 Owner income$1.75M
Owner income$1.75MHow Much Aquatic Therapy Center Owners Make From $589K Revenue

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$1.75M  Net margin40.5%
Net margin40.5% Revenue for target pay$4.31M
Revenue for target pay$4.31M Business difficultyHard
Business difficultyHard


You’re trying to turn pool-based rehabilitation visits into real owner pay, not just top-line revenue This page covers aquatic therapy center revenue and expenses, including visit volume, collected rates, pool overhead, billing fees, reserves, and aquatic therapy business owner pay over a 60-month model period It does not give tax advice, guaranteed distributions, or clinic valuation
Owner income$1.75MNet margin40.5%Revenue for target pay$4.31MBusiness difficultyHardWant to test your owner pay assumptions?
Owner income calculator
Estimate owner take-home and target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: Research-based planning estimate only, not guaranteed salary, tax advice, or owner distribution advice.
Want the full forecast and owner income in one view?
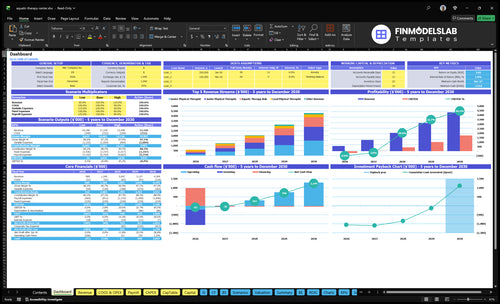
Open the Aquatic Therapy Center Financial Model Template to see dashboard outputs, revenue forecast, assumptions, staffing, pool costs, startup costs, debt, reserves, and owner pay in one place.
Owner income model highlights
- Year 1 revenue $589,320
- Year 5 revenue $4,309,440
- Fixed costs $19,700 monthly
- Stress tests utilization, reimbursement, payroll, reserves
What revenue is needed to pay an aquatic therapy center owner?
For an Aquatic Therapy Center, the bare minimum revenue before therapist payroll and owner pay is about $22,775 per month. Here’s the quick math: $19,700 in fixed overhead divided by a 86.5% pre-payroll contribution margin, because listed COGS plus variable costs equal 13.5% of revenue. To find the true owner-pay target, add therapist payroll, debt service, reserves, taxes, and the owner draw.
Revenue floor
- $19,700 fixed overhead
- 13.5% variable cost load
- 86.5% pre-payroll margin
- $22,775 monthly break-even
What to add next
- Therapist payroll
- Debt payments
- Cash reserves
- Taxes and owner draw
How does the owner role change aquatic therapy center income?
An owner-operated Aquatic Therapy Center usually shows stronger near-term cash because the owner can replace part of therapist payroll, but that cash is partly payment for clinical labor, not pure profit. In a manager-led setup, early take-home is lower because both management and therapist wages must be paid before any distributions. A multi-therapist model can grow from 3 clinical roles plus an aide in Year 1 to 16 staff roles by Year 5, but only if referrals, utilization, and pool capacity can carry the payroll risk.
Near-term cash
- Owner labor boosts early cash.
- Some income is wage replacement.
- Manager pay cuts early take-home.
- Distributions come after payroll.
Scale risk
- Year 1 can start lean.
- 3 clinical roles plus an aide is the base.
- Year 5 can reach 16 staff roles.
- Growth only works with strong utilization.
What affects aquatic therapy center profit margin most?
Utilization and revenue per visit move margin the most at an Aquatic Therapy Center, because pool overhead stays high even when visits dip. At 3,705 Year 1 monthly visits, a $10 change in collected revenue per visit shifts monthly revenue by about $3,705, or about $3,205 after the 13.5% COGS and variable cost load. A 5-point utilization lift across Year 1 roles adds about $3,970 a month before payroll, utilities, water heating, chemicals, maintenance, billing fees, and therapist coverage; see What Is The Estimated Cost To Open And Launch Your Aquatic Therapy Center? for the setup side.
Revenue per visit
- $10 more per visit = $3,705/month
- Net lift is about $3,205 after load
- Track collected revenue, not billed revenue
- Small pricing changes move margin fast
Utilization and overhead
- 5-point lift adds $3,970/month
- Pool costs do not fall quickly
- Watch payroll and therapist coverage
- Heating, chemicals, and billing bite hard
Want the six main income drivers?
1
371-2.6K/moVisit Volume
Utilization, or booked pool time used, turns more visits through the same space and lifts income fast.
2
$403K-$1.42MStaffing Structure
Wage load climbs as the team grows, so matching FTEs to demand is what protects take-home pay.
3
$133-$138Payer Mix
A better payer mix raises the cash kept per visit, so the same treatment hours produce more owner income.
4
80-200/moTherapist Output
More treatment slots per clinician increase revenue without adding staff at the same pace.
5
4.0%-3.2%Referral Retention
Stronger referrals keep the schedule full and push marketing spend down as a share of revenue.
6
3.5%-2.7%Pool Costs
Pool chemicals and equipment upkeep look small, but they still leak margin every month if the facility runs hot.
Aquatic Therapy Center Core Six Income Drivers
Visit Volume And Pool Utilization
Visit Volume and Pool Utilization
This driver is the number of billable aquatic therapy visits you actually fill, not the pool’s max schedule. Modeled monthly visits rise from 3,705 in Year 1 to 25,955 in Year 5 as utilization moves from 55% to 90%. More filled sessions spread fixed pool, rent, utilities, insurance, and admin costs across more reimbursed visits, which lifts gross margin and owner pay.
The ceiling is not demand alone; it’s licensed therapist capacity, documentation time, patient safety, and pool scheduling. Here’s the quick math: volume only helps if reimbursement per visit stays above the variable cost of serving it. If staffing or pool hours lag, cancellations, overtime, and rushed charting can wipe out the gain.
Fill the schedule, not just the pool
Track scheduled visits, completed visits, and utilization by role every week. Use the gap between booked and delivered sessions to spot weak referrals, late cancellations, or overbooked therapists. Dense scheduling matters more than raw capacity because a half-full pool still carries the same fixed overhead.
Set visit targets by staff mix and pool blocks, then test which roles can safely run near 90% utilization without adding documentation backlog. Watch the costs that scale with volume too: chemicals and water treatment are 20% of Year 1 revenue, and equipment maintenance is 15%. What this hides is simple: if each added visit does not cover its share of overhead, cash stays tight.
- Scheduled visits per week
- Completed visits per week
- No-show rate and cancellations
- Therapist hours by role
- Pool blocks and safety limits
1
Reimbursement And Payer Mix
Reimbursement and Payer Mix
Collected revenue per visit is the key lever here. In this model, it sits near $133 in Year 1 and $138 in Year 5, with role pricing ranging from $70 to $200. That means payer mix, clean claims, and any private-pay add-ons can move owner income fast. A $10 swing per visit changes monthly revenue by about $3,705 before payroll.
What this hides: reported revenue can look fine while cash lags from denials, underpayments, and late collections. The owner pays for that gap in slower cash flow and less room for draw. One clean rule: if collected revenue per visit slips, the business needs more volume just to hold the same take-home pay.
Track Net Collections Per Visit
Measure payer mix by visit, not just by patient count. Track gross charges, allowed amounts, denial rate, days in accounts receivable, and cash collected per visit. That tells you whether the center is really getting the $133 to $138 it models, or leaking margin through billing gaps.
- Split visits by payer type.
- Recheck low-paying plans monthly.
- Bill private-pay services cleanly.
- Fix denials within 7 days.
If the team can lift net collections by $10 per visit, the owner gets about $3.7k more monthly revenue before payroll. That is usually easier than adding a full new therapist schedule, so pricing discipline and fast collections should get reviewed every month.
2
Therapist Productivity And Labor Efficiency
Therapist Billable Capacity
Profit here comes from how many billable visits per therapist the team can safely handle against wages, benefits, aide support, and documentation time. In Year 1, the model uses 1 lead PT, 1 senior PT, 1 junior PT, and 1 aquatic therapy aide; by Year 5 it scales to 1 lead, 5 senior, 5 junior, 5 aides, and 2 wellness coaches, so staffing mix directly changes owner take-home.
Here’s the quick math: if staff can hold more paid visits without cutting care quality, labor cost per visit falls and gross margin rises. But unsafe ratios can boost short-term margin and still hurt retention, compliance, and patient outcomes, which can lower future revenue. The key inputs are visit load, documentation time, benefits, and aide coverage.
Measure Visits per Therapist
Track billable visits per therapist by role, plus unpaid admin time, so you can see where capacity is leaking. Use role-based targets instead of one blanket number, because a lead PT, senior PT, junior PT, and aide do not carry the same load. That keeps payroll tied to revenue, not wishful scheduling.
- Billable visits per paid hour
- Documentation minutes per visit
- Visits per aide-supported hour
- Payroll plus benefits per visit
- Safety incidents and rework
Watch for the trap: if you push staffing leaner than the care model can support, margin may look better for a month, but clinical risk and turnover can erase it. The better move is to staff so each therapist stays productive, the pool schedule stays dense, and owner profit comes from sustainable throughput, not overtime or burnout.
3
Pool Facility And Operating Costs
Pool Cost Load
This driver is the full pool facility bill: lease or mortgage, utilities, liability insurance, maintenance, software, licensure, supplies, plus pool chemicals and water treatment. Fixed monthly overhead is $19,700 ($12,000 lease, $3,500 utilities, $1,500 insurance, $1,000 maintenance, $800 software, $500 licensure, $400 supplies).
In Year 1, chemicals and water treatment add 20% of revenue, and equipment maintenance adds another 15%. So every $10,000 of monthly revenue leaves about $6,500 before therapist pay and marketing. Downtime, heating spikes, repairs, and access rules can shrink owner take-home even when visits stay booked.
Track Cost per Visit
Track pool cost as a percent of revenue and per completed visit. If chemicals stay near 20% and maintenance near 15%, price and utilization have to cover the rest. One clean test: compare cost per visit before and after schedule changes, then raise prices if higher heating or access hours lift the bill.
- Monthly visits and open hours
- Heating and utility bills
- Chemicals and repairs
- Downtime and access limits
Build a repair log, a heating log, and a downtime log. If the pool closes, fixed overhead still runs at $19,700 a month, so lost hours hit twice: less revenue and the same lease, utilities, and insurance. Keep distributions last, after the monthly reserve for chemicals, repairs, and replacement parts.
4
Staffing Struc ture And Owner Role
Owner Labor vs Profit
An owner who treats patients can cut paid therapist payroll, but that cash is labor pay, not pure profit. In Year 1, staffing is small: one lead PT, one senior PT, one junior PT, and one aquatic therapy aide. In Year 5, the model expands to one lead, five senior, five junior, five aides, and two wellness coaches, so the center needs enough visits to cover both clinical wages and management pay.
Here’s the key split: owner clinical hours improve cash flow, but only the remaining profit is an ownership draw. If you mix the two, you overstate passive income. A manager-led center is less owner-dependent, but it still needs dense scheduling to pay for the full wage stack.
Separate Pay From Draw
Track owner hours, billable visits, and clinical payroll separately. That lets you see whether the owner is replacing staff labor or earning true profit. A clean model should show the owner’s treatment pay as expense, then the leftover cash as distribution.
- Log owner visits and collections.
- Split clinical pay from profit draw.
- Test if visits cover management wages.
If the owner stops treating patients, payroll rises fast unless volume is high enough to absorb it. If the owner does treat patients, the business may look healthier on paper, but only because labor moved from payroll into owner compensation.
5
Referrals And Patient Retention
Referral Flow And Repeat Care
When orthopedic, post-surgical, senior care, sports medicine, and chronic pain referrals stay steady, visit volume is easier to forecast and therapist schedules stay full. That matters because marketing and patient acquisition are modeled at 40% of revenue in Year 1, then 32% by Year 5, so every extra referred visit lowers the share of revenue needed to win new patients.
Weak referrals do the opposite. If repeat care plans do not hold patients, the center still carries fixed pool costs, rent, utilities, insurance, and admin costs, but with fewer reimbursed visits to cover them. One clean metric is referral-to-start rate: if referrals rise but starts do not, owner income usually leaks through wasted marketing spend and idle therapist time.
Track Source Mix And Rebook Rate
Watch where patients come from, how many start treatment, and how many finish a plan and rebook. A simple scorecard should include new referrals by source, start rate, visit completion rate, and 30-day return rate. If one channel dries up, the center needs more paid marketing, which pushes down profit and owner draw.
Here’s the quick math: more retained patients mean more billed visits with the same pool and staff base. That improves cash flow because recurring care fills open slots without fresh ad spend. The owner should ask one question every week: are referrals becoming kept visits, or just inquiries? If the answer is no, margin will stay under pressure.
- Track referrals by source.
- Measure starts per referral.
- Measure rebook rate after visits.
- Cut gaps in care plans.
- Watch marketing as revenue share.
6
Compare low, base, and high owner income scenarios
Owner income scenarios
Income moves with visit volume, revenue per visit, and staffing depth. The Year 1, Year 3, and Year 5 cases show how a pool rehab center shifts from thin surplus to strong owner take-home.
| Scenario | Low CaseLow case | Base CaseBase case | High CaseHigh case |
|---|---|---|---|
| Launch model | Year 1 stays lean at 371 monthly visits, $133 revenue per visit, and $589,320 annual revenue. | Year 3 moves to 1,291 monthly visits, $132 revenue per visit, and $2,046,600 annual revenue. | Year 5 reaches 2,596 monthly visits, $138 revenue per visit, and $4,309,440 annual revenue. |
| Typical setup | This case assumes a small opening team, heavier fixed costs, and a $272,862 pre-payroll surplus before debt, reserves, and taxes. | This case assumes a fuller therapist roster, stronger visit density, and a $1,545,514 pre-payroll surplus before owner pay, debt, reserves, and taxes. | This case assumes a mature schedule, deeper staffing, and a $3,594,692 pre-payroll surplus before owner pay, debt, reserves, and taxes. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $272,862 pre-payroll surplusLean surplus | $1,545,514 pre-payroll surplusMid-case surplus | $3,594,692 pre-payroll surplusPeak surplus |
| Best fit | Use this to stress-test a cautious opening with slower utilization. | Use this as the mid-case planning view for budgeting and staffing. | Use this to test the upside if utilization stays high and staffing keeps up. |
Planning note: Scenario figures are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Aquatic Therapy Center Porter's Five Forces Analysis
- Aquatic Therapy Center BCG Matrix
- Aquatic Therapy Center Business Model Canvas
- 7 Core Financial KPIs for Your Aquatic Therapy Center
- Aquatic Therapy Center Business Plan Template in Pre-Written Word
- How to Boost Aquatic Therapy Center Profit Margins
- How Much Does It Cost To Run An Aquatic Therapy Center Monthly?
- Aquatic Therapy Center Startup Costs: Plan For $750K+ In CAPEX
- Aquatic Therapy Center Financial Model Template in Excel
- Start an Aquatic Therapy Center: 6–12 Month Launch Plan
- How to Write an Aquatic Therapy Center Business Plan in 7 Steps
- Aquatic Therapy Center Marketing Mix
- Aquatic Therapy Center Marketing Plan
- Aquatic Therapy Center Business Proposal
- Aquatic Therapy Center PESTEL Analysis
- Aquatic Therapy Center Pitch Deck Example Editable PPTX
- Aquatic Therapy Center Business SWOT Analysis
- Aquatic Therapy Center Value Proposition Canvas
Frequently Asked Questions
Owner income depends on what remains after payroll, debt, reserves, and taxes The researched model shows $589,320 in Year 1 revenue and $272,862 before clinical payroll and owner pay By Year 5, revenue reaches $4,309,440 with $3,594,692 before those same deductions