 Time to Open12 monthsLaunch runway
Time to Open12 monthsLaunch runwayHow To Start An Ambulance Service With a 6-Driver Launch Plan

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Time to Open12 monthsLaunch runway  Launch Sequence6 stagesLicense first
Launch Sequence6 stagesLicense first Key BottleneckLicense gateState rules
Key BottleneckLicense gateState rules First Revenue StepSigned contractDispatch ready
First Revenue StepSigned contractDispatch ready


You’re coordinating licensing, clinical oversight, vehicles, crews, dispatch, and contracts before the first call, not just buying an ambulance This guide covers the Month 1 to Month 60 launch path, with Year 1 planning built around 4 EMTs, 3 paramedics, 4 drivers, 2 dispatchers, and 1 supervisor Costs, funding, and profitability are validation checks here, not the main scope
Time to Open12 monthsLaunch runwayLaunch Sequence6 stagesLicense firstKey BottleneckLicense gateState rulesFirst Revenue StepSigned contractDispatch readyLaunch timeline
This is a short web summary of the launch sequence, and the XLSX export holds the detailed Gantt Chart.
Launch scheduleWeek 1Week 2Week 3Week 4Week 5Week 6Week 7
Licensing / compliance
- File EMS application
- Submit policy docs
- Complete inspections
- Secure operating permit
Medical director / protocols
- Appoint medical director
- Draft protocols
- Approve standing orders
- Set QA reviews
Vehicles / fleet
- Order ambulances
- Fit radio gear
- Mount stretcher systems
- Complete vehicle inspections
Equipment / supplies
- Order medical kits
- Stock consumables
- Calibrate monitors
- Pack response bags
Hiring / training
- Hire field crews
- Hire dispatchers
- Run ride-alongs
- Publish shift roster
Dispatch / billing
- Bind insurance coverage
- Sign service contracts
- Set dispatch software
- Open billing workflow
- Test soft launch
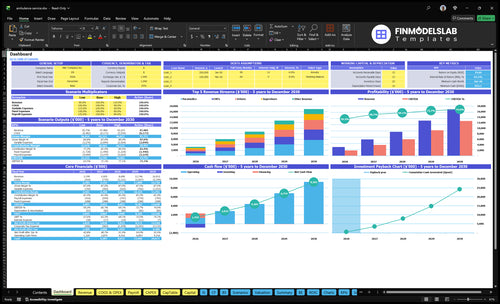
Why test an Ambulance Service launch before opening month?
The screenshot should show revenue, costs, cash needs, assumptions, and break-even logic; open the Ambulance Service Financial Model Template.
Financial model highlights
- $266.6k monthly billings
- 19% variable costs
- $24k fixed monthly
- Staffing and readiness tabs
Do you need a license to start an ambulance service?
Yes, an Ambulance Service needs licensing before launch; it’s a launch dependency, not cleanup work. In the US, rules vary across 50 states, so confirm agency approval, local authority, crew credentials, and insurance before buying vehicles or signing transport contracts; then track readiness with What Is The Most Critical Metric To Measure The Success Of Ambulance Service?.
License gates
- Get state EMS agency approval
- Secure local service area authorization
- Pass vehicle and equipment inspections
- Document required insurance before launch
Dispatch risks
- Approve medical direction and protocols
- Verify EMT and paramedic credentials
- Confirm 911 and facility contract rules
- Keep 100% of compliance files ready
How do you get clients for an ambulance service?
If you’re starting an Ambulance Service, get your first clients through signed agreements, not broad ads, and point prospects to How Much Does It Cost To Open And Launch Your Ambulance Service Business? for startup context. Focus on hospitals, nursing homes, rehabilitation centers, dialysis centers, event organizers, local government opportunities, and non-emergency medical transport referral sources. Revenue only works if your call volume matches what your staffed units can handle, and Year 1 capacity assumes 14 operating team members.
Target first
- Sign hospitals before ads
- Work nursing homes first
- Reach rehab centers directly
- Call dialysis centers early
Match ops
- Confirm service scope
- Set response coverage
- Map dispatch routing
- Lock billing and escalation rules
What ambulance service launch mistakes create the most risk?
Ambulance Service launch mistakes get expensive fast when you start taking calls before licensing, credentialing, dispatch, billing, and protocols are ready. With $24,000/month in visible fixed overhead before CEO salary and other payroll, one weak month can burn cash quickly, so don’t accept revenue until you have readiness gates, backup staffing, vehicle inspection proof, and signed first-revenue sources.
Top launch risks
- Underestimate licensing time
- Launch without credentialed EMT coverage
- Miss medical protocols
- Ignore billing setup
Controls that reduce risk
- Use readiness gates before calls
- Document dispatch-to-billing flow
- Keep backup staffing ready
- Keep insurance and call volume verified
Confirm what must be ready before accepting ambulance transport calls
Launch readiness checklist
Use this go-live approval checklist to confirm the ambulance service is ready before opening.
Compliance
- State EMS license approvedCritical
You can't run emergency transports without the state license.
- Service authorization on fileCritical
Service authorization clears you to take calls and bill.
- Medical director agreement signedHigh
A medical director anchors clinical oversight and protocols.
- Insurance policies boundCritical
Coverage needs to be active before the first unit rolls.
Fleet setup
- Ambulance registrations completeCritical
Registered units can be deployed and insured.
- Vehicle inspection passedCritical
An uninspected vehicle is a launch blocker.
- Stretcher and supplies stockedHigh
You need core equipment ready for each transport.
- Fuel and maintenance vendors setHigh
Fuel and repair delays can stop a unit fast.
Dispatch and billing
- Dispatch center setup completeCritical
Dispatch must route calls before launch.
- Dispatch software passed testingCritical
Calls, notes, and timestamps need to work cleanly.
- Billing claim flow worksCritical
Trips only turn into cash if billing runs.
- Radio and phone routing testedHigh
Crews need a reliable way to hear and answer calls.
Staffing
- EMT roster fully staffedCritical
You need enough EMTs to cover shifts and backups.
- Paramedic roster fully staffedCritical
Higher acuity calls need paramedic coverage.
- Driver shifts cover demandHigh
A unit is useless without a driver on shift.
- Backup supervisor shifts setHigh
Backup oversight keeps gaps from becoming service failures.
Referral pipeline
- Hospital referral contacts readyCritical
Hospitals are a core source of emergency and transfer calls.
- Nursin g home agreements signedHigh
These facilities drive recurring transport volume.
- Rehab, dialysis, and public leads readyHigh
These sources help fill non-emergency transport demand.
Financial control
- Utilization model matches staffingCritical
Trips per shift must fit the crew on hand.
- Variable costs stay near 19%High
Fuel, supplies, maintenance, and billing fees add up fast.
- Fixed overhead stays at $24kHigh
Rent, insurance, utilities, software, training, office, and marketing total $24,000.
- Cash runway covers slow claimsCritical
Claims lag can strain Month 1 cash.
- Breakeven path and signoffCritical
The model and final approval should both be clear before launch.
Want the six launch drivers that decide opening readiness?
1EMS License
License gateState EMS approval is the launch gate; without it, no compliant transport calls can start.
2Medical Director
Signed protocolsSigned medical oversight keeps protocols, meds, and review rules clear before the first call.
3Fleet Ready
19% loadOne compliant ambulance, stocked and inspected, keeps call acceptance live and cuts downtime.
4Shift Coverage
14 staffYear 1 needs 4 EMTs, 3 paramedics, 4 drivers, 2 dispatchers, and 1 supervisor to cover shifts.
5Dispatch Systems
$24K fixedDispatch, billing, and insurance must work on day one, or first claims and payments slip.
6First-Call Pipeline
60% useSigned facility and referral deals turn readiness into calls and reduce idle crew time.
EMS Licensing And Service Authorization
EMS Licensing and Service Authorization
Licensing is the gate. An ambulance can’t take compliant transport calls until the state EMS agency approves the service, any required local authority signs off, the vehicle passes inspection, and the service level is set. If marketing starts before permission is active, the launch can look open while operations are still blocked.
This driver includes the application, policies, medical director tie-in, insurance evidence, vehicle records, crew credentials, and completed approval tasks. The practical rule is simple: no approval, no legal dispatch. That affects opening date, day-one revenue, and whether crews can work without compliance gaps.
Pre-Launch Authorization Checklist
Sequence the work before you set an opening date. Verify the application is complete, the medical director tie-in is signed, insurance proof is ready, vehicle records match the unit, and crew credentials are current. If any of those are missing, the approval clock stalls and first-day transport capacity slips.
- Confirm state approval status.
- Check local authorization rules.
- Clear vehicle inspection first.
- Match service level to equipment.
- Block marketing until legal go-live.
Track this as a hard launch gate, not an admin task. The risk is simple: one missing document can turn a staffed ambulance into an idle asset. Keep a dated file for every approval step so you can prove readiness and move from paper authorization to real dispatch without delay.
1
Medical Director And Clinical Protocols
Medical Director and Protocols
If the medical director has not signed off, the ambulance service is not ready to open. This step sets the care rules: approved EMS clinical protocols, escalation rules, patient care report expectations, and controlled medication policies where applicable. Without that package, crews may not know what they can do on scene, and launch can slip even if the trucks and staff are ready.
This driver also sits upstream of licensing, staffing, and service scope. If you plan to run 4 EMTs, 3 paramedics, 4 drivers, 2 dispatchers, and 1 supervisor, they still need one clear playbook before the first dispatch. Weak protocol control creates charting gaps, inconsistent care, and avoidable compliance problems during early calls.
Lock the clinical playbook before go-live
Start with a written set of standing orders, crew procedures, documentation standards, and quality review steps. Have the medical director review each item against the actual service scope, so the launch plan matches what the crew can legally do on day one.
- Train staff on one protocol version.
- Test escalation rules before opening.
- Check chart fields and signatures.
- Assign a clear QA review owner.
Use sign-off sheets and mock patient care reports before the first call. If protocol training is late, opening can still stall because the service is not operational until crews can document, escalate, and treat the same way every time.
2
Ambulance Fleet And Equipment Readiness
Fleet And Equipment Readiness
This driver decides whether you can take the first call on time. For an ambulance service, the vehicle must match the service level offered, so a basic unit can’t cover an advanced setup gap. The real readiness signal is one compliant ambulance that is registered, equipped, inspected, maintained, fueled, stocked, and dispatch-ready.
If that unit is late, the launch slips even if staffing and contracts are ready. Missing stretchers, oxygen, meds, or inspection records can stop dispatch on day one and create compliance risk. One broken unit can also mean lost calls, slower response, and cash burn before revenue starts.
Pre-Open Unit Check
Use a pre-open checklist tied to the call level you plan to serve. Confirm stretcher setup, emergency equipment, medical supplies, a vehicle maintenance plan, a fuel process, and inspection records before launch. For budgeting, the source model sets supplies at 8% of modeled revenue, fuel at 5%, and maintenance at 4%.
Here’s the quick math: at $100,000 of modeled revenue, that means $8,000 for supplies, $5,000 for fuel, and $4,000 for maintenance. Build those costs into opening cash, and test that the unit can accept calls without preventable downtime. If the inspection log or stock list is weak, day-one service gets shaky fast.
3
Certified Staffing And Shift Coverage
Credentialed Shift Coverage
For an ambulance service, staffing is the gate that decides whether the truck can leave the bay and take calls on day one. If the roster does not match the planned service level, you get missed calls, coverage gaps, and launch delays even if the vehicles and licenses are ready.
Year 1 planning here assumes 4 EMTs, 3 paramedics, 4 drivers, 2 dispatchers, and 1 supervisor. The readiness check is simple: verified credentials, shift schedules, backup call-off coverage, and paramedic coverage where required. If any of those seats are empty, service capacity drops fast and burnout rises just as demand starts.
Build Coverage Before the First Dispatch
Before opening, verify every credential, set the weekly schedule, and test who fills in when someone calls off. That means checking EMT and paramedic licenses, assigning drivers and dispatchers, and making sure supervisor oversight is actually on the calendar, not just on paper. One open shift can block a full day of service.
Also line up training and onboarding before launch so the team knows call flow, hours of operation, and handoff rules. If staffing is thin at start, use backup coverage and tighter hours instead of pretending the roster is full. Credential checks, call-off coverage, and training completion are the three things that keep day-one operations legal and usable.
- Confirm all EMT and paramedic credentials.
- Map shifts to planned operating hours.
- Assign backup staff for call-offs.
- Test dispatch and supervisor coverage daily.
4
Dispatch, Billing, Insurance, And Admin Systems
Dispatch, Billing, and Admin Setup
For an ambulance service, this is the day-one cash and compliance system. If call intake, dispatch, patient care reports, and claims handoff are not working, you can answer a call but still miss the bill or trigger denials. With $1,500/month for software, $5,000/month for insurance premiums, and a 2% billing fee, this setup has to be live before the first transport.
This includes call intake, dispatch procedures, patient care report rules, insurance coverage checks, claims workflow, payment tracking, software access, and staff training. One broken step can delay revenue by weeks. The opening risk is not just admin work; it is slow cash, bad documentation, and weak first-day service.
- Set up dispatch and intake lines.
- Use one patient care report format.
- Assign billing handoff ownership.
- Track denials from day one.
- Confirm every user has access.
Test Calls and Claim Handoff
Run test calls before opening. Verify someone answers, dispatch logs the call, crews complete the patient care report, and billing receives the chart the same day. Build a simple rule: every transport closes with coverage captured, report signed, and claim queued. Here’s the quick math: at 2% billing fees, a $100,000 month costs $2,000 in billing fees.
Train on denial tracking and access control. Confirm payer edits are set, logins work, and one person owns exceptions. If documentation rules are loose for even the first week, you can open on time but still start with slow cash and avoidable denials. That creates early strain on working capital, even if the ambulances are ready.
5
Contracts And First-Call Pipeline
Contracts And First-Call Pipeline
For an ambulance operator, signed contracts are the difference between being ready and being idle. The real launch signal is signed or near-signed facility relationships with hospitals, nursing homes, rehabilitation centers, dialysis centers, event organizers, plus local government and referral sources where they matter.
This is the first revenue gate because the model starts with 60% utilization for EMTs, paramedics, and drivers, and 70% for dispatchers and supervisors. If those contracts slip, crews still need pay, vehicles still need fuel and upkeep, and the business opens with less call volume than planned.
Build The Call List Before Opening
Track every target by status: outreach made, meeting set, draft terms sent, credentialing checked, and contract near signature. Keep the dispatch-to-billing workflow ready too, because a first call only turns into cash if the paperwork, handoff, and claim steps are clean from day one.
Here’s the practical test: if the service can’t name its first few likely call sources and show how each one will flow to dispatch and billing, the opening plan is too thin. One clean one-liner: no pipeline, no ramp.
- Lock facility talks early
- Map payer enrollment needs
- Test call-to-claim steps
- Assign a contact owner
- Set weekly contract reviews
6
Related Products
- Ambulance Service Porter's Five Forces Analysis
- Ambulance Service BCG Matrix
- Ambulance Service Business Model Canvas
- 7 Critical KPIs to Track for Ambulance Service Growth
- Ambulance Service Business Plan Template in Pre-Written Word
- 7 Strategies to Increase Ambulance Service Profitability and Efficiency
- How Much Does It Cost To Run An Ambulance Service Each Month?
- Ambulance Service Startup Costs: $745K In Launch CAPEX
- Ambulance Service Financial Model Template in Excel
- How Much Does An Ambulance Service Owner Make? $150K Salary Plus Profit
- How to Write an Ambulance Service Business Plan in 7 Steps
- Ambulance Service Marketing Mix
- Ambulance Service Marketing Plan
- Ambulance Service Business Proposal
- Ambulance Service PESTEL Analysis
- Ambulance Service Pitch Deck Example Editable PPTX
- Ambulance Service Business SWOT Analysis
- Ambulance Service Value Proposition Canvas
Frequently Asked Questions
Start by confirming state EMS licensing rules, service area requirements, medical director needs, vehicle inspection standards, and staffing credentials Then build the operating plan around compliant units, dispatch, billing, insurance, and first contracts The provided Year 1 plan assumes 4 EMTs, 3 paramedics, 4 drivers, 2 dispatchers, and 1 supervisor