 Time to Open6 monthsLaunch runway
Time to Open6 monthsLaunch runwayStart an Aviation Medical Examiner Practice in 3 to 9 Months

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description

Time to Open6 monthsLaunch runway  Launch Sequence5 stagesCompliance first
Launch Sequence5 stagesCompliance first Key BottleneckLicense gateApproval path
Key BottleneckLicense gateApproval path First Revenue StepFirst bookingBooking live
First Revenue StepFirst bookingBooking live


Key Takeaways
- FAA designation gates launch before any exam revenue.
- Office setup must support privacy, vitals, and workflow.
- MedXPress checklists cut rework and opening-month delays.
- Staffing and runway must match expected booking volume.
Time to Open6 monthsLaunch runwayLaunch Sequence5 stagesCompliance firstKey BottleneckLicense gateApproval pathFirst Revenue StepFirst bookingBooking liveLaunch timeline
Short web summary of the launch timeline; the XLSX export includes the detailed Gantt Chart.
Launch scheduleMonth 1Month 2Month 3Month 4Month 5Month 6Month 7Month 8Month 9
FAA compliance
- Eligibility review
- Application packet
- MedXPress setup
- Inspection prep
- Certificate decision
Facility setup
- Lease signed
- Suite buildout
- IT setup
- Safety setup
- Opening inspection
Equipment
- Vendor quotes
- Order equipment
- Delivery check
- Calibrate devices
- Test workflow
Staffing
- Hire coordinator
- Hire assistants
- Train staff
- Set schedules
- Ramp coverage
Marketing
- Partner outreach
- Clinic list
- Landing page
- Local campaign
- Referral follow-up
Finance
- Model validation
- Price review
- Billing setup
- Cash plan
- Go-live gate
Why test the Aviation Medical Examiner Practice ramp before opening?
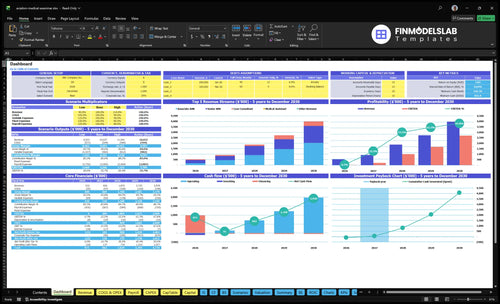
The dashboard and model tabs show launch timing, appointment volume, pricing, staffing, runway, breakeven, and the monthly ramp; open Aviation Medical Examiner Practice Financial Model Template.
Financial model highlights
- Year 1 staffing set
- 1 Senior, 1 Associate
- 1 Consultant, 2 MAs
- No Nurse Practitioner
- Senior: 160, 65%, $250
- Associate: 180, 40%, $180
- Consultant: 40, 30%, $450
- $44,360 monthly role revenue
- $42,166 payroll plus fixed
- Breakeven needs volume lift
- Startup costs need input
How long does it take to open an AME practice?
An Aviation Medical Examiner Practice usually takes 3 to 9 months to open, and an existing medical office can move faster if privacy, equipment, scheduling, and payment workflows are already in place. A new aviation-focused clinic needs more time for FAA AME designation, exam equipment, staff training, FAA MedXPress workflow, and local referral marketing, so don’t promise a fixed opening date until compliance and readiness are confirmed.
Faster launch
- Existing office cuts setup time
- Privacy already in place
- Scheduling works from day one
- Payment flow already ready
Delay risks
- FAA designation can slow launch
- Equipment procurement takes time
- Staff training needs setup time
- First referrals may start weak
How do you become an FAA aviation medical examiner before opening?
You become an Aviation Medical Examiner Practice founder by first holding an active state medical license, completing required Federal Aviation Administration (FAA) AME training, and receiving FAA AME designation before offering FAA medical certificate exams; budget planning can run beside that path using What Does It Cost To Run An Aviation Medical Examiner Practice?. Treat designation as a launch gate, not admin work, because pilots need certificates across 3 FAA classes and your office must be ready for MedXPress, issuance, deferrals, records, malpractice, and trained intake.
Designation first
- Start with active state licensure
- Complete FAA-required AME training
- Secure FAA AME designation
- Follow official FAA policy materials
Open ready
- Set up FAA MedXPress workflow
- Train intake before launch
- Document issuance and deferral steps
- Confirm malpractice coverage scope
How do you get patients for an AME practice?
Patients for an Aviation Medical Examiner Practice usually come from local aviation relationships first, not broad healthcare branding, so start with flight schools, aviation academies, fixed-base operators, airport bulletin boards, pilot groups, student pilots, and private pilots; for cost context, see What Does It Cost To Run An Aviation Medical Examiner Practice?. Set up local search visibility, a complete business profile, clear exam slots, payment expectations, and MedXPress prep before opening. That makes first bookings easier and cuts avoidable no-shows.
Where bookings come from
- Target flight schools first
- Use airport bulletin boards
- Build pilot group ties
- Focus on renewals and student pilots
How to test demand
- 104 Senior AME visits monthly
- 72 Associate AME visits monthly
- 176 total monthly visits at capacity
- Match demand to Year 1 volume
Build the AME practice opening checklist before the first pilot appointment
Launch readiness checklist
Use this go-live approval checklist to confirm the practice is ready before opening.
Licensing
- State medical license activeCritical
No license, no launch; the clinic can't issue exams without this gate.
- FAA AME path approvedCritical
FAA designation must be in place before any pilot medical can be issued.
- Malpractice and HIPAA policies readyCritical
Coverage and privacy rules need to be active before patient data flows.
Clinic setup
- Exam room readyHigh
The room must support a full FAA physical without extra handoffs.
- Vitals workflow testedHigh
Vitals steps need to run fast and the same way for every patient.
- Vision and hearing tools calibratedCritical
Calibration proof protects exam quality and avoids rework on launch.
Workflow
- MedXPress intake script trainedHigh
Staff need the confirmation number before they book the exam slot.
- Records and privacy flow setHigh
Charting and privacy need one clear path from intake to storage.
- Payment collection testedHigh
If payment fails at check-in, visits slow down and cash slips.
Staffing
- First-month staffing scheduledHigh
Coverage must match expected demand from the first operating month.
- Billing and records clerk readyMedium
Back office needs a person for records, follow-up, and billing.
- Clinical handoffs rehearsedHigh
Clean handoffs cut delays between assistant, examiner, and consultant.
Demand
- Local flight schools contactedHigh
Nearby pilots need a steady source of appointments from day one.
- Fixed-base operators in pipelineHigh
Fixed-base operators can send steady referrals if they know the offer.
- Search listings publishedMedium
Search visibility matters for first bookings and local trust.
Finance
- Payroll and overhead modeledCritical
Year 1 fixed overhead is $10,750 a month, and payroll is about $31.4k.
- Cash covers trough in Month 2Critical
The model shows minimum cash of $852k in Month 2, so opening cash matters.
- Unit economics testedHigh
Year 1 variable costs run about 17.5% of revenue, and breakeven is Month 13.
- Go-live signoff completeCritical
Do not open until compliance, workflow, staffing, and referral checks are green.
Want to see the six main AME practice launch drivers?
1FAA Designation
FAA gateThe practice cannot do FAA physical exams until the physician's AME designation, state license, malpractice coverage, and workflow training are active.
2Office Setup
$95.5KThe first pilot visits only run cleanly if the exam room, privacy, vitals, vision, hearing, internet, and equipment calibration are ready.
3MedXPress Flow
ChecklistA written MedXPress intake and issuance checklist cuts rework by standardizing confirmation numbers, documentation, and deferral routing.
4Pilot Network
80%Year 1 fill depends on flight schools, airport groups, and local aviation channels, where aviation community marketing drives most revenue.
5Staff Capacity
8 FTEDay-one throughput depends on a tested booking path and the Year 1 team mix across clinical, front desk, and records work.
6Cash Runway
$852KCash falls to a $852K minimum in Month 2, and breakeven does not arrive until Month 13, so funding has to cover the early ramp.
FAA AME designation readiness
AME designation readiness
FAA AME designation is the gate that decides whether this practice can see pilots on day one. If the physician’s designation, training, and FAA workflow are not complete before opening, marketing can still create demand, but the clinic cannot perform FAA medical exams, which turns a planned launch into a delay.
The readiness signal is simple: active state license, malpractice coverage, confirmed designation path, and a clear certification workflow. This includes training, process review, documentation setup, and staff education, because a scheduled opening means nothing if the physician cannot legally complete exam duties yet.
Pre-open FAA checklist
Lock the sequence before you publish dates. First verify the physician’s designation path and FAA process steps, then finish training and document the front-desk and clinical workflow. If any of those pieces slip, opening-day capacity drops to zero for FAA exams, even if the office, staff, and marketing are ready.
- Confirm designation path status
- Check state license and coverage
- Finish FAA workflow training
- Set exam forms and scripts
- Train staff on intake steps
What this hides: the risk is binary. Either the physician can perform FAA exams, or the clinic cannot serve its core customer from day one.
1
Clinical office and exam equipment readiness
Exam Room Readiness
Complete room readiness is what keeps the clinic open on schedule and lets the first pilot be seen without scrambling. The room has to support privacy, vitals, vision screening, hearing workflow, documentation, reliable internet, and calibration-ready equipment. If any of that is missing, you get delays, slower charting, and rescheduled exams on day one.
The fixed burn starts before the first appointment: $6,500 medical suite rent, $950 utilities and high-speed internet, $300 equipment calibration, and $550 janitorial and biohazard disposal. That is $8,300/month before supplies or staff, so a late room setup directly adds cash pressure while revenue is still zero.
Run the Full Room Check
Stage the room with a generic exam table, diagnostic wall unit, and EKG equipment when required. Then test the full patient path: check-in, vitals, vision, hearing, documentation, and exit. The goal is simple: one complete dry run before the first pilot appointment, with no gaps in tools, forms, or internet access.
- Verify privacy and exam flow.
- Confirm calibration documents.
- Test internet and charting.
- Stock supplies before opening.
- Run one mock patient visit.
If the room only works on paper, the clinic will slow down on live visits. A broken workflow can turn a 20-minute exam into a longer visit, create backlogs, and push pilots into another day. Day-one readiness means the room, tools, and documentation all work together before anyone books.
2
MedXPress and certification workflow control
MedXPress Intake Control
MedXPress is the FAA’s online medical application workflow used before the exam, and it sets the pace for opening month. If intake, confirmation numbers, exam documents, certificate steps, special issuance flags, and deferral routing are not tight on day one, the clinic will lose time to rework, reschedules, and missed records instead of moving pilots through cleanly.
The readiness signal is a written front-desk and clinician checklist that everyone follows the same way. That matters because the model carries 20% FAA MedXPress processing fees in Year 1 and 45% medical consumables and lab kits, so sloppy workflow quickly turns into wasted spend and slower first-revenue exams. This is operational workflow planning, not legal or medical advice.
Lock the exam flow before first appointments
Build the intake sequence before opening, then test it with a mock pilot visit. The front desk should confirm the application is complete, collect the confirmation number, route the chart to the clinician, and file the exam record the same day. One clean script beats a pile of apologies.
- Verify confirmation number handling.
- Document special issuance and deferrals.
- Test certificate issuance steps end to end.
- Assign one owner for rework follow-up.
- Track missing forms before the visit starts.
If the checklist is weak, opening day still happens, but exams slow down and staff spend time chasing documents instead of completing visits. A tight workflow keeps the room moving, protects patient experience, and lowers the chance of avoidable delays in the first month.
3
Pilot referral network
Pilot referral network
First revenue depends on being visible where pilots already ask for medical certificate exams. If the clinic is open but pilots cannot find it, the first month turns into empty slots, slow cash in, and wasted AME time. In this model, aviation community marketing drives 80% of Year 1 revenue, then drops to 55% by Year 5, so launch-day visibility is not optional.
Build referral paths with flight schools, aviation academies, fixed-base operators, airport communities, airport bulletin boards, student pilot groups, private pilot groups, and local aviation associations. The readiness signal is simple: booked outreach meetings, a live local search profile, a clear exam page, and opening-month appointment slots. That setup helps push utilization toward 65% for the Senior AME and 40% for the Associate AME in Year 1.
Build the referral map before opening
Start with a named outreach list and track each contact by source, meeting date, and next step. Verify that the search profile is live, the exam page says exactly what pilots need, and the booking calendar has real slots in the first month. If any of those are missing, pilots will bounce before the first appointment is booked.
Use a simple launch checklist: meetings booked, referral contacts logged, appointment slots open, and incoming calls answered fast. The goal is not broad marketing; it is being easy to find in the places where pilots already search. Without that, day-one operations may be staffed and ready, but demand will still lag.
- Book flight-school outreach first
- Confirm local search visibility
- Publish the exam page early
- Open first-month appointment slots
- Log every referral source
4
Scheduling and staffing capacity
Scheduling and staffing capacity
Day-one performance depends on whether a pilot can book, check in, pay, and finish the exam without handoffs breaking the flow. The readiness test is a booked path from first call to completed documentation, not just a full calendar. Year 1 staffing assumes 1 Lead AME Medical Director, 1 Clinic Manager, 1 Patient Coordinator, 1 Senior AME, 1 Associate AME, 1 Case Consultant, and 2 Medical Assistants, with no Nurse Practitioner.
The Year 1 wage load is about $31,400/month before fixed overhead, so weak scheduling turns into idle payroll fast. If appointment availability, front desk training, patient intake, payment collection, reminders, records handling, or exam slot design are not tested before opening, same-week access still fails at the front desk. That means reschedules, slower visits, and delayed first revenue.
Test the full booking path
Before opening, run one live test from first call to completed paperwork. Confirm who answers, how slots are assigned, how payments are collected, and where records are stored. One clean script matters more than extra marketing.
Use a written checklist for intake, reminders, documentation, and exam-room turnover. If a pilot needs more than one handoff to finish the visit, capacity is already slipping.
- Train front desk before launch
- Map every patient handoff
- Set exam slot lengths
- Assign backup coverage
- Test documentation before day one
5
Financial ramp and cash runway
Cash runway and launch gap
If appointment volume comes in light, this clinic can open late or open stressed. The Year 1 model shows about $44,360/month in revenue, with $36,600/month of contribution left after variable costs, but $31,400/month of payroll and $10,750/month of fixed overhead leave a roughly $5,600/month gap before other items.
That means the launch date should not be locked until you know how many pilot bookings or ancillary services close the gap. Here’s the quick math: if bookings slip, cash burn starts on day one, and even a small delay in ramp can shorten runway fast. One clean rule: don’t open until the first-month booking plan matches the staffing plan.
Validate the gap before you set the date
Build the opening plan around the stated capacity assumptions for Senior AME, Associate AME, and Case Consultant. Then test whether the expected appointment volume, pricing, and marketing ramp actually support those numbers before hiring and spending hit full speed.
- Match booked slots to staff capacity.
- Stress test the first 90 days of cash.
- Delay hires until demand is visible.
- Track bookings needed to close $5,600/month.
If marketing ramps slower than planned, the clinic still carries payroll and overhead. That’s why runway should be measured in months of cash, not hope. A short opening delay is cheaper than opening with too few exams to cover the monthly gap.
6
Related Products
- Aviation Medical Examiner Practice Porter's Five Forces Analysis
- Aviation Medical Examiner Practice BCG Matrix
- Aviation Medical Examiner Practice Business Model Canvas
- What 5 KPIs Should Aviation Medical Examiner Practice Business Track?
- Aviation Medical Examiner Business Plan Template in Pre-Written Word
- How Increase Aviation Medical Examiner Practice Profits?
- What Does It Cost To Run An Aviation Medical Examiner Practice?
- Aviation Medical Examiner Practice Startup Costs: $852K Cash Need
- Aviation Medical Examiner Financial Model Template in Excel
- How Much Aviation Medical Examiner Practice Owners Make: $240K+
- How To Start An Aviation Medical Examiner Practice?
- Aviation Medical Examiner Practice Marketing Mix
- Aviation Medical Examiner Practice Marketing Plan
- Aviation Medical Examiner Practice Business Proposal
- Aviation Medical Examiner Practice PESTEL Analysis
- Aviation Medical Examiner Practice Pitch Deck Example Editable PPTX
- Aviation Medical Examiner Practice Business SWOT Analysis
- Aviation Medical Examiner Practice Value Proposition Canvas
Frequently Asked Questions
Start with physician eligibility, active state licensure, and the FAA AME designation path Then prepare the exam room, FAA MedXPress workflow, malpractice coverage, scheduling, payment collection, and pilot referral sources Use the 3 to 9 month launch range as a planning guide, and test whether Year 1 volume can cover about $42,166/month in fixed overhead and payroll