 Time to Open9 monthsLaunch runway
Time to Open9 monthsLaunch runwayHow To Start A Chronic Care Management Service With A 30-Month Breakeven

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description

Time to Open9 monthsLaunch runway  Launch Sequence6 stagesCompliance first
Launch Sequence6 stagesCompliance first Key BottleneckBilling gateProvider alignment
Key BottleneckBilling gateProvider alignment First Revenue StepFirst claimCCM claim live
First Revenue StepFirst claimCCM claim live


Key Takeaways
- Billing readiness protects first revenue from denials.
- Provider partnerships drive eligible patients and workflows.
- Care tech must match billing and documentation.
- Cash runway must cover slower revenue and hiring.
Time to Open9 monthsLaunch runwayLaunch Sequence6 stagesCompliance firstKey BottleneckBilling gateProvider alignmentFirst Revenue StepFirst claimCCM claim liveLaunch timeline
This short web summary shows the launch sequence, and the XLSX export holds the detailed Gantt Chart.
Launch scheduleMonth 1Month 2Month 3Month 4Month 5Month 6Month 7Month 8Month 9Month 10Month 11Month 12
Legal / compliance
- Draft provider agreements
- Build HIPAA packet
- Prepare consent forms
- Review billing rules
- Sign compliance checklist
Platform / security
- Install security stack
- Buy IT hardware
- Map EMR workflow
- Configure platform
- Test billing flow
Facilities / equipment
- Secure office lease
- Order furniture
- Set up office
- Receive hardware
- Finish fit-out
Staffing / training
- Hire core team
- Onboard coordinators
- Train staff
- Assign call scripts
- Run mock cases
Marketing / intake
- Build referral list
- Launch outreach
- Create intake scripts
- Start lead capture
- Track conversion
Finance / operations
- Set up payroll
- Define billing rules
- Build forecast
- Test invoicing
- Go-live review
Why test the Chronic Care Management Service model before launch?
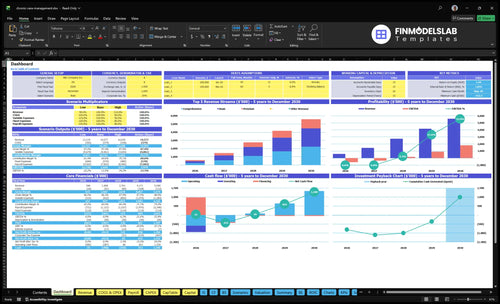
Use the Chronic Care Management Service Financial Model Template to test the dashboard and model tabs, timing, cash, and break-even. It maps Months 1-12 build, Months 1-6 office fit-out, Months 3-6 training, and Months 4-9 EMR integration.
Key model checks
- Office fit-out and build
- 60/30/10 mix, $99-$299
- Month 30 break-even path
How do you get patients for chronic care management?
For a Chronic Care Management Service, patients usually come first through primary care practices, clinics, and healthcare organizations with eligible Medicare patients, not broad consumer ads; see How Increase Chronic Care Management Service Profitability? First revenue depends on provider trust and billing readiness, then the flow is patient list review, eligibility check, consent capture, care plan setup, monthly contact, documentation, and compliant claim submission. A Year 1 marketing budget of $300,000 with $450 CAC means you need tight provider relationships, and that can improve to $300 CAC by Year 5. Make patient ownership, consent language, and contact cadence explicit in agreements.
Patient sources
- Start with primary care practices.
- Target clinics with Medicare patients.
- Work with healthcare organizations.
- Trust beats broad advertising.
Launch flow
- Review patient lists first.
- Check eligibility and capture consent.
- Set the care plan.
- Run monthly contact and claims.
What are the requirements to start a chronic care management service?
To start a Chronic Care Management Service, set up the legal entity, lock down HIPAA controls, sign business associate agreements, insure the operation, staff licensed clinical roles, and align provider supervision, consent, documentation, time tracking, and billing before launch; see What Are The Operating Costs For Chronic Care Management Service? for the cost side. Budget at least $4,500/month for HIPAA legal retainer, insurance, and software, plus 2 care coordinator FTEs in Year 1, and confirm legal, medical, and payer rules with qualified advisors.
Launch Requirements
- Set up the business entity
- Get healthcare counsel review
- Build HIPAA privacy controls
- Sign business associate agreements
Operating Checks
- Carry $1,200/month liability insurance
- Plan $1,800/month HIPAA legal retainer
- Budget $1,500/month software licenses
- Verify staff, consent, billing rules
How long does it take to launch a chronic care management service?
A Chronic Care Management Service does not launch on a fixed date; it starts when the compliance, staffing, and systems work is done. In the setup plan, data security starts in Month 1, IT hardware by Month 2, and office fit-out runs through Month 6, while EMR integration can stretch to Month 9 and custom platform work to Month 12. First revenue can begin only after compliant enrollment and service documentation are ready.
Launch build
- Month 1: data security
- Month 2: IT hardware
- Month 3: furniture
- Months 3-6: staff training
Common delays
- Provider agreements slow go-live
- Credentialing can block billing
- HIPAA documentation must be ready
- Patient consent must be collected
Confirm what must be ready before accepting CCM patients
Launch readiness checklist
Use this go-live approval checklist to confirm the service is ready before opening.
Compliance
- Business registration completeCritical
You need a legal entity before contracts, accounts, and vendor onboarding start.
- Healthcare counsel review completeCritical
Use the HIPAA retainer to clear launch risks in policies, contracts, and workflows.
- HIPAA policies writtenCritical
Written rules are the base line for handling patient data and staff access.
- BAAs signedCritical
Business associate agreements must be signed before vendors touch protected data.
- Professional liability insurance boundHigh
The $1,200 monthly policy should be live before patient work starts.
Platform
- EHR platform selectedCritical
The care record system must be chosen before setup, training, and go-live.
- CRM licenses activeHigh
The $1,500 monthly software stack has to be active for intake and follow-up work.
- Data security controls liveCritical
Security systems should be live before any protected health data is handled.
- Billing codes mappedCritical
Mapped codes prevent missed charges and bad claim setup in the first month.
- Billing exports testedCritical
Exports must work before launch because billing breaks can delay cash.
Care flow
- Care plan templates approvedHigh
Approved care plans keep patient work consistent across coordinators and cases.
- Patient consent workflow testedCritical
Consent has to work cleanly before any outreach, tracking, or billing starts.
- Supervising provider workflow agreedCritical
Provider oversight must be clear so care staff know who signs off and when.
Staffing
- Care coordinators trainedCritical
Care teams need the same steps for outreach, follow-up, and documentation.
- Documentation process auditedHigh
Audited notes reduce c laim errors and protect the chart trail.
- Time tracking testedCritical
Time tracking must work because missing minutes can break billing.
- Escalation paths setHigh
Staff need a clear path for urgent symptoms, provider questions, and handoffs.
Revenue
- Referral sources identifiedCritical
You need a clear referral list before the first patient intake push.
- Enrollment intake readyHigh
A fast intake flow helps convert referrals into active patients.
- First billing run testedCritical
The first billing run should be tested before live claims or invoices go out.
Finance
- Month 30 runway fundedCritical
Breakeven is Month 30, so cash has to carry the business to that point.
- Year 1 cash gap coveredCritical
Year 1 revenue is $596,000 and EBITDA is -$577,000, so the early gap is real.
- Go-live signoff completeCritical
Do not launch until compliance, workflow, and cash checks all pass.
Want to see the six CCM launch drivers?
1Compliance Billing Readiness
CPT 99490Clean billing, consent, and time records keep first claims from getting denied.
2Provider Partnerships
Signed partnersSigned practice referrals unlock eligible patients and stabilize the first billable workflow.
3Care Tech Setup
M1-M12Secure software, EMR links, and exports cut manual workarounds and billing delays.
4Coordinator Capacity
2 FTETwo care coordinators in Year 1 set the first patient panel and follow-up load.
5Enrollment Workflow
$300K / $450 CACA $300K marketing plan and $450 CAC must turn referrals into billable enrollments.
6Revenue Runway
M30 / M29Breakeven lands in Month 30, but cash still bottoms at -$552K in Month 29.
Compliance And Medicare Billing Readiness
Medicare Billing Readiness
For a chronic care management service, billing readiness is the launch gate. If HIPAA policies, business associate agreements, patient consent records, care plan documentation, time tracking, and the supervising provider workflow are missing, Medicare billing can stop on day one. That matters because billing errors and thin records can block revenue even when the care work is already happening.
Here’s the quick math on setup cost: a $1,800 monthly HIPAA legal retainer plus $1,200 monthly professional liability insurance adds up to $3,000 per month before launch. Build the CPT 99490 documentation path, billing-code accuracy checks, and claim review before opening, so the first claims are cleaner and the launch does not depend on fixes after go-live.
Prelaunch Billing Check
Before you open, have counsel review the compliance setup, then bring in a billing expert to audit the records flow. Test the full path from consent to care plan to time log to claim, and confirm the supervising provider signs off the way Medicare requires. If any step is manual or unclear, fix it before patient enrollment starts.
Use a short launch list: HIPAA policies, BAAs, consent forms, documentation audit, test claim workflow. That sequence helps prevent denied claims, keeps staff from guessing on billing rules, and gives you a cleaner first revenue month instead of a messy rework cycle.
1
Provider Partnership Model
Provider Partnership Model
Provider partnerships matter because they open the door to eligible patients and the billable workflow that lets a chronic care management service start on time. If the agreement, patient ownership, referral flow, supervising provider role, consent responsibility, and escalation path are not clear, the business may have referrals but no clean way to enroll or bill from day one.
The launch risk is highest when a practice sends patients before the workflow is tested. That can create consent gaps, broken handoffs, and stalled care plan approval. Strong partnerships with primary care practices, clinics, and healthcare organizations should also line up billing alignment, EHR access, staff communication, and reporting cadence so the first claims are more likely to go through cleanly.
Test the referral path before go-live
Before opening, get the signed agreement in place and document who owns the patient, who gives consent, who supervises, and who escalates issues. Then map the referral steps inside the practice, confirm EHR access, and test care plan approval with staff so there is no guesswork when the first patient comes in.
Use a simple launch checklist: referral flow, supervising provider roles, escalation process, reporting cadence, and consent responsibility. If any of those are still informal, the partnership is not ready for live referrals, and first-revenue timing can slip even when the contract is signed.
- Confirm patient ownership.
- Test referrals before launch.
- Align billing and EHR access.
- Assign consent responsibility.
- Set reporting and escalation rules.
2
Care Management Technology Setup
Care Management Tech Setup
The service can’t open cleanly unless the software handles a patient registry, care plans, secure communication, time tracking, documentation, reporting, and billing exports from day one. The main dependency is the fit between the platform workflow and the provider billing process; if staff use manual workarounds, records split and claims slow down.
Here’s the quick math on timing: custom platform development runs Months 1-12, EMR integration runs Months 4-9, data security systems start in Month 1, and IT hardware lands in Months 1-2. Add $1,500 monthly for CRM and software licenses. Any slip here turns opening day into cleanup work.
Test the Billing Path First
Before launch, test the full path from referral to billable record: consent, care plan creation, secure note capture, time tracking, export, and claim handoff. That sequence has to work without staff patching gaps by hand.
Also verify HIPAA vendor agreements, user access, and audit trails before the first patient goes live. The goal is simple: fewer billing delays and cleaner operations, not a fancy build that needs constant rework.
3
Clinical Staffing And Coordinator Capacity
Clinical Staff Capacity
Year 1 starts with 2 care coordinator FTEs at $82,000 each, so base clinical payroll is $164,000 before support roles. That matters because this service only opens cleanly if licensed staff are hired, trained, and ready to document, follow up, and escalate on day one. If enrollment outruns staffing, service quality drops fast and first claims can slip.
Training runs Months 3-6, so the launch plan has to match real ramp, not just headcount on paper. The staffing path grows to 4 FTEs in Year 2, 7 in Year 3, 10 in Year 4, and 12 in Year 5, with 1 customer success FTE, 0.5 IT FTE, and 0.5 marketing FTE in Year 1. One clean rule: don’t let patient growth outrun care follow-up capacity.
Capacity and launch check
Build the operating model around panel capacity and documentation load, not just enrollment targets. Before opening, verify staffing schedules, escalation rules, visit-note templates, and who closes each patient touch. Test whether the team can document, route issues, and finish follow-up within the same week.
Put the first launch gate on training completion and supervised workflow tests during Months 3-6. If referrals start before the team can chart cleanly and hand off urgent issues, the business can miss service promises and create avoidable compliance and cash strain. Keep early enrollment tied to what 2 care coordinator FTEs can truly handle.
4
Patient Enrollment And Consent Workflow
Enrollment And Consent Flow
This launch driver decides whether referred patients become billable members fast enough to open on time. In chronic care management (CCM), the path runs from eligibility check to benefit explanation, consent capture, care plan setup, monthly contact scheduling, and service-time documentation. If any handoff breaks, you get consent leakage between referral and first documented service, and first revenue slips.
With $300,000 in Year 1 marketing and $450 CAC, the model implies about 667 enrollments before churn. At the stated mix of 60% Basic, 30% Comprehensive, and 10% Premium, the starting average price is $149 per member per month. That only works if the audit trail is live from day one; weak scripts or missing documentation turn paid leads into unbilled work.
Verify The First Handoff
Before launch, test the full sequence in order: eligibility screen, consent script, care plan template, registry entry, contact cadence, provider escalation, and time log. If the team can’t move a patient from referral to first documented service in one clean workflow, opening on time is a paper launch, not an operating launch.
- Use one consent script.
- Assign one owner per handoff.
- Test audit trail on day one.
- Log monthly contact before go-live.
What this hides: if provider turnaround is slow, the pipeline can look healthy while billable starts lag. So verify that referrals, consent, and documentation all land in the same system before you commit to marketing spend and staffing. One missed step can delay cash and force manual rework.
5
Revenue Ramp And Cash Runway
Cash Runway
Cash timing sets the launch speed. This CCM service can open on paper before it can safely scale in practice, because enrollment ramps faster than cash arrives. With revenue at $596,000 in Year 1 and EBITDA still at -$577,000, the first months need enough cash to cover payroll, coordinator training, and billing lag.
The pressure point is the gap between service delivery and reimbursement. Breakeven lands in Month 30, payback in Month 56, and minimum cash hits -$552,000 in Month 29. If payroll comes before claims cash, hiring too early can force a launch delay or a hard pause in enrollment even when demand is there.
Match Hiring To Cash
Build the launch plan around cash, not hope. Before opening, map the first 6 to 12 months of enrollment, coordinator capacity, reimbursement timing, and billing lag. Tie each hire and each marketing dollar to a cash checkpoint so the team does not outgrow the runway before the first claims cycle clears.
Track three things from day one: monthly enrollment, payroll due dates, and expected reimbursement dates. Here’s the quick math: revenue is expected to rise from $596,000 in Year 1 to $1.458 million in Year 2, then $2.761 million in Year 3. If actual enrollment slips, slow hiring first, because the cash shortfall shows up before the revenue ramp does.
- Set a cash floor before launch.
- Sequence hires after reimbursement tests.
- Review billing lag every month.
- Hold marketing spend to capacity.
6
Related Products
- Chronic Care Management Service Porter's Five Forces Analysis
- Chronic Care Management Service BCG Matrix
- Chronic Care Management Service Business Model Canvas
- What 5 KPIs Should Chronic Care Management Service Business Track?
- Chronic Care Management Business Plan Template in Pre-Written Word
- How Increase Chronic Care Management Service Profitability?
- What Are The Operating Costs For Chronic Care Management Service?
- Chronic Care Management Service Startup Costs: $363K CAPEX Plan
- Chronic Care Management Financial Model Template in Excel
- Chronic Care Management Owner Income: $596K Revenue To Year 3 Profit
- How To Write A Business Plan For Chronic Care Management Service?
- Chronic Care Management Service Marketing Mix
- Chronic Care Management Service Marketing Plan
- Chronic Care Management Service Business Proposal
- Chronic Care Management Service PESTEL Analysis
- Chronic Care Management Pitch Deck Example Editable PPTX
- Chronic Care Management Service Business SWOT Analysis
- Chronic Care Management Service Value Proposition Canvas
Frequently Asked Questions
Start by setting up the entity, HIPAA policies, provider workflow, care management platform, consent process, and billing documentation The researched model starts operations in Month 1, trains staff in Months 3-6, and integrates EMR workflows in Months 4-9 It assumes $596,000 in Year 1 revenue but negative EBITDA of -$577,000, so launch readiness and cash runway matter