 Time to Open3-6 monthsLaunch runway
Time to Open3-6 monthsLaunch runwayHow To Start An Angiography Suite Design Firm In 3 To 6 Months

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Time to Open3-6 monthsLaunch runway  Launch Sequence5 stagesCredentials first
Launch Sequence5 stagesCredentials first Key BottleneckCoordination gateFacility quals
Key BottleneckCoordination gateFacility quals First Revenue StepPaid assessmentSite review fee
First Revenue StepPaid assessmentSite review fee


You’re launching a specialized healthcare construction firm, not a general contractor with a medical brochure This guide covers the 3 to 6 month sales-readiness path, the five-year model period, launch sequencing, bottlenecks, first revenue moves, and the practical next step: validate your pipeline before fixed overhead gets heavy
Time to Open3-6 monthsLaunch runwayLaunch Sequence5 stagesCredentials firstKey BottleneckCoordination gateFacility qualsFirst Revenue StepPaid assessmentSite review feeLaunch timeline
This is a short web summary of the launch plan, and the XLSX export includes the detailed Gantt Chart.
Launch scheduleMonth 1Month 2Month 3Month 4Month 5Month 6Month 7Month 8Month 9Month 10Month 11Month 12
Formation / compliance
- Form Entity
- Register Tax Accounts
- Confirm Licensing Scope
- Set Governance Records
Insurance / risk
- Submit Insurance Apps
- Request Bond Quotes
- Review Coverage Terms
- Issue Certificate Templates
Vendors / subs
- Build Vendor List
- Meet MEP Vendors
- Form Subcontractor Bench
- Review Equipment Quotes
Estimating / PM
- Set CRM
- Draft Templates
- Build Estimating Model
- Map PM Workflow
- Run QA Review
Marketing / sales
- Build Target List
- Start Outreach Calls
- Qualify Leads
- Send Feasibility Offers
- Issue Proposals
Staffing / ops
- Hire PM Team
- Add Site Fleet
- Onboard Core Staff
- Run Training
- Set Go-Live Checklist
Why test the revenue ramp before you hire?
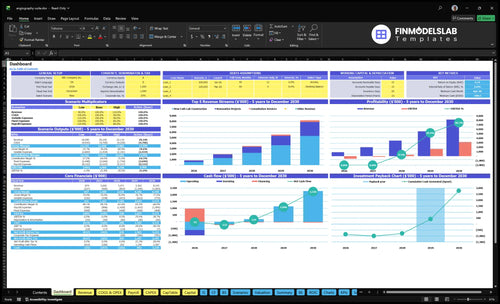
The Angiography Suite Design and Installation Financial Model Template shows revenue ramp, staffing, cash runway, break-even path, and project cash timing, so you can test Month 13 hiring. Open the model.
Financial model highlights
- 45% new construction
- 40% renovations
- 15% consultation services
- $262/hour weighted rate
- $31.4k monthly revenue
- 313% direct costs
- 687% contribution margin
- $34k fixed monthly
What are the biggest mistakes when starting an angiography suite installation business?
Starting an Angiography Suite Design and Installation business, the biggest mistake is bidding before the equipment vendor, electrical, HVAC, shielding, infection-control, and low-voltage teams are lined up. That’s risky because Year 1 subcontractor and material costs are modeled at 18% of revenue and equipment procurement at 8%, so a bad estimate can wipe out margin fast. The safer move is to sell feasibility first, then price the job after the scope is clear.
Biggest mistakes
- Bidding before vendor coordination
- Skipping compliance checks
- Using unvetted subcontractors
- Weak estimating controls
Safer approach
- Prequalify all key trades
- Map electrical and HVAC early
- Lock shielding and infection control
- Delay hires until demand is real
How to get first clients for an angiography suite design business?
The fastest first clients for an Angiography Suite Design and Installation business usually come from hospital facilities teams, cardiology groups, ambulatory surgery centers, imaging equipment vendors, architects, healthcare real estate developers, and referral partners. Start with paid site assessments, feasibility studies, and preconstruction proposals before full build contracts. For the model, $180,000 in Year 1 marketing and $45,000 CAC implies about 4 customers, so track every lead in CRM early; see How Much To Start Angiography Suite Design And Installation Business? for the setup side, and use consultation work at 15% of Year 1 mix at $225/hour as the easiest entry.
First target list
- Hospital facilities teams first
- Cardiology groups next
- Ambulatory surgery centers need help
- Referral partners widen reach
Low-friction offers
- Sell paid site assessments
- Lead with feasibility studies
- Pitch preconstruction proposals early
- Track every lead in CRM
What do you need to start an angiography suite design and installation business?
To start an Angiography Suite Design and Installation business, you need healthcare construction credibility, a formed company, applicable contractor licensing, insurance, bonding, vendor ties, and a qualified technical team before selling to hospitals; see How To Launch Angiography Suite Design And Installation Business? for the launch path. Budget professional liability at $8,500/month and project-specific insurance plus bonding at 18% of Year 1 revenue.
Required Setup
- Form the legal company
- Secure contractor licensing where required
- Carry general liability insurance
- Model professional liability at $8,500/month
Go-to-Market Musts
- Budget bonding at 18% of Year 1 revenue
- Build imaging equipment supplier relationships
- Coordinate early with MEP engineers
- Hire CEO, principal architect, senior project manager, MEP engineer, 0.5 business development manager, and admin assistant
Confirm what must be ready before approaching hospitals or cardiology groups
Launch readiness checklist
Use this go-live approval checklist to confirm the business is ready before opening.
Formation
- Entity formation completeCritical
The firm needs a legal base before contracts, permits, and banking move forward.
- Contractor licensing verifiedCritical
Verify contractor licensing for the launch scope and any local work rules.
- Tax and banking readyHigh
Clean banking and tax setup keeps deposits, payroll, and vendor payables moving.
Safety
- Insurance bound and activeCritical
Professional liability and general liability should be active before site work starts.
- Project bonding approvedHigh
Bonding matters for project access and should match the Year 1 revenue risk profile.
- Regulatory scope signed offCritical
Document healthcare safety, infection control, and radiation-related scope before launch.
Workflow
- Infection-control workflow documentedCritical
A clear infection-control path reduces rework and site delays during build and turnover.
- Imaging vendor coordination testedHigh
Coordination must cover power, layout, shielding, and equipment handoff timing.
- Project management platform liveHigh
Live project tracking keeps design, install, and punch list items from slipping.
Vendors
- Trade bench fully coveredCritical
Cover electrical, HVAC, shielding, low-voltage, flooring, infection-control, and finishes.
- Estimating templates approvedHigh
Standard templates keep bids consistent and help avoid missing trade inputs.
- Equipment procurement mappedHigh
Lead times for major equipment must fit the first project schedule.
Team
- Key roles staffedCritical
Staffing must cover design, project delivery, business development, and admin work.
- Clinical safety training completeHigh
Training should show healthcare safety and infection-control familiarity for the team.
- In itial payroll capacity checkedHigh
Payroll must fit early revenue timing, since Year 1 EBITDA is negative.
Finance
- Cash runway covers rampCritical
The model shows minimum cash of negative $310k in Month 28, so runway matters.
- Marketing budget allocatedHigh
Year 1 marketing budget is $180,000, so spend needs a clear pipeline target.
- First revenue pursuit readyCritical
The CRM pipeline should be active before proposals depend on missing vendor inputs.
Want to see the six launch drivers?
1Healthcare Construction Credibility
Trust gateRaises qualified lead conversion because hospitals trust proven medical design-build experience and clear safety procedures.
2Imaging Equipment Vendor Coordination
Scope-readyCuts rework by locking imaging supplier inputs, mechanical, electrical, and plumbing needs, and room handoffs before bid award.
3Healthcare Subcontractor Network
Trade benchSpeeds bids and lowers delivery risk by keeping healthcare-ready trades prequalified and available.
4Repeatable Preconstruction Workflow
6-stage flowShortens sales cycles by standardizing site checks, estimates, approvals, and handoffs.
5Qualified Sales Pipeline
3-6 moTurns a $180K budget and $45K CAC into paid assessments only if named leads stay active.
6Cash Runway Project Timing
Month 28Protects runway because $34K fixed costs and slow awards can outrun cash before payback.
Healthcare Construction Credibility
Healthcare Credibility
Hospitals and cardiology groups do not buy a general contractor; they buy proof that the team can handle medical facility risk. If the firm cannot show a principal with healthcare design-build experience, professional liability coverage, and relevant project examples, qualified leads will stall before award, and opening slips because there is no day-one work to execute.
This is the trust gate. The bottleneck is being seen as “just construction” instead of a specialist who can coordinate specialized trades, follow safety rules, and deliver a compliant cath lab on time. Without that proof, the company may still get calls, but it will struggle to convert them into paid preconstruction work or a first project.
Prove It Before You Bid
Before launch, document the principal’s healthcare project history, confirm contractor licensing where required, and secure insurance evidence that is ready to send with every proposal. Build short proposal language that names the firm’s cardiac and medical facility experience, plus a clear safety process for infection control, site access, and trade coordination.
Here’s the quick check: if the team cannot hand a hospital buyer a clean qualification packet in one email, it is not launch-ready. The packet should include project examples, coverage proof, licensing status, and a simple list of how the firm manages architects, equipment vendors, and specialty subs from day one.
- Attach project sheets first.
- Show insurance before pricing.
- State safety steps in writing.
- Map trade handoffs early.
What this hides is timing risk. Every month spent rebuilding trust can keep $34,000 in monthly fixed expenses and about $43,125 in initial payroll on the clock, so credibility has to be ready before the first serious bid goes out.
1
Imaging Equipment Vendor Coordination
Vendor Input Workflow
In an angiography suite, the room can’t be priced or built cleanly until the imaging supplier’s inputs are locked. Late equipment data pushes out scope, schedule, and bid accuracy, which can trigger change orders and slow opening. The pain shows up fast: a missed utility load or clearance can force redesign after award.
This driver covers original equipment manufacturer (OEM) equipment data, mechanical, electrical, and plumbing (MEP) requirements, radiation shielding, room readiness, and facility handoffs. If those pieces are not aligned before bid day, the team is guessing on the one thing hospitals care about most: whether the suite will be ready for safe use on day one.
Lock the bid assumptions early
Build one checklist for vendor outreach and do not release a proposal until you have equipment footprint, utility loads, shielding notes, and handoff timing. That keeps the preconstruction scope credible and cuts the chance of a post-award schedule conflict.
Assign one owner to chase the imaging supplier, shielding consultant, MEP engineer, and facility team. Keep one assumptions log for every bid, so the team can see what is confirmed, what is pending, and what could move the opening date.
- Confirm equipment dimensions first.
- Match loads to MEP design.
- Get shielding input before pricing.
- Track room readiness handoffs.
- Flag open assumptions in bids.
One clear rule: if the vendor data is still open, the schedule is still open.
2
Healthcare Subcontractor Network
Prequalified Subcontractor Bench
An angiography suite can’t open on time without a ready bench of electricians, HVAC, shielding, flooring, infection-control, low-voltage, and finish trades who already know healthcare site rules. This is the delivery capacity behind the first award. If you wait until award to source subs, you can win the job and still miss the start date.
The real dependency is trade capacity in the target market. Each quote needs a confirmed scope, availability check, insurance verification, and site-rule signoff. Weak execution here turns into pricing gaps, schedule slip, and rework before the first room is turned over.
Lock the Bench Before Bidding
Before opening, build a prequalified list and test it with real bid requests. Use quote templates, ask for current certificates of insurance, and confirm who can work in occupied healthcare spaces. That keeps the first proposal cycle fast and lowers the chance that a signed project sits idle while you scramble for labor.
With $34,000/month in fixed expenses before payroll, every delay burns cash. A simple readiness check helps: if a key trade cannot quote, mobilize, and follow site rules within your planned window, do not price the job as if they can.
- Verify trade coverage by market.
- Collect insurance before bid release.
- Confirm healthcare site rules.
- Track availability weekly.
- Keep quote templates standard.
3
Repeatable Preconstruction Workflow
Repeatable Preconstruction Workflow
This driver matters because early interest only becomes paid feasibility when the team can move from site assessment to scope, estimate, and schedule without rebuilding the plan each time. For an angiography suite, the preconstruction chain includes site assessment, scope definition, estimating, scheduling, submittals, vendor coordination, and closeout. If any step is ad hoc, launch slips and day-one delivery starts with missed assumptions.
Here’s the quick math: with $34,000 in monthly fixed expenses before payroll and about $43,125 in initial monthly payroll, custom proposals burn cash fast. A repeatable process shortens sales cycles and keeps estimate control tighter, so the business can get to paid feasibility work sooner instead of opening with a pipeline full of unpaid redesign.
Lock the Preconstruction Handoff
Before opening, build one intake path from sales into delivery. Use templates for site walks, scope sheets, assumptions, estimate backup, schedule notes, and closeout. Assign one owner for vendor and subcontractor input, then add approval gates at scope sign-off and before price release. Don’t send a proposal without written equipment and trade assumptions.
Because imaging equipment, shielding, and MEP details drive room readiness, late input can force rework and push first revenue back. Test the CRM handoff before the first lead comes in, and track how long each proposal stage takes. If the team cannot turn a lead into a buildable scope in a few clean steps, opening on time gets risky fast.
- Set one scope template.
- Require written vendor inputs.
- Use approval gates before bids.
- Track proposal cycle days.
- Hand off closed work in CRM.
4
Qualified Sales Pipeline
Qualified Sales Pipeline
Named leads are the gate to first revenue here. For cath lab work, the pipeline has to be built around hospitals, ambulatory surgery centers, cardiology practices, architects, healthcare developers, and imaging equipment channels. If the list is weak, paid assessments and proposals land late, and the launch can slip even if the team is ready.
Here’s the quick math: a $180,000 Year 1 marketing budget and $45,000 CAC support about 4 qualified wins ($180,000 ÷ $45,000 = 4). That means lead quality is a launch control, not a side task. Without a clean pipeline, you open with no booked work, and cash gets tight fast.
Target Accounts and Cadence
Build the launch plan around a target account list, clear CRM stages, a defined feasibility offer, and a fixed follow-up cadence. That lets you sort serious buyers from noise, time proposals better, and pull paid assessments forward before opening. The goal is simple: more paid assessments and better proposal timing.
- Separate accounts by buyer type.
- Track every lead in CRM.
- Set follow-up dates now.
- Skip broad construction marketing first.
5
Cash Runway And Project Timing
Cash Runway for Project Timing
This launch driver is about keeping cash alive while proposals, awards, and commissioning move slowly. A workable runway model maps retainers, progress payments, subcontractor deposits, staffing, and overhead to the month cash actually lands. Year 1 fixed expenses are $34,000/month before payroll, payroll is about $43,125/month, and marketing averages $15,000/month from a $180,000 annual budget, so pre-direct burn starts near $92,125/month.
Here’s the quick math: one active customer at 120 billable hours and about $262/hour produces about $31,440/month before direct and variable costs. That does not cover the stated overhead by itself, so a delayed award can force hiring cuts, slower vendor commits, or a launch slip. The big risk is paying people and trades before milestone cash is in.
Build the cash calendar before opening
Map each project phase to cash: proposal, retainer, design, equipment planning, construction, commissioning, and handoff. Put payment dates beside labor, deposit, and permit dates, then test the worst case if an award slips by 30 to 60 days. If the model breaks, delay hires and keep the team lean until the first contract is firm.
Verify who needs cash first: subcontractors, equipment suppliers, insurance, and payroll. Confirm the opening checklist covers lead times, inspections, and handoffs, because a late deposit or missing sign-off can stop work and push first revenue out. The model should show exactly which month the business can support one active customer and still pay overhead.
- Retainer dates and amounts
- Progress payment milestones
- Subcontractor deposit timing
- Payroll start month
- Inspection and handoff dates
6
Related Products
- Angiography Suite Design and Installation Porter's Five Forces Analysis
- Angiography Suite Design and Installation BCG Matrix
- Angiography Suite Design and Installation Business Model Canvas
- What Are The 5 KPIs For Angiography Suite Design And Installation Business?
- Angiography Suite Business Plan Template in Pre-Written Word
- How Increase Angiography Suite Design And Installation Profitability?
- What Are Operating Costs For Angiography Suite Design And Installation?
- Angiography Suite Startup Costs: $708K Before Contingency
- Angiography Suite Financial Model Template in Excel
- Angiography Suite Owner Income: $180K Salary To Year 5 Upside
- How To Write An Angiography Suite Design And Installation Business Plan?
- Angiography Suite Design and Installation Marketing Mix
- Angiography Suite Design and Installation Marketing Plan
- Angiography Suite Design and Installation Business Proposal
- Angiography Suite Design and Installation PESTEL Analysis
- Angiography Suite Design and Installation Pitch Deck Example Editable PPTX
- Angiography Suite Design and Installation Business SWOT Analysis
- Angiography Suite Design and Installation Value Proposition Canvas
Frequently Asked Questions
Yes, the model assumes a CEO and principal architect from Month 1, with a design architect added in Month 13 That does not replace contractor licensing checks where applicable It means the launch plan expects design authority, healthcare construction judgment, and proposal control before the firm sells angiography suite work