 Owner incomeNot calculable
Owner incomeNot calculableHow Much Autism Support Service Owners Make On $143M Year 1 Revenue

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner incomeNot calculable  Net margin48%–79%
Net margin48%–79% Revenue for target pay$118.8k–$1.02M
Revenue for target pay$118.8k–$1.02M Business difficultyHard
Business difficultyHard


You’re planning owner pay before the service has a clean payroll model, so separate revenue from cash you can actually take home The provided assumptions produce $143M in Year 1 revenue and $1228M by Year 5, but owner take-home is a planning estimate before personal taxes and varies by payer contracts, state rules, staffing, service mix, reserves, and debt service
Owner incomeNot calculableNet margin48%–79%Revenue for target pay$118.8k–$1.02MBusiness difficultyHardWant to test your owner pay number?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: Research-based planning estimate only. It is not guaranteed salary, tax advice, or owner distribution advice. It excludes personal benefits, acquisition debt, grants, and state-specific reimbursement rules.
How do you stress-test owner pay in the Autism Support Service model?
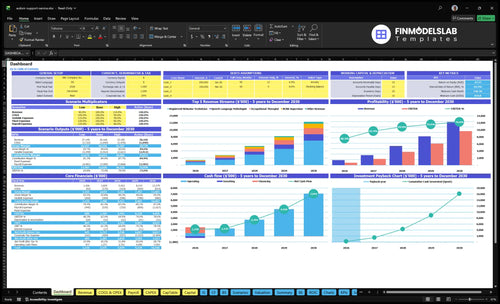
The dashboard shows revenue, margin, costs, reserves, and owner take-home assumptions; open the Autism Support Service Financial Model Template to check it.
Owner-pay model highlights
- Owner income outputs
- Revenue and staffing tabs
- Scenario tables by driver
What revenue is needed to pay an autism support service owner?
Revenue need isn’t a single number for an Autism Support Service owner; it depends on active clients, authorized hours, collected rates, utilization, and therapist capacity. In the model, monthly revenue is $118,820 in Year 1 from 20 listed clinical staff, and $1,023,240 in Year 5 from 108 listed clinical staff, so owner pay has to fit after payroll and reserves. A $65 Registered Behavior Technician treatment and a $200 to $240 psychology treatment do not have the same margin math.
Revenue drivers
- Active clients set volume.
- Authorized hours cap billable time.
- Collected rates drive cash.
- Utilization changes realized output.
Pay planning
- Pay comes after payroll.
- Keep reserves for slow collections.
- Model $65 vs $200 to $240 services.
- Use staff capacity to test scenarios.
How much can an autism support service owner pay themselves?
An Autism Support Service owner can pay themselves only from durable cash left after clinician payroll, admin wages, fixed overhead, variable costs, reserves, and reinvestment; see What Does It Cost To Run Autism Support Service? for the cost stack. The source model shows $143M Year 1 revenue and $5,109k pre-clinician-payroll surplus, but direct clinician wages are not provided, so that surplus is not owner salary.
Pay order
- Pay clinicians first
- Cover admin wages
- Fund fixed overhead
- Hold cash reserves
Owner test
- Model owner pay as an expense
- Exclude unpaid clinician payroll
- Check cash, not billed revenue
- Reinvest before taking distributions
What affects autism support service profit margin the most?
Collected payer rates, utilization, and direct clinician payroll move Autism Support Service margin the most. For a quick KPI lens, see What Are The Five Core KPIs For Autism Support Service Business? Small shifts matter here because Year 1 role utilization ranges from 50% to 75%, while variable costs start at 205% of revenue and fall to 130% by Year 5.
Biggest margin levers
- Collected payer rates change cash margin fast
- Utilization swings billed hours per clinician
- Direct clinician payroll is the swing factor
- Cancellations cut paid session volume
Cost pressure points
- Fixed overhead stays at $19,800/month
- Admin wages rise from $385k to $790k
- Supervision load raises labor cost
- Billing cost and overhead add drag
Want the six main income drivers?
1
$65-$240Payer Rates
The same visit can bill from $65 to $240, so rate cards and clean collections move take-home fast.
2
$1.4M-$12.3MClient Census
More active clients and authorized hours push revenue from $1.4M in Year 1 to $12.3M in Year 5.
3
50%-90%Utilization Spread
When clinician use rises from 50% to 90%, more billed time lands on the same payroll base.
4
5 linesService Mix
A wider mix of behavior analyst supervision, technician visits, speech therapy, occupational therapy, and psychology adds oversight, so higher-pay work has to carry the lower-pay work.
5
$19.8K/moOverhead Load
Fixed overhead runs about $19.8K a month, so any slack in rooms, systems, or licensing cuts straight into cash.
6
$385K-$790KOwner Capacity
If the owner stays in delivery and admin, payroll scales from about $385K to $790K, so delegation is what protects margin.
Autism Support Service Core Six Income Drivers
Payer Rates And Collections
Payer Rates And Collections
This driver is the cash you actually collect per treatment, not the billed rate. For this kind of autism support center, collected reimbursement sets the top line before rent, payroll, and admin get paid, and rates can range from $65 for Registered Behavior Technician treatments to $240 for clinical psychologist treatments by Year 5.
Here’s the quick math: sessions × collected rate = revenue. Watch average collected rate, denial rate, payment lag, authorization limits, and private-pay share. Lower collections cut owner pay dollar-for-dollar after fixed costs, so delays and denials hit cash flow fast. Stronger collections improve timing and the owner’s ability to take profit out.
Track Collections, Not Just Charges
Measure what gets approved, what gets paid, and how long it takes. Compare billed versus collected dollars each month, then break out denials, aged claims, and unpaid authorized sessions. If a payer is slow or underpriced, the issue shows up in cash before it shows up in revenue, so use those numbers to push contract fixes and faster follow-up.
Protect owner income by tightening intake checks and claim cleanup. Confirm benefits and authorization limits before care starts, then rework denials fast. A small lift in collection rate matters more than a small lift in charges, because fixed overhead stays in place and every extra collected dollar can flow to profit or owner draw.
1
Active Clients And Authorized Service Hours
Active Clients And Authorized Service Hours
This driver is the number of active clients and the approved or purchased hours tied to each care plan. When those hours stay full, clinicians keep billing. When authorizations run late or families miss slots, weekly billable hours drop, revenue falls, and fixed payroll and rent still hit the owner’s draw.
The capacity benchmark here is 40 to 45 monthly Board Certified Behavior Analyst supervisor treatments, 120 to 130 Registered Behavior Technician treatments, and 100 to 110 speech or occupational therapy treatments per provider. Stable census protects utilization; weak intake conversion, cancellations, or early discharge can leave paid staff underbooked.
Track authorization flow, not just headcount
Measure active clients, weekly billable hours, cancellations, intake conversion, and discharge timing. Here’s the quick math: if authorizations do not cover the provider’s monthly treatment load, booked hours shrink fast and gross margin gets thinner because payroll stays fixed while sessions disappear.
Use a simple control sheet by therapist and payer. Flag late authorizations, waitlist leakage, and family schedule gaps before they cut census. One clean rule: no open slot should sit unfilled for more than one week without a follow-up.
- Check hours approved versus billed.
- Review cancellations by family and payer.
- Track intake-to-first-visit conversion.
- Watch discharge dates against plan.
2
Clinician Utilization And Wage Spread
Clinician Utilization Spread
Owner income here comes from the gap between collected billable revenue and clinician payroll. Utilization usually runs from 50% to 90% across roles, so the same paid hour can produce very different margin. An RBT at 70% utilization in Year 1 creates less revenue capacity than at 85% later; that is about 21% more billable output for the same paid time.
Here’s the quick math: higher billable productivity lifts gross margin, but non-billable paid time, supervision hours, training, turnover, and benefits all eat into the wage spread. If scheduling pushes utilization too high, retention and care quality can slip, and that can hurt cash flow more than a small margin gain helps it. Ethical scheduling lifts margin without burning out staff.
Track Utilization by Role
Measure billable hours, paid non-billable time, and collected revenue per clinician by role each week. Split out supervision and training so you can see the real wage spread, not just headcount. If an RBT is stuck near 70%, find the blocker: authorization lag, cancellations, or too much admin time.
Set a target band, not a max squeeze. Compare utilization at 70%, 80%, and 85% to see where margin improves without raising turnover. If the schedule gets tighter, watch discharge timing, no-show rates, and staff exit risk. That is where owner pay gets protected or lost.
3
Service Mix And Supervision Intensity
Service Mix Drives Margin
This driver is the service mix: how many sessions are Registered Behavior Technician at $65, speech-language pathology at $130, occupational therapy at $130, Board Certified Behavior Analyst supervision at $150, and clinical psychology at $200. The mix sets revenue per booked hour, but it also sets payroll pressure because higher-rate services often need scarcer staff and more supervision.
If the mix leans too hard toward lower-rate care, gross margin per hour drops and there is less left after fixed costs. If it leans too hard toward high-rate services, supervisor time, session length, and documentation can become the bottleneck, which slows cash flow and cuts the amount available for owner pay.
Track Revenue By Service Line
Measure each service line on its own. Track rate per treatment, supervision ratio, session length, and documentation time each month so you can see which sessions add profit and which only add workload.
- Compare revenue per staffed hour.
- Watch supervisor hours per session.
- Shift slots before adding headcount.
A balanced schedule usually protects owner income best: enough higher-rate work to lift revenue, but not so much that scarce staff drive overtime, delays, or missed authorizations. If documentation starts crowding treatment time, the margin you expected can disappear fast.
4
Overhead, Compliance, And Admin Costs
Overhead, Compliance, and Admin Cost Load
Fixed overhead cuts cash before owner pay. Here, it totals $19,800/month or $237,600/year, including $12,000 rent, $2,500 utilities and maintenance, $1,200 Health Insurance Portability and Accountability Act (HIPAA) compliant IT and security, $1,800 liability insurance, $800 supplies, and $1,500 licensing fees. Admin payroll rises from $385k to $790k a year, so the center must carry enough billable hours to cover the base.
The key inputs are rent, admin headcount, compliance spend, and the split between fixed costs and variable delivery costs. When utilization dips, these center costs stay put, so break-even pressure rises fast and owner draw shrinks. Lean admin improves resilience.
Track Fixed Cost Per Billable Hour
Measure monthly overhead against billable hours, active clients, and collected revenue. Here’s the quick math: $19,800 in fixed overhead never goes away, so every drop in utilization pushes more of that load onto each session. Keep admin payroll separate from clinician payroll, then watch whether compliance, scheduling, and billing can run without extra layers.
Use a simple control list: rent, HIPAA IT, insurance, licenses, and admin wages. If one cost grows, offset it with more booked hours or less non-clinical time. The goal is not cheap staffing; it’s enough support staff to protect care without turning overhead into a drag on owner income.
- Track overhead monthly.
- Split fixed and variable costs.
- Watch admin payroll growth.
- Protect billable utilization.
5
Owner Role And Scalable Capacity
Owner Role and Scalable Capacity
When the owner bills therapy, cash can start sooner, but the ceiling stays low because one person’s time caps volume. In this model, the owner as a clinician can create early billable revenue, yet that role limits growth. Staff scale from 20 to 108 over five years, so income shifts toward managing capacity instead of doing every billable hour.
The tradeoff is hard cash pressure. Center-based growth adds fixed overhead from Month 1, including $19,800/month of fixed costs and admin payroll rising from $385k to $790k a year. If the owner hires faster than demand, payroll drag can hit profit and delay owner pay.
Hire to demand, not to hope
Track booked hours, active clients, and authorization coverage before adding staff. Capacity per provider is only about 40 to 45 monthly BCBA supervisor treatments, 120 to 130 RBT treatments, or 100 to 110 speech or occupational therapy treatments, so headcount should follow real session demand.
- Watch filled hours weekly.
- Track denials and payment lag.
- Keep cash for slow payer cycles.
- Delay hiring until sessions fill.
Scalable capacity helps only when utilization, meaning paid time that turns into billable sessions, stays ahead of headcount. If scheduling gaps or payer delays widen, owner income falls fast because fixed payroll and rent keep running.
6
Compare low, base, and high owner income scenarios without treating them as guarantees
Owner income scenarios
Owner income changes fast with utilization, collections, staffing mix, and payroll pressure. The low, base, and high cases show how much cash the owner can safely pull out.
| Scenario | LowConservative | BaseOperating plan | HighStretch |
|---|---|---|---|
| Launch model | Lower utilization and slower collections keep owner pay light or delayed. | Steady utilization and cleaner collections support a normal owner draw. | Stronger utilization and tighter collections push owner income higher. |
| Typical setup | Cancellations run higher, clinician payroll feels tight, and cash gets tied up in receivables before the owner takes much out. | Therapy volume scales across BCBA supervisors, RBTs, speech, OT, and psychology while fixed overhead stays near $19,800 a month. | Staffing stays stable, admin load stays lean, and better cash conversion lifts take-home after payroll and overhead. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | Delayed owner drawDownside draw | Modeled owner drawModel draw | Upside owner drawUpside draw |
| Best fit | Use this to stress test cash strain, delayed pay, and a tougher staffing month. | Use this as the core operating case for budgeting, hiring, and lender talks. | Use this to test upside when volume is strong and collections stay clean, but full take-home still needs payroll, reserves, taxes, and debt. |
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Autism Support Service Porter's Five Forces Analysis
- Autism Support Service BCG Matrix
- Autism Support Service Business Model Canvas
- What Are The Five Core KPIs For Autism Support Service Business?
- Autism Support Service Business Plan Template in Pre-Written Word
- How Increase Autism Support Service Profits?
- What Does It Cost To Run Autism Support Service?
- Autism Support Service Startup Costs: $310K CAPEX, $820K Cash Need
- Autism Support Service Financial Model Template in Excel
- How To Open An Autism Support Service In 8 Weeks To 6 Months
- How To Write A Business Plan For Autism Support Service?
- Autism Support Service Marketing Mix
- Autism Support Service Marketing Plan
- Autism Support Service Business Proposal
- Autism Support Service PESTEL Analysis
- Autism Support Service Pitch Deck Example Editable PPTX
- Autism Support Service Business SWOT Analysis
- Autism Support Service Value Proposition Canvas
Frequently Asked Questions
The provided data supports revenue, not a final owner income claim Revenue is $143M in Year 1 and $1228M in Year 5 After listed variable costs, fixed overhead, and admin payroll, cash before direct clinician payroll, reserves, debt, and taxes is about $511k to $966M, so owner pay must be modeled below that ceiling