work
Yes
Advanced imaging equipment package
$2,000,000
MRI and CT scanner spend
Yes
Surgical suites and anesthesia equipment
$870,000
Surgical fit-out plus anesthesia machines
Yes
Lab and emergency care setup
$700,000
Emergency critical care unit and laboratory equipment
Yes
Practice management software and IT infrastructure
$250,000
Hospital software system plus office IT infrastructure
Yes
Working capital reserve
$3,996,000
Lease, payroll, supplies, and early months before breakeven
No
Veterinary Hospital Core Five Startup Costs
Facility Buildout and Leasehold Improvements Startup Expense
Buildout Scope
This is mostly capital spending (CAPEX), not day-one operating spend, unless you separate a lease deposit or rent prepayment into working capital. The buildout covers exam rooms, treatment, surgery, recovery, kennels, plumbing, HVAC, medical flooring, radiology shielding if needed, reception, and workflow design.
Cost Inputs
Estimate it from shell condition, square footage, landlord allowance, surgery scope, emergency capability, and the imaging plan. The research data confirms a $25,000 monthly lease as the occupancy anchor, but it does not give construction or tenant improvement quotes, so the buildout budget still needs bids.
Use square feet and finish level.
Price HVAC, plumbing, shielding.
Separate deposit from buildout cash.
Spend Control
Keep scope tight around patient flow and safety first. Save money by phasing noncritical finishes, but do not cut corners on plumbing, HVAC, sterility, or shielding. The real savings come from controlling scope, because code, animal handling, and clinical workflow still drive the spec.
Finish the core rooms first.
Delay cosmetic upgrades.
Protect code and infection control.
Lease Anchor
The occupancy base starts at $25,000 per month, and buildout sits on top of that cash need. If the landlord allowance is small, tenant improvements hit startup cash harder; if it is large, you protect runway, but you still need enough funding to finish and open.
Medical, Surgical, and Treatment Equipment Startup Expense
What it covers
This CAPEX (capital expenditure) covers exam tables, anesthesia machines, surgical lights, monitors, an autoclave, a dental unit, oxygen setup, treatment tables, cages, recovery gear, and emergency support gear. Size it to the Year 1 mix of 2 surgical, 2 internal medicine, 1 imaging, 3 emergency critical care, and 1 anesthesiology specialist.
How to size it
Use unit counts, vendor quotes, and service needs to estimate this line. A surgery-heavy hospital needs more monitors, lights, and recovery bays; an imaging-heavy one may need different support gear. Don’t buy a full tertiary package on day one. Tie each item to the actual case mix and opening room count.
Control the spend
Cut cost by leasing gear that may change with case mix, financing larger items, and staging noncritical buys after opening. Protect anesthesia, oxygen, monitoring, and recovery capacity first. The safest savings come from bundling quotes and avoiding duplicate devices that sit idle between cases.
Owned, financed, leased
Separate this cost into owned assets, financed equipment, and leased equipment before you build the budget. That split changes upfront cash, monthly debt service, and replacement timing. It also keeps the startup plan honest, because the same hospital can open with a core owned set and add leased specialty gear later.
Diagnostics, Imaging, Lab, and Pharmacy Setup Startup Expense
Diagnostics Stack
Digital radiography, ultrasound if offered, in-house blood analyzers, microscopes, centrifuges, lab software integration, and pharmacy storage sit in this cost. Split the plan into owned, leased, and outsourced pieces so the startup budget matches the service mix. Start with equipment quotes and interface fees, not guesses.
Cost Base
Here’s the quick math: 36 effective imaging treatments a month at $800 each equals $28,800 in monthly imaging revenue. Lab testing and external diagnostics should be modeled at 30% of revenue until more tests move in-house. That makes this a mix of upfront CAPEX and ongoing variable spend.
Spend Control
Lease high-cost imaging gear when volume is still uncertain, and buy the core analyzers you’ll use every day. Keep outsourced tests as the bridge, then move only the high-frequency work in-house. More in-house testing raises CAPEX, but it can trim external diagnostic spend over time if case volume holds.
Pharmacy Controls
Pharmacy setup needs shelving, locked medication storage, and controlled-substance procedures that separate access, counts, and records. Treat this as a small build cost plus compliance work, not just fixtures. Keep opening stock tight and tie reorders to actual case flow, or expired meds and shrink will bite cash fast.
Technology, Systems, and Administrative Infrastructure Startup Expense
What It Covers
This cost covers the hospital’s digital and admin stack: practice management software, payment processing setup, computers, tablets, phones, networking, cameras, access control, website, booking tools, and cybersecurity. Treat hardware and install as upfront spend, then keep $2,500 per month for IT and software subscriptions plus $1,000 per month for security services.
How to Price It
Build the estimate from device counts, setup quotes, and months of coverage. Include cloud or server choice, booking tools, and integration work for lab results, medical records, billing, appointment scheduling, and client communications. One clean rule: if it touches daily flow, it belongs in the stack; if it renews monthly, it belongs in operating spend.
Price hardware separately.
Keep SaaS on monthly run-rate.
Get integration quotes upfront.
How to Trim It
Start with only the tools needed on day one, then add features after go-live. Standardize on one system, avoid duplicate apps, and keep camera and access control tied to the same security plan. The common mistake is mixing setup cost with monthly software, which makes launch cash look better than it is.
Buy once, then subscribe.
Skip duplicate software.
Use one login path.
Where It Connects
Integration is the real risk. If the system cannot move data cleanly between records, billing, scheduling, and client messages, staff will rekey work and slow care. That is why access control, cameras, and cybersecurity should be planned with the software stack from the start, not added later.
Licenses, Insurance, Staffing, Inventory, and Launch Readiness Startup Expense
Pre-Opening Cash
Treat state licensing, United States Drug Enforcement Administration (DEA) setup where needed, legal and professional fees, insurance binders, recruiting, training, and launch marketing as pre-opening expense. Treat first payroll, medical supplies, pharmaceuticals, food, cleaning supplies, and refill stock as working capital. The monthly cash anchors are $8,000 insurance, $89,167 support payroll, $2,000 marketing, and $1,500 cleaning, with Year 1 variable cost load at 190% of revenue.
Opening Stock
Opening stock should be priced separately from ongoing replenishment. Count day-one units of medical supplies, pharmaceuticals, food, and cleaning items, then multiply by supplier quotes. Add any controlled-substance handling tied to DEA procedures where applicable. That keeps the launch budget clear: one-time stock goes in setup cash, while restocking follows service volume and the 190% variable-cost load.
Trim the Spend
Keep the first buy tight. Order only the items needed to open safely, then restock from actual case mix and par levels, not guesswork. Use quotes from two or three vendors, push noncritical items to reorder later, and avoid overbuying pharmaceuticals with expiry risk. The savings come from smaller opening stock, not weaker care.
Opening Cash Buffer
Budget launch readiness as cash, not furniture. Licenses, recruiting, training, binders, and first payroll hit before revenue, so the real risk is underfunded opening month cash. If service ramp is slower than planned, the $89,167 support payroll and $8,000 insurance anchors stay fixed while inventory and marketing still need funding.
Compare 3 Startup Cost Scenarios
Scenario table
More service depth means more equipment, staff, and cash tied up before revenue catches up. Lean, base, and full show how much buildout changes startup cost and working capital pressure.
Lean, base, and full launch cost bands
Scenario
Lean LaunchLean build
Base LaunchCore plan
Full LaunchFull build
Launch model
Start with core specialty care and send high-cost imaging and lab work outside.
Open the researched five-line hospital with in-house core diagnostics and planned staffing.
Launch as a larger referral center with more imaging, emergency coverage, and in-house capacity.
Typical setup
Use a smaller leased site with fewer specialty services and limited in-house diagnostics.
Run 5 service lines with 9 clinical specialists, 17 support FTE, $44,000 monthly fixed overhead, and about 200 effective monthly treatments.
Add broader imaging, larger treatment capacity, more emergency coverage, and higher reserve months.
Cost drivers
Smaller lease
fewer specialists
outsourced imaging
outsourced lab work
lower payroll
5 service lines
9 clinical specialists
17 support FTE
$44,000 fixed overhead
$89,167 support payroll
MRI and CT buildout
emergency unit
larger payroll
higher reserve months
more treatment capacity
Planning rangeCAPEX only
Below base capexLower cash
$5.6M capexModel case
Above base capexHigh cash
Best fit
Best for founders testing demand before funding a full hospital build.
Best for operators who want the modeled balance of services, staff, and cash needs.
Best for well-capitalized teams that can carry heavy capex and longer cash draw.
!
Planning note: These scenario ranges are researched planning assumptions from the model, not vendor quotes or firm bids.
Plan working capital from monthly readiness costs, not just construction In this research set, fixed overhead is $44,000 per month and support payroll is about $89,167 per month, so each reserve month adds roughly $133,167 before medical supplies and debt service A three-month reserve would equal about $399,501 plus inventory and launch variance
Not always compare buying, leasing, and outsourcing by service line Surgery, anesthesia, treatment, imaging, and lab equipment should be split into owned assets, leased assets, and outsourced services The model already carries $2,500 per month for IT and software, but it does not include vendor quotes for medical equipment, so those quotes must be added separately
Budget leased space in three layers: monthly rent, deposits or prepaid rent, and buildout The source model includes a $25,000 monthly facility lease, plus $4,000 in base utilities and $8,000 in property and malpractice insurance Tenant improvements should stay in CAPEX, while deposits and reserve rent should sit in working capital
Fund payroll before revenue is stable because hiring starts before the hospital is fully productive The source plan includes 17 support FTE in Year 1 and about $89,167 in monthly support payroll It also plans 9 clinical specialists across surgery, internal medicine, imaging, emergency critical care, and anesthesiology, so recruiting timing matters
Yes, emergency services usually raise funding needs because they add staffing, monitoring, oxygen, treatment capacity, and reserve pressure In the Year 1 model, emergency critical care has 3 specialists, 50 monthly treatments per specialist, 600% capacity use, and a $1,500 treatment price That equals 90 effective treatments and $135,000 in monthly revenue capacity
About the author
Felix Ward
Entrepreneurship Researcher
Felix Ward is an entrepreneurship researcher at Financial Models Lab who focuses on expense and revenue planning for people opening a new small business. He turns practical business questions into clear planning steps, with a special focus on first-year business planning. Known for making business planning easier for non-finance readers, he writes in a calm, structured, and approachable way.
Choosing a selection results in a full page refresh.