 Owner income$181k-$4.72M
Owner income$181k-$4.72MHow Much Balance Disorder Clinic Owners Make In 5 Years

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$181k-$4.72M  Net margin21.7%-72.8%
Net margin21.7%-72.8% Revenue for target pay$835k-$6.48M
Revenue for target pay$835k-$6.48M Business difficultyHard
Business difficultyHard


A balance disorder clinic owner can make meaningful income once visits, payer collections, and clinician utilization cover the fixed cost base In this researched model, annual revenue rises from $835,000 in Year 1 to $6479 million in Year 5, while EBITDA rises from $181,000 to $4718 million If the owner also fills the Medical Director role, the model includes a $210,000 annual salary before any distributions Actual owner take-home depends on payer mix, staffing, debt service, taxes, reserves, and how much cash stays in the clinic
Owner income$181k-$4.72MNet margin21.7%-72.8%Revenue for target pay$835k-$6.48MBusiness difficultyHardWant to test your own owner pay?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: Research-based planning estimate only. It is not guaranteed salary, tax advice, or owner distribution advice.
Want to check owner income in the Balance Disorder Treatment Clinic financial model?
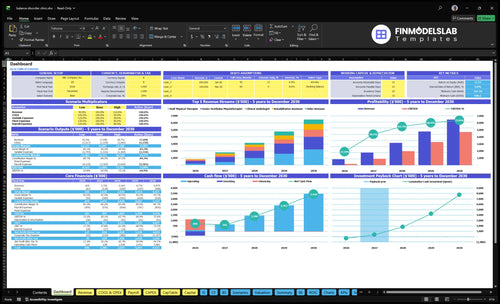
Open the Balance Disorder Treatment Clinic Financial Model Template to see owner take-home, dashboard, assumptions, cash flow, and scenario tests.
Owner-income model highlights
- Revenue $835k to $6479 million
- EBITDA $181k to $4718 million
- Utilization and cost tables
- Minimum cash $640,000
- 18-month payback, 994% IRR, 1157% ROE
How much revenue does a balance disorder clinic need to pay the owner?
For a Balance Disorder Treatment Clinic, owner pay should come from collections, not billed charges. Year 1 adds $19,400 a month in fixed expenses, $429,000 in annual wages, and variable costs listed at 190% of revenue, while collected revenue averages about $170 per completed treatment ($835,000 / 4,920). So the owner draw sits last, after payroll, lease, insurance, billing, marketing, and reserves.
Cash first
- $19,400 fixed monthly cost
- $429,000 annual wage base
- $170 collected per treatment
- 4,920 Year 1 treatments
Pay order
- Use collections, not billed charges
- Pay payroll before owner draw
- Cover lease, insurance, billing, marketing
- Keep reserves before taking profit
What balance disorder clinic operating costs reduce owner income most?
Owner income gets squeezed most by wage payroll, the $12,500 monthly facility lease, $2,200 professional liability insurance, $1,800 EHR and HIPAA IT support, and billing and claims processing at 60% of Year 1 revenue. In Year 1, the variable cost stack reaches 190% and still runs at 143% by Year 5, so collections pressure is the real problem; if you’re planning the model, How To Write Balance Disorder Treatment Clinic Business Plan? keeps the math honest. No-shows and denials cut cash directly, so they hit owner income fast.
Biggest monthly drains
- Payroll is the biggest lever.
- $12,500 lease hits every month.
- $2,200 liability insurance is fixed.
- $1,800 IT support stays on.
Capital and collection pressure
- $120,000 clinic fit-out comes first.
- $85,000 posturography platform adds upfront strain.
- $65,000 rotational chair system raises capex.
- $45,000 VNG system also ties up cash.
Is a balance disorder clinic profitable if the owner treats patients?
The Balance Disorder Treatment Clinic can be profitable if the owner treats patients, because a licensed owner-clinician can keep the clinical margin that would otherwise go to a hired Medical Director, modeled at $210,000. The hired-provider model only works well if utilization, referral flow, scheduling, and payer collections stay strong. In Year 1, the clinic can run with 2 senior vestibular physiotherapists, 1 audiologist, 1 staff physical therapist, and 1 rehab assistant.
Owner-operated model
- $210,000 salary value stays in-house.
- Works best if licensed and credentialed.
- Keeps control over quality and diagnosis.
- Shorter path to positive unit economics.
Scale and staffing
- Year 1: 4 clinical roles plus rehab support.
- Hired model depends on referral volume.
- Collections and scheduling drive margin.
- Year 5 needs more supervision and reinvestment.
What drives owner take-home most?
1
$835K-$6.48MPatient Volume
More completed visits push annual revenue from $835K in Year 1 to $6.48M in Year 5.
2
$90-$275Payer Mix
Better payer and reimbursement mix lifts what each treated case brings in, so the same visit count earns more.
3
3.1xService Mix
Shifting toward higher-priced specialty care raises average revenue per visit and supports the jump in EBITDA margin.
4
40%-85%Provider Utilization
Moving staff from 40% to 85% utilization spreads wages across more visits and lifts take-home fast.
5
$19.4K/moFixed Overhead
The $19.4K monthly fixed base must be covered first, but it gets easier to absorb as revenue scales and EBITDA margin expands.
6
14.3%-19.0%No-Shows
Fewer missed visits keep the schedule full, and that helps variable costs fall from 19.0% to 14.3% later.
Balance Disorder Treatment Clinic Core Six Income Drivers
Patient Volume And Referrals
Completed Visits Drive Cash
This clinic’s income comes from completed visits, not inquiries. Year 1 is modeled at about 410 completed treatments per month across senior vestibular physiotherapists, a clinical audiologist, a staff physical therapist, and a rehabilitation assistant, so referral flow from otolaryngology, neurology, and primary care has to stay steady or revenue slips before the schedule fills.
Here’s the quick math: if referrals lag hiring, schedules stay underfilled and break-even moves out. That hits cash flow first, then owner distributions. One missed visit is lost collection, while payroll, rent, and admin still run. The key input is not lead count; it’s booked, attended, and billed visits that actually turn into cash.
Track Referral-to-Visit Conversion
Measure each source separately: referrals received, appointments booked, and visits completed. That shows where the funnel leaks. If one channel sends volume but no kept visits, it won’t pay the fixed overhead of $19,400 per month.
Use a simple weekly dashboard: completed visits by provider, no-shows, and source mix. If the clinic is missing the 410-visit plan, slow hiring, tighten reminders, and push referral follow-up before adding more labor. More filled slots lift revenue before fixed costs rise, which is what protects owner pay.
- Track booked visits by referral source.
- Watch no-shows and cancellations weekly.
- Compare planned versus completed visits.
1
Reimbursement And Payer Mix
Collected Reimbursement Per Visit
Collected reimbursement per visit drives owner income more than billed charges here. Year 1 prices range from $90 for rehabilitation assistant services to $250 for clinical audiologist services, and Year 5 rises to $110 to $275. The real input is payer mix across Medicare, commercial insurance, and cash-pay, because the same visit can collect very different dollars.
Here’s the quick math: if collections slip from coding errors, denials, or billing lag, revenue falls but payroll and rent do not. Billing and claims processing starts at 60% of revenue and improves to 50% by Year 5, so every $100,000 in revenue frees up about $10,000 more for owner pay by then.
Tighten Payer Mix And Claims
Track denials, coding accuracy, billing lag, and claims cost by payer. Use a simple forecast with visit count, price per visit, payer mix, and collection timing. If Medicare or commercial claims slow down, cash flow tightens fast, even when billed revenue looks healthy.
- Split visits by payer source.
- Measure denial rate weekly.
- Watch days in A/R.
- Test price by service type.
2
Service Mix
Service Mix
Evaluations, vestibular testing, therapy visits, and follow-up care change revenue per patient episode because each service pays differently. In Year 1, a clinical audiologist visit is $250, a staff physical therapist visit is $150, and a rehabilitation assistant visit is $90. If the schedule skews toward lower-priced visits, revenue per clinic day falls even when the calendar looks full.
The key input is the mix by service role and visit type, not just total visits. Capacity planning has to match clinician slots, or the clinic gets the wrong revenue mix, slower collections, and less cash for owner pay. A full $250 slot matters more than a lower-priced slot when fixed payroll and rent stay the same.
Track revenue per slot
Build the weekly schedule around service blocks: evaluations, testing, therapy, and follow-up. Track collected revenue per completed visit by role, and watch the share of $250, $150, and $90 slots. That tells you fast whether higher-value work is being crowded out before owner distributions shrink.
- Completed visits by clinician role
- Collected revenue per episode
- Open slots by service type
- Days from visit to cash
Use the mix to set staffing, then adjust templates so the right clinician is in the right room at the right time. If rehab assistant slots fill while audiology slots stay open, the clinic can look busy but still miss cash targets. That’s the revenue trap.
3
Staffing And Provider Utilization
Provider Utilization Drives Owner Pay
Owner take-home rises when payroll matches actual patient demand, not planned headcount. In Year 1, the model uses 650% utilization for senior vestibular physiotherapists, 500% for the clinical audiologist, 600% for the staff physical therapist, and 400% for the rehabilitation assistant. If schedules stay underfilled, collections lag and payroll still runs.
Keep owner-operated capacity separate from hired-provider capacity. Hiring ahead of demand adds payroll burden, admin scheduling, credentialing delays, and cancellation risk, so the same visit volume can leave less cash for owner draw. By Year 5, utilization reaches 850% across the listed clinical roles, which means the model expects tighter scheduling and better labor efficiency.
Track Capacity Before You Hire
Measure booked hours, completed visits, and cancellation rates by role. Those inputs tell you whether demand can support another clinician or whether current staff should absorb more visits first. In plain terms: if the calendar is soft, payroll is too heavy.
Add headcount only when referral flow, credentialing status, and rebook rates can fill the next schedule block. What this estimate hides is the cash drag from slow payer setup and last-minute gaps, both of which can cut owner income fast.
- Track booked versus available hours weekly.
- Separate owner hours from hired hours.
- Watch cancellations by provider.
- Delay hiring until schedules hold.
4
Fixed Costs And Equipment Overhead
Fixed Costs and Equipment Overhead
Fixed costs of $19,400 per month set the break-even line before owner pay. That includes the lease, EHR and HIPAA IT support, liability insurance, utilities, office expenses, and calibration. If visit volume or collections slip, profit disappears fast because these costs run every month whether the schedule is full or not.
Launch overhead also matters: $407,000 in capex for diagnostic systems, fit-out, testing booth, IT, screening tools, furniture, and treatment tables, with minimum cash need peaking at $640,000 in Month 6. That means take-home income depends on having enough cash to survive the ramp, not just enough demand on paper.
Track Cash Burn and Break-Even
Track monthly collections, fixed overhead, and cash on hand against the $19,400 run rate. Here’s the quick math: owner pay starts only after fixed costs are covered, so every extra visit that adds margin helps fund distributions. The key inputs are visit volume, reimbursement per visit, and any delay in collections.
Watch the launch cash path each month through Month 6. If cash falls faster than planned, slow hiring and control spending on nonessential equipment adds. What this estimate hides is timing risk: even strong revenue can miss owner pay if collections lag while capex and overhead keep running.
5
Retention And No-Shows
Completed Visits
Retention and no-shows decide how much demand turns into cash. Here’s the quick math: if a $185 senior vestibular physiotherapist visit no-shows, revenue drops by $185, but payroll, rent, and billing still run. So the owner’s take-home gets squeezed even when the schedule looks full.
Track scheduled visits, completed visits, cancellations, no-shows, and follow-up adherence. Poor follow-through hurts predictable cash flow, and with fixed costs at $19,400 per month, lower completion rates can delay owner distributions fast.
Track and Recover Missed Visits
Use completion rate as the main control. If bookings rise but completed visits lag, the clinic is leaking revenue. Model a simple gap: scheduled minus completed equals lost billable visits, and that lost volume shows up as weaker collections and thinner owner pay.
- Measure no-show rate by provider.
- Send reminders before each visit.
- Confirm follow-up before discharge.
- Review referral source communication.
6
Compare low, base, and high owner-income scenarios
Owner income scenarios
Owner income moves with visit volume, claim quality, and how fully the specialty team is used. The model clears break-even by Month 2, but the upside depends on keeping schedules full.
| Scenario | Low CaseLow Case | Base CaseBase Case | High CaseHigh Case |
|---|---|---|---|
| Launch model | Slower visits, more denials, and limited diagnostic volume keep owner income tied mostly to role pay. | The core model supports modest owner income from salary plus early distributions once volume normalizes. | Mature utilization and a fuller provider bench push owner income into the upside case. |
| Typical setup | The clinic runs below plan, with lighter volume, a smaller diagnostic mix, and tighter collections. | The clinic follows the modeled case with $835,000 Year 1 revenue, $181,000 EBITDA, Month 2 break-even, $640,000 minimum cash, and an 18-month payback. | The clinic reaches Year 5 scale at $6.479 million revenue and $4.718 million EBITDA, with margin badges of 217% in Year 1, 501% in Year 2, 627% in Year 3, 689% in Year 4, and 728% in Year 5. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | Role salary onlyLow income case | Modest salary plus distributionsBase income case | Upside distribution caseHigh income case |
| Best fit | Use this to stress-test a lean owner-operated clinic with weak early utilization. | Use this as the core specialty clinic case for planning and lender conversations. | Use this to test a high-utilization, multi-provider clinic with strong throughput. |
Planning note: Scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distribution targets.
Related Products
- Balance Disorder Treatment Clinic Porter's Five Forces Analysis
- Balance Disorder Treatment Clinic BCG Matrix
- Balance Disorder Treatment Clinic Business Model Canvas
- How Increase Profitability Of Balance Disorder Treatment Clinic?
- Balance Disorder Treatment Clinic Business Plan Template in Pre-Written Word
- How Increase Profits Balance Disorder Treatment Clinic?
- What Does It Cost To Run A Balance Disorder Treatment Clinic?
- Balance Disorder Clinic Startup Costs: $315K+ Before Runway
- Balance Disorder Clinic Financial Model Template in Excel
- How To Open A Balance Disorder Treatment Clinic In 6–12 Months
- How To Write Balance Disorder Treatment Clinic Business Plan?
- Balance Disorder Treatment Clinic Marketing Mix
- Balance Disorder Treatment Clinic Marketing Plan
- Balance Disorder Treatment Clinic Business Proposal
- Balance Disorder Treatment Clinic PESTEL Analysis
- Balance Disorder Treatment Clinic Pitch Deck Example Editable PPTX
- Balance Disorder Treatment Clinic Business SWOT Analysis
- Balance Disorder Treatment Clinic Value Proposition Canvas
Frequently Asked Questions
The model shows $181,000 of Year 1 EBITDA and $4718 million by Year 5 before taxes, debt service, reinvestment, and reserves If the owner also works as Medical Director, the wage plan includes $210,000 per year Actual take-home depends on cash policy and distributions