 Owner income$130k
Owner income$130kHow Much Does A Birth Center Owner Make? $130k Plus Profit

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description

Owner income$130k  Net margin-4%
Net margin-4% Revenue for target pay$1.06M
Revenue for target pay$1.06M Business difficultyHard
Business difficultyHard


Key Takeaways
- Volume drives revenue; Year 1 is barely break-even.
- Staffing must match births or payroll crushes margin.
- Fixed costs keep running at $17,400 monthly.
- Ancillary services help, but births still pay the bills.
Owner income$130kNet margin-4%Revenue for target pay$1.06MBusiness difficultyHardWant to test your birth center income?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: This is a research-based planning estimate only. It is not guaranteed salary, tax advice, or owner distribution advice.
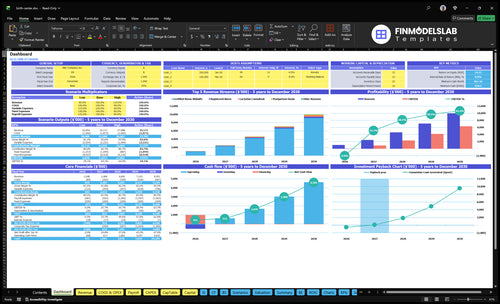
Want to check owner income in the Birthing Center model?
The screenshot shows revenue, margin, costs, reserves, and owner take-home assumptions. Open the Birthing Center Financial Model Template.
Owner-income model highlights
- Owner salary and draws
- Revenue and EBITDA view
- Scenarios for cash flow
What costs reduce birth center owner income?
Clinical payroll is the biggest cost that cuts owner income at a Birthing Center, before any distributions. For setup context, see How Much Does It Cost To Open A Birthing Center? Year 1 payroll is $590,000, fixed overhead is $17,400 a month, and revenue-based costs hit 195% in Year 1, so cash gets tight fast.
Main cost drains
- $590,000 Year 1 payroll
- $150 million by Year 5
- $12,000 lease or mortgage
- $1,500 utilities monthly
Other income reducers
- $800 general liability insurance
- $1,200 professional fees
- 60% medical supplies cost
- $431,000 minimum cash in Month 12
Does a birth center owner make more if they work as a midwife?
Yes. In a Birthing Center, the owner can take home more cash earlier if they fill the Lead Certified Nurse-Midwife Director role, because that pay is modeled at $130,000 a year and is separate from business profit and distributions. But Year 1 EBITDA is -$47,000, so distributions are not supported yet, even if the owner earns the clinical salary.
Owner pay first
- $130,000 director salary is separate.
- Year 1 EBITDA: -$47,000.
- No profit distribution in Year 1.
- Manager-run ops cut owner workload.
Scaling tradeoff
- CNMs scale from 2 to 6.
- More CNMs raise revenue capacity.
- More staff also need backup coverage.
- Labor savings can become burnout risk.
How many births per month does a birth center need to be profitable?
A Birthing Center needs about 11 completed birth packages per month to cover Year 1 operating costs, with model breakeven in Month 13; track this alongside What Is The Most Critical Indicator To Measure The Success Of Your Birthing Center? because volume alone won’t save weak collections.
Quick Math
- Year 1 revenue: $1.05 million
- Volume: about 10 births/month
- Year 1 EBITDA: -$47,000
- Breakeven need: about 11 births/month
Watch Limits
- Match volume to midwife coverage
- Check room capacity before scaling
- Track transfers and payer collections
- No national breakeven number fits all
Want the six birth center income drivers?
1
10-864/moBirth volume
Birth packages rise from 10 a month in Year 1 to 234 in Year 2 and 864 in Year 5, so volume drives most take-home income.
2
$8K-$8.8KBirth pricing
The birth package price moves from $8,000 to $8,800, so even small rate gains lift revenue fast.
3
$590K-$1.5MStaffing mix
Payroll starts near $590K and reaches about $1.5M, so hiring pace and FTE mix decide what stays after labor.
4
$17.4K/moFixed overhead
Lease, utilities, insurance, software, cleaning, and admin costs set a $17.4K monthly floor before profit starts.
5
$13K-$23K/moAncillary revenue
Lactation, childbirth education, registered nurse, and postpartum doula work add extra income without needing another birth.
6
40%-92%Client flow
Better conversion and fewer transfers keep more cases in house and protect utilization across the care team.
Birthing Center Core Six Income Drivers
Birth Volume
Birth Package Volume
Completed birth packages drive most revenue. At $8,000 per Year 1 package, each added birth brings cash before supplies, labs, malpractice, outreach, payroll, and overhead. With about 10 birth packages per month in Year 1, EBITDA is about negative $47,000; at 234 per month in Year 2, EBITDA reaches $881,000.
The key inputs are completed births, low-risk eligibility, room capacity, on-call coverage, hospital transfers, and referral flow. One clean truth: no completed birth, no margin spread. Higher steady volume helps owner take-home only after reserves are funded.
Track Completed Births
Watch the funnel each month so you can see where volume leaks out. Track inquiries, consults, booked packages, completed births, and transfer rate. If referrals slow or risk-outs rise, revenue drops fast because fixed costs do not wait.
- Booked-to-completed birth rate
- Low-risk screening pass rate
- Room and on-call capacity
- Transfers and lost revenue
Protect volume by matching staffing and space to realistic demand, and keep referral sources warm. Each added birth should clear the $8,000 revenue step before you add payroll or room count.
1
Payer Mix
Payer Mix
Payer mix is the share of births covered by private insurance, Medicaid, and self-pay. It changes the average collected revenue per birth, so owner pay can move even when birth volume does not. With a model price of $8,000 per Year 1 birth package, rising to $8,800 by Year 5, collection quality drives cash, not just billed revenue.
Here’s the quick math: if reimbursement falls or gets paid late, the business may need more than the modeled 11 break-even births per month to cover the same fixed load. Credentialing delays, state rules, contract exclusions, denials, and bad debt all hit EBITDA and cash reserves before they show up in headline volume.
Control collections
Track collection rate, deposit timing, denial rate, and payment lag by payer. Build the forecast on cash collected per birth, not just booked births, so owner distributions reflect money in hand. Private insurance, Medicaid, and self-pay should each have their own rules, because they affect cash flow and bad debt differently.
- Collect deposits before service.
- Review denials by payer.
- Model lag days monthly.
- Recheck contract exclusions often.
2
Clinical Staffing Model
Clinical Staffing Load
Payroll is the throttle on owner income here. The model puts Year 1 payroll at $590,000, with a Lead Certified Nurse-Midwife Director at $130,000, Certified Nurse-Midwives at $110,000, Registered Nurses at $75,000, plus support roles. Year 1 staffing includes 2 Certified Nurse-Midwives and 2 Registered Nurses, then grows to 6 of each by Year 5.
Here’s the quick math: every added clinician raises fixed cost before it adds enough births to pay for itself. Owner-clinician coverage can save cash early, but it also pushes call, charting, and patient care onto the owner. If staffing runs ahead of birth volume, margin shrinks fast and owner draw gets squeezed.
Right-Size the Care Team
Track headcount against completed births, not hope. The core inputs are birth volume, coverage hours, on-call load, and the pay rate for each role. Use the role mix to test whether each $110,000 CNM and $75,000 RN is supporting enough delivered packages to keep labor efficient. If the team is underfilled, call coverage gaps and burnout rise.
What to measure each month: births per clinician, call shifts per owner, overtime, and transfer rate. A right-sized model protects gross margin and cash flow, while overhiring locks in payroll before revenue catches up. For this business, staffing should follow low-risk birth volume, not the other way around.
3
Fixed Facility And Insurance Costs
Fixed Facility Overhead
$17,400 a month in fixed overhead means the center pays the same bill whether it books 0 births or 10. That total includes $12,000 lease or mortgage, $1,500 utilities, $800 general liability insurance, $1,000 cleaning, and $1,200 accounting or legal fees. With Year 1 birth packages at $8,000 each, fixed overhead alone needs about 2.2 births per month before any owner pay.
Fixed costs do not flex. If births slow, margin and cash flow tighten fast because these bills still hit every month. The $485,000 buildout capex also matters because overbuilt space and reserve drain can squeeze working cash. What this estimate hides is the rest of care delivery cost, so owner distributions only make sense after fixed overhead is covered and reserves stay intact.
Right-Size the Space
Track fixed overhead ÷ monthly collected revenue and stress test it at 0, 2, and 4 births. Build the forecast from the real inputs: lease, utilities, insurance, cleaning, and accounting or legal fees. If the space needs extra rooms, security, or sterilization gear to meet licensing rules, add those costs before you open.
- Model rent against low volume.
- Watch reserve coverage monthly.
- Delay nonessential buildout upgrades.
- Keep fixed costs tied to demand.
4
Client Conversion And Transfers
Eligible Birth Conversion
Inquiries only matter when they become completed, low-risk births. The gate is consult-to-client conversion plus risk screening: if a lead books but fails eligibility, revenue drops while staff time is already spent. With CNM capacity modeled at 50% in Year 1 and 90% by Year 5, more of each inquiry must survive intake and stay in care to support owner pay.
One transfer before completion can cut collected birth-package revenue, depending on contract and billing terms. So the owner should tie pay to completed births, not scheduled starts, and watch continuity of care closely.
Track Transfers Before They Hit Cash
Measure the funnel in order: inquiry, consult, accepted client, completed birth, transfer. The key ratio is completed births ÷ consults, plus transfer rate. If intake is weak, you overstate revenue and owner draw. Conservative transfer modeling is the safer call because a planned birth that transfers may only collect part of the package.
- Watch consult-to-client conversion
- Flag risk-outs at intake
- Log every transfer reason
- Match billing to contract terms
5
Ancillary Revenue
Ancillary Services Revenue
Ancillary revenue adds money per family through Registered Nurse services, lactation consulting, childbirth education, and postpartum doula visits. In Year 1, that’s about $7,320 per month, or $87,840 a year. The prices given are $150 for a Registered Nurse service, $200 for a lactation consult, $300 for childbirth education, and $180 for a postpartum doula visit.
This helps owner income when staff time is already in place, because more service revenue can flow through with limited new fixed cost. The catch is simple: it does not replace birth volume. If classes run light or scheduling gets messy, you can add payroll strain without enough cash back, which hurts take-home profit.
Track service fill and labor use
Measure each service line by booked visits, attendance, staff hours, and cash collected. Here’s the quick math: revenue equals service price times delivered volume across the four offerings. If a class or consult uses staff time but stays underfilled, margin drops fast.
- Track revenue per family.
- Watch class fill rates.
- Match staffing to booked demand.
- Cut low-volume time blocks.
6
Compare lean, base, and high birth center owner-income cases
Owner income scenarios
Income moves with the ramp: Year 1 is a loss, Year 2 turns profitable, and Year 3 scales further. Payouts still depend on reserves, debt, taxes, staffing, and payer mix.
| Scenario | Low CaseLow Case | Base CaseBase Case | High CaseHigh Case |
|---|---|---|---|
| Launch model | Year 1 stays in ramp-up, with EBITDA (operating profit before interest, taxes, depreciation, and amortization) at -$47k, so owner income is mostly salary. | Year 2 is the profit case, with EBITDA at $881k, so distributions are possible if reserves, debt, and taxes allow. | Year 3 is the scale case, with EBITDA at $2.331m, so payout room improves if reserves stay strong. |
| Typical setup | Year 1 runs with 2 certified nurse-midwives, 2 registered nurses, 1 lactation consultant, 1 childbirth educator, and 1 postpartum doula. | Year 2 adds one certified nurse-midwife and one registered nurse, and the center moves into positive EBITDA. | Year 3 reaches 4 certified nurse-midwives and 4 registered nurses, which supports the strongest payout path if cash is preserved. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $130,000 salary onlyLow Case Salary | $130,000 + possible distributionsBase Case Upside | $130,000 + stronger distributionsHigh Case Upside |
| Best fit | Use this if you want a cautious ramp model with no payout assumed. | Use this if you are planning around profitable operations and reserve checks. | Use this to test the strongest owner payout path after reserves and taxes. |
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Birthing Center Porter's Five Forces Analysis
- Birthing Center BCG Matrix
- Birthing Center Business Model Canvas
- 7 Core Financial KPIs to Track for a Birthing Center
- Birthing Center Business Plan Template in Pre-Written Word
- 7 Strategies to Increase Birthing Center Profitability and Margin
- How Much Does It Cost To Run A Birthing Center Each Month?
- Birthing Center Startup Costs: $485K CAPEX and $431K Cash Need
- Birthing Center Financial Model Template in Excel
- How To Open A Birthing Center: 9-18 Month Launch Roadmap
- How to Write a Birthing Center Business Plan: 7 Actionable Steps
- Birthing Center Marketing Mix
- Birthing Center Marketing Plan
- Birthing Center Business Proposal
- Birthing Center PESTEL Analysis
- Birthing Center Pitch Deck Example Editable PPTX
- Birthing Center Business SWOT Analysis
- Birthing Center Value Proposition Canvas
Frequently Asked Questions
A birth center owner can take a $130,000 salary if they serve as the Lead Certified Nurse-Midwife Director in this model Profit distributions are not supported in Year 1 because EBITDA is negative $47,000 By Year 2, EBITDA reaches $881,000, but that is before taxes, reserves, debt service, and reinvestment