 Owner income$0–$57k
Owner income$0–$57kHow Much Allergy And Immunology Clinic Owners Make: $57k Year 1 EBITDA

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$0–$57k  Net margin63%–500%
Net margin63%–500% Revenue for target pay$900k
Revenue for target pay$900k Business difficultyHard
Business difficultyHard


A US allergy and immunology clinic owner can plan around $0 to $57,000 of first-year distribution potential before personal taxes if the clinic protects cash These are researched assumptions, not guaranteed earnings The model reaches about $900,000 in first-year activity revenue, $667,000 EBITDA in Year 2, and $5993 million EBITDA by Year 5 as provider capacity scales If the owner also works as the paid physician, the model includes a separate $250,000 physician wage inside payroll
Owner income$0–$57kNet margin63%–500%Revenue for target pay$900kBusiness difficultyHardWant to test your allergy clinic owner pay?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, labor, overhead, reserves, and pay goals.
Planning note: This is a researched planning estimate only. Actual owner income depends on collections, payer mix, staffing, taxes, reserves, and cash needs. It is not guaranteed salary, tax advice, or owner distribution advice.
Want to check the full Allergy and Immunology Clinic forecast?
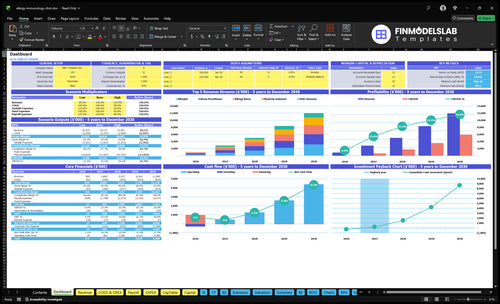
The Allergy and Immunology Clinic Financial Model Template shows the dashboard, assumptions, revenue build, staffing, expenses, cash flow, and owner pay in one view. It also tracks activity revenue, EBITDA, EBITDA margin, minimum cash, payback, and return metrics.
Owner-income model highlights
- Owner pay is shown clearly
- Revenue builds from $900k
- Scenarios test lean, base, high
How much does a private allergy practice owner make?
A private Allergy and Immunology Clinic owner’s income is not the same as clinic profit: this model already includes a $250,000 annual physician wage, and owner distributions depend on EBITDA, cash profit before interest, tax, depreciation, and amortization, after reserves and reinvestment; track demand with What Is The Current Growth Rate Of Patient Visits At Your Allergy And Immunology Clinic?. Model EBITDA is $57,000 in Year 1, $667,000 in Year 2, and $5.993M in Year 5.
Income split
- Separate wage from owner profit
- $250,000 physician salary is payroll
- Distributions come after reserves
- Treating owner may earn both
Cash limits
- EBITDA is not full take-home
- Debt can reduce distributions
- Payer timing can delay cash
- Growth hiring can absorb profit
How much revenue does an allergy clinic generate?
Revenue comes before profit and owner take-home for an Allergy and Immunology Clinic, so the first question is volume. Here’s the quick math: year 1 activity revenue is about $900k from 1 allergist, 1 nurse practitioner, and 1 allergy nurse; by year 5, with clinical roles up to 21, it reaches about $1.198M.
Year 1 revenue
- $350 to $390 physician visits
- $200 to $240 NP or PA visits
- $75 to $95 allergy nurse visits
- About $900k in year 1
Year 5 ramp
- 21 clinical roles by year 5
- About $1.198M revenue
- Utilization rises by role
- Revenue scales with capacity
Are allergy shots profitable for a clinic?
Yes—allergy shots can be profitable in an Allergy and Immunology Clinic, but only if reimbursement, vial cost, and nursing time stay tight. For the startup-cost angle, see How Much Does It Cost To Open An Allergy And Immunology Clinic?; one model puts allergy nurse revenue at $270k in Year 1 from 400 monthly treatments at $75 and 75% utilization. Still, the same model shows immunotherapy vials at 50% of revenue in Year 1 and medical supplies plus test kits at 40%, so payer rules and staffing waste can wipe out margin.
Why it works
- $270k Year 1 nurse revenue
- 400 monthly treatments
- $75 per treatment
- 75% utilization
What can break margin
- Vials can take 50% of revenue
- Supplies add 40% in Year 1
- Year 5 drops to 40% and 30%
- Payer rules can erase margin
Want to see the six income drivers?
1
$900K-$1.2MProvider Capacity
More referral flow and clinician slots lift visit volume, which is how the clinic moves from about $900K in Year 1 revenue toward about $1.2M by Year 5.
2
2%-3%Collections Rate
Cleaner claims and better payer terms keep more cash from each billed dollar, and the billing fee load sits around 3% early and 2% by Year 5.
3
7%-9%Service Mix
A smarter split between testing and immunotherapy changes the supply cost drag on revenue, so mix shifts margin fast.
4
$605KStaff Productivity
Higher output per provider and support staff spreads the $605K Year 1 payroll over more revenue and lifts take-home pay.
5
$174K/moOverhead Control
Fixed overhead runs about $174K a month, so even small savings in rent, insurance, EMR, and admin costs fall straight to EBITDA.
6
$57K-$5.99MOwner Leverage
If the owner keeps a patient schedule, the clinic can protect the $57K Year 1 EBITDA and build toward $5.99M by Year 5 while staying safer against the $705K minimum cash need.
Allergy and Immunology Clinic Core Six Income Drivers
Provider Capacity And Referral Flow
Provider Capacity and Referral Flow
New patient referrals fill the base schedule (open appointment slots) that feeds testing, follow-ups, allergy shots, and immunotherapy starts. Year 1 runs with 1 allergist, 1 nurse practitioner, and 1 allergy nurse; Year 5 expands to 5 allergists, 2 immunologists, 5 nurse practitioners, 4 physician assistants, and 5 allergy nurses. Empty slots turn payroll into margin drag, so this driver hits owner income fast.
Utilization (paid time filled with visits) rises from 65% to 85% for allergists and 75% to 95% for allergy nurses. Here’s the quick math: a 20-point gap means paid capacity sits unused. If referral flow slows, the clinic can look staffed for growth but still miss profit and owner draw because fixed payroll rises before revenue does.
Measure Fill Before Hiring
Track referrals, new patient conversion, show rate, and booked utilization by provider type. Add headcount only after the schedule stays full, because hiring ahead of referrals pushes fixed pay up before collections catch up.
- Count weekly referrals
- Watch open slots by provider
- Track no-shows and reschedules
- Delay hires until fill rate holds
1
Payer Mix And Collections
Payer Mix And Collections
Collected revenue is what pays the clinic, not billed charges. Model prices run $350 to $390 for physician services, $200 to $240 for nurse practitioner or physician assistant services, and $75 to $95 for allergy nurse services, so the service mix changes cash fast. A physician visit at $390 with a 30% billing fee leaves about $273 before rent, payroll, and supplies.
This driver includes payer mix, denials, prior authorization, and collection speed. Billing service fees run 30% of revenue in Year 1 and fall to 20% by Year 5, so the same schedule can throw off very different EBITDA. EBITDA means earnings before interest, taxes, depreciation, and amortization, and it depends on realized collections, not scheduled appointments.
Track Cash, Not Just Visits
Track gross charges, collected revenue, denial rate, prior authorization lag, and days in accounts receivable. If collections slip, owner pay slips too, even when volume looks fine. Keep a simple split by provider type so you can see whether $350 to $390 physician visits are funding overhead better than $200 to $240 NP or PA visits or $75 to $95 nurse services.
Push for cleaner claims, faster auths, and tighter follow-up on unpaid balances. The quick test is this: if billing costs still sit at 30% and denials rise, every dollar collected has less room left for payroll and owner draw. By Year 5, the billing fee target is 20%, so the clinic should keep improving clean-claim rates as scale grows.
2
Testing And Immunotherapy Service Mix
Service Mix Drives Recurring Margin
For an allergy and immunology clinic, service mix means how much revenue comes from testing, recurring allergy shots, and immunotherapy starts. Here’s the quick math: allergy nurse volume rises from 400 monthly treatments at 75% utilization in Year 1 to 480 monthly treatments at 95% utilization in Year 5, so repeat shots can fill the schedule and lift collected revenue.
Margins improve if direct costs fall with scale: immunotherapy vials drop from 50% of revenue in Year 1 to 40% in Year 5, and medical supplies plus test kits fall from 40% to 30%. The catch is simple: capacity, safety protocols, payer rules, and supply costs decide how much of that volume turns into owner take-home pay.
Track Volume, Cost, and Utilization
Measure treatments per month, nurse utilization, and cost per treatment by service line. Repeat allergy shots should raise schedule density, but only if each visit clears its own direct cost and does not slow testing or new starts. If utilization slips, idle nurse time and clinic time eat into margin fast.
Watch the mix between recurring shots and one-time tests. Keep supply orders tied to booked volume, not hope, so vials, kits, and disposables do not sit on the shelf. One clean rule helps: if a service cannot cover its direct cost and payer rules, it is hurting profit even when the calendar looks full.
3
Clinical Staffing Productivity
Clinical Staffing Productivity
Clinical staffing productivity is the gap between payroll and the patients each shift can carry. In Year 1, payroll is $605k across clinic manager, admin, medical assistant, physician, nurse practitioner or physician assistant, and allergy nurse roles, so empty slots quickly turn fixed labor into lost owner pay.
By Year 5, support staffing reaches 3 admin FTE, 5 medical assistant FTE, 7 physician FTE, 9 NP or PA FTE, and 5 allergy nurse FTE. If visit volume does not rise with that headcount, labor cost per encounter climbs and distributions shrink. One clean rule: more staff only helps if each schedule stays full.
Track output per FTE
Measure visits, treatments, and same-week fill rate by role, then compare that output to payroll each month. The key inputs are FTE count, booked slots, kept visits, and treatments per nurse or provider. That tells you whether labor is producing enough billable work to cover the fixed wage base.
Watch for small gaps across many providers. Even modest underbooking can spread over 16 to 29 FTE in Year 5, so the owner should tighten templates, cut low-yield blocks, and rebalance staffing before payroll outruns collections. The goal is simple: keep throughput ahead of headcount growth.
- Track visits per FTE monthly
- Compare payroll to collections
- Flag empty schedule blocks fast
- Match hires to booked demand
4
Operating Costs And Overhead Control
Fixed Overhead Floor
$174k in monthly fixed overhead sets the profit floor before owner distributions. At that run rate, annual fixed cost is $2.088M before billing fees or marketing. When visits dip, those bills still hit cash, so owner pay can shrink fast even if the schedule looks “mostly full.”
The key inputs are monthly visits, realized collections, and fixed spend. Separate fixed costs from cl inical costs: rent, utilities, malpractice, EMR, cleaning, office supplies, and waste disposal do not flex with volume, so the owner has to clear that base every month to protect take-home income.
Hold the Overhead Line
Track overhead as a share of collected revenue, not booked charges. Use a simple test: if collections fall, can the clinic still cover $174k plus billing fees and marketing? That answer tells you how much room there is for owner draws.
- Review fixed spend every month.
- Separate fixed and variable costs.
- Keep marketing tied to returns.
5
Owner Role And Provider Leverage
Owner Role and Provider Leverage
If the owner treats patients, manages the clinic, or hires more providers, the pay mix changes fast. In this model, a physician-owner can earn a separate $250k physician wage plus any profit draw, so take-home income is not just EBITDA. The leverage upside is real: modeled EBITDA rises from $57k in Year 1 to $5,993M in Year 5.
That growth only works if referral flow, collections, and staffing stay ahead of hiring. More providers add payroll, supervision, compliance, scheduling, and management load, so empty calendars turn into margin drag. One clean rule: hire for booked demand, not hope.
Track Capacity Before You Add Providers
Measure three inputs before expanding: referral volume, collections rate, and provider utilization. Also track the real cost of added roles, including salary, oversight time, and admin support. If a new clinician will not keep the schedule full, the extra wage lowers owner income instead of lifting it.
Use a simple test: add providers only when current staff are near target utilization and collections are stable. Watch the mix of physician salary versus profit draw, since a physician-owner may be paid twice, once as wage and once as distribution. If collections slow or staffing gaps widen, pause hiring before EBITDA gets diluted.
- Track booked visits by provider.
- Compare collections to scheduled volume.
- Watch payroll growth against utilization.
- Count supervision hours, not just heads.
6
Compare lean, base, and high allergy clinic owner income scenarios
Owner income scenarios
Owner income moves fast in this clinic because each added clinician lifts visit volume, but payroll, supplies, and billing fees rise too. Year 1 is lean, Year 3 is the scaled middle, and Year 5 is the mature case.
| Scenario | Low CaseLean launch | Base CaseScaled multi-provider | High CaseMature clinic |
|---|---|---|---|
| Launch model | This is the lean launch case with one allergist, one nurse practitioner, and one allergy nurse. | This is the modeled middle case with a larger provider mix and stronger throughput. | This is the stronger earnings case with a full clinic team and near-mature throughput. |
| Typical setup | Year 1 scale is about $900k in annual activity revenue and $57k EBITDA, with 3 clinical roles, 65% to 75% capacity use, and light billing and marketing overhead. | Year 3 scale is about $5.04M in annual activity revenue and $1.784M EBITDA, with 12 clinical roles, wider use of allergist, immunologist, NP/PA, and allergy nurse capacity, and steady fee-based costs. | Year 5 scale is about $12.0M in annual activity revenue and $5.993M EBITDA, with 21 clinical roles, higher capacity use, and more revenue from allergist, immunologist, NP/PA, and allergy nurse visits. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $0 - $57kLean launch | $1.78MScaled multi-provider | $5.99MMature clinic |
| Best fit | Use this to stress-test a slow opening, small patient panel, or delayed referral flow. | Use this as the middle case for a clinic that builds a steady referral base and fills schedules. | Use this to test upside if recruiting, scheduling, and patient demand all stay strong. |
Planning note: Scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or actual distributions.
Related Products
- Allergy and Immunology Clinic Porter's Five Forces Analysis
- Allergy and Immunology Clinic BCG Matrix
- Allergy and Immunology Clinic Business Model Canvas
- 7 Critical KPIs for Allergy and Immunology Clinic Success
- Allergy And Immunology Clinic Business Plan Template in Pre-Written Word
- 7 Strategies to Increase Allergy and Immunology Clinic Profitability
- How to Run an Allergy and Immunology Clinic: Key Monthly Costs
- Allergy and Immunology Clinic Startup Costs: $298K CAPEX to $10M
- Allergy and Immunology Clinic Financial Model Template in Excel
- How To Open An Allergy And Immunology Clinic In 4–9 Months
- How to Write an Allergy and Immunology Clinic Business Plan
- Allergy and Immunology Clinic Marketing Mix
- Allergy and Immunology Clinic Marketing Plan
- Allergy and Immunology Clinic Business Proposal
- Allergy and Immunology Clinic PESTEL Analysis
- Allergy and Immunology Clinic Pitch Deck Example Editable PPTX
- Allergy and Immunology Clinic Business SWOT Analysis
- Allergy and Immunology Clinic Value Proposition Canvas
Frequently Asked Questions
Plan around the modeled minimum cash need of $705,000, with the low point in Month 5 Startup capex totals $298,000, including $150,000 for build-out, $40,000 for immunotherapy lab equipment, and $30,000 for diagnostic equipment Cash reserves matter because EBITDA is not the same as spendable owner income