 Owner income($40K) to $2.0M
Owner income($40K) to $2.0MHow Much Colon Hydrotherapy Clinic Owners Make: $396K EBITDA

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income($40K) to $2.0M  Net margin-8% to 72%
Net margin-8% to 72% Revenue for target pay$543K
Revenue for target pay$543K Business difficultyHard
Business difficultyHard


A colon hydrotherapy clinic owner can make little or nothing in the first year if the clinic is still ramping In the researched case, the clinic shows -$40K EBITDA in Year 1, then improves to $396K in Year 2 and $2042M in Year 5 Those figures are planning assumptions, not guaranteed salary Actual owner take-home depends on session volume, average ticket, staffing, rent, insurance, marketing, debt payments, and cash reserves
Owner income($40K) to $2.0MNet margin-8% to 72%Revenue for target pay$543KBusiness difficultyHardWant to test your owner pay?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: Research-based planning estimate only. It is not guaranteed salary, tax advice, or owner distribution advice.
Want to check owner income in the Colon Hydrotherapy Clinic model?
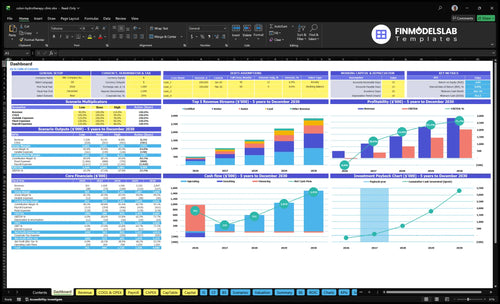
This dashboard shows revenue, margin, costs, reserves, and owner draw assumptions. Open the Colon Hydrotherapy Clinic Financial Model Template.
Owner-income model highlights
- $501K Year 1 revenue
- $1.028M Year 2 revenue
- $2.847M Year 5 revenue
- Breakeven in Month 13
- Payback in 23 months
- Minimum cash $761K
- IRR 887%, ROE 484%
- Scenario planning only
How many colon hydrotherapy sessions per week are needed?
For a Colon Hydrotherapy Clinic, plan on about 81 sessions per week to break even and about 98 sessions per week to support a $100K annual owner-pay target before reserves and taxes. The year-1 model shows about 324 booked sessions per month at 60% capacity, $418K in monthly revenue, and an average ticket near $129.
Break-even math
- 352 sessions per month breaks even
- That equals 81 sessions per week
- Based on $129 average ticket
- Utilization drives the result
Owner-pay target
- 424 sessions per month supports target pay
- That equals 98 sessions per week
- Assumes $100K annual owner pay
- Staffing and overhead still matter
How much profit does a colon hydrotherapy clinic make?
A Colon Hydrotherapy Clinic can show researched EBITDA of -$40K in Year 1, $396K in Year 2, $832K in Year 3, $1.454M in Year 4, and $2.042M in Year 5; for planning details, see How To Write A Business Plan For Colon Hydrotherapy Clinic?. EBITDA means profit before interest, taxes, depreciation, and amortization, so it excludes personal taxes and debt service.
Profit path
- Year 1: -$40K EBITDA
- Year 2: $396K EBITDA
- Year 3: $832K EBITDA
- Year 5: $2.042M EBITDA
What profit covers
- Subtract treatment supplies and practitioner labor
- Subtract rent, utilities, insurance, marketing
- Subtract staff, software, maintenance, reserves
- Manager salary is not owner distribution
How does solo versus staffed clinic ownership change income?
A solo owner usually keeps more cash early in a Colon Hydrotherapy Clinic because they do the treatments and the management work, but income is capped by one person’s schedule. A staffed multi-room clinic can scale to $10.28M in Year 2 and $28.47M in Year 5 as utilization rises from 70% to 85%, but payroll can eat the upside fast. Here’s the quick math: the real driver is room utilization and payroll control, not staffing by itself.
Solo owner
- Keeps more early cash.
- Does treatments and admin.
- One schedule limits volume.
- Lower fixed payroll pressure.
Staffed scale
- Clinic manager: $130K.
- Front desk: $48K.
- Part-time admin, marketing, maintenance, bookkeeping.
- Works if rooms reach 85% use.
Want the six biggest income drivers?
1
3.9K-19.1KSession Volume
More treatments is the biggest revenue lever, rising from 3,888 annual sessions in Year 1 to 19,074 in Year 5.
2
60%-85%Room Utilization
Moving capacity from 60% to 85% spreads fixed room costs over more paid visits and lifts margin.
3
$129-$149Average Ticket
A higher ticket price lifts revenue without adding the same number of extra sessions.
4
98%-69%Labor Model
The practitioner mix matters because direct costs fall from 98% to 69% as the schedule and staffing get more efficient.
5
$14.8K/moOverhead Control
Monthly fixed costs sit near $14.8K, so rent, utilities, and insurance can push breakeven out fast.
6
HighRepeat Retention
Keeping clients coming back fills open slots and cuts the cost of replacing them with new leads.
Colon Hydrotherapy Clinic Core Six Income Drivers
Session Volume
Booked Sessions
Session volume is the first driver of owner pay because each booked treatment turns fixed clinic time into revenue. In Year 1, the model shows about 324 sessions per month and negative EBITDA; break-even sits near 81 sessions per week. Year 2 rises to about 633 sessions per month and $396K EBITDA, so the owner’s draw starts to depend on how fast booked visits scale.
What matters is not room count alone. The risk is assuming new rooms fill up without repeat bookings and local referral flow. If demand stalls, extra capacity just adds payroll and overhead, and owner income stays thin even when the schedule looks busy.
Track Fill, Rebook, Referrals
Measure booked sessions per week, repeat booking rate, and referral source before adding capacity. Use the Year 1 break-even mark of 81 sessions weekly as the first test, then watch whether volume comes from returning clients or new leads. That tells you if owner income is sustainable or just a short spike.
- Track sessions weekly
- Separate new vs repeat bookings
- Watch no-shows and rebooks
- Measure referral traffic by source
If bookings rise but repeat rate stays weak, new rooms will not protect profit. Tie scheduling to follow-up reminders, package rebooking, and local referrals so the clinic can hold 324 monthly sessions in Year 1 and move toward the higher-volume Year 2 run rate.
1
Average Ticket
Average Ticket
The average ticket is the blended price per treatment. In Year 1, that’s about $129, with tier prices from $95 for junior sessions to $200 for master sessions. By Year 5, the blend rises to about $149, with prices from $115 to $220. Since direct treatment costs are under 10% in Year 1, price changes flow fast into profit and owner pay.
What drives this metric is the mix of full-price sessions, packages, and memberships, plus how much discounting you allow. Here’s the quick math: if a session sells for $129 and direct cost stays below $13, most of the extra dollar can reach gross profit. Deep discounts help fill slots, but they can wipe out cash for rent, payroll, and the owner draw.
Price the Mix, Not Just the Session
Track blended ticket by provider, tier, and sales channel. Split out standard visits, packages, and memberships so you can see where margin leaks. If the local wellness market won’t support your target price, adjust the offer mix before cutting rates. Avoid health outcome claims and price on service quality, privacy, and experience.
- Measure full-price share each month.
- Cap discounts before margin drops.
- Test package prepay and renewals.
- Watch contribution after direct cost.
Use pricing to support cash flow, not just bookings. A stronger ticket can cover fixed overhead faster, while a weak ticket forces higher volume just to hold owner income flat. If packages stabilize bookings, make sure the discount still leaves room for payroll, supplies, and profit. One bad promo can cost more than ten extra sessions help.
2
Room Utilization
Room Utilization
Room utilization is the share of available appointment capacity that actually gets booked. Here it moves from 60% in Year 1 to 70% in Year 2 and 85% in Year 5, so the same room base produces more visits and spreads rent, software, insurance, and front desk payroll across more treatments.
The catch is schedule design. Intake, session time, sanitation, room turnover, and realistic operating hours all eat capacity. Overbooking can hurt client experience and raise compliance risk, which can push repeat bookings down and cut owner pay even when top-line volume looks strong.
Track booked slots, not hope
Build the schedule around booked slots divided by available slots. A move from 60% to 85% utilization does not change fixed costs, but it does lift contribution by filling more of the same room hours. One empty hour is lost margin, and every filled hour helps cover overhead before owner draw.
Watch no-shows, late cancels, turnover time, and bookings by practitioner. Keep buffers for intake and sanitation, then use reminders, deposits, or waitlists before you ever double-book. If capacity gets tight, protect service quality first; bad flow can erase the gain from higher utilization.
- Booked slots / available slots
- No-show and late-cancel rate
- Turnover minutes per room
- Utilization by day and practitioner
3
Practitioner Labor Model
Practitioner Mix and Owner Pay
Who performs the treatment drives how much cash stays with the owner. This model grows from 7 practitioners in Year 1 to 21 in Year 5 across junior, certified, senior, lead, and master tiers. If the owner works sessions, payroll pressure is lower, but owner pay is tied to hours in the room. If hired staff do the work, income scales better, but only when bookings are full.
The key inputs are sessions per practitioner, utilization, and labor cost by tier. A staffed room only helps if demand fills it; otherwise payroll turns into margin drag. The owner should separate labor savings from owner income, because the first can rise while the second stays flat if the calendar is thin.
Track Labor by Booked Session
Measure sessions per practitioner per day, owner-operated share, and payroll as a percent of revenue. Add headcount only when repeat bookings keep rooms busy, not just when demand looks good for one month. If a new hire is paid but a room sits empty, gross margin drops fast and owner take-home shrinks.
Use a simple rule: grow staff only when booked sessions can support the next tier. In a service model like this, the best labor mix is the one that keeps the owner out of low-value chair time and puts paid practitioners in filled slots. One empty room can erase the benefit of a lower wage bill.
4
Client Retention
Client Retention
Repeat visits matter because this clinic earns per treatment, so keeping clients coming back is what turns one appointment into stable monthly cash flow. The model grows from 3,888 annual treatments in Year 1 to 19,074 in Year 5, or about 324 to 1,590 treatments per month. If first-visit clients do not rebook, the owner has to buy more traffic just to stand still.
The main inputs are repeat-appointment rate, membership sign-ups, package renewals, referral traffic, and how often staff secure the next booking before the client leaves. One clean rule: book the next visit before checkout. That simple step protects revenue quality, steadies labor planning, and improves the owner’s take-home income without forcing ad spend up at the same pace.
Measure Rebook Rate
Track first-visit rebook rate, membership conversion, and renewal r ate by practitioner and by month. Here’s the quick math: if monthly treatment volume needs to move from 324 to 1,590, retention has to do real work, not just new leads. Focus on follow-up booking within 24 hours, package reminders, and referral asks after each session.
What this estimate hides is churn after the first visit. If clients leave without a next date, revenue gets lumpy and marketing costs rise. So measure the share of visits that turn into the next visit, and coach staff on booking behavior, not health-benefit promises. That’s what protects margin and keeps more cash available for owner pay.
5
Fixed Overhead
Fixed Overhead
Fixed overhead is the base cost the clinic pays even when sessions are slow. Here it is $148K per month, led by $10K rent, $18K utilities and water, $1K insurance, $700 maintenance, $400 software, $600 supplies, and $300 licenses and certifications. That means gross profit has to clear a very large fixed floor before the owner sees take-home pay.
Here’s the quick math: if monthly gross profit falls below $148K, the gap comes straight out of cash. That’s why the $761K minimum cash need in Month 12 matters. What this estimate hides is local variability; rent, utilities, and licensing can move a lot by state and city, so the owner should not treat it as legal advice.
Control the Fixed Cost Floor
Track fixed overhead as a monthly run-rate, not a yearly average. The owner should split costs into rent, utilities, insurance, software, supplies, and licenses, then test each line against booked sessions and gross profit. One clean rule: every added room or staff hire should be tied to enough session volume to cover its share of the fixed base.
- Watch overhead as a percent of gross profit.
- Compare cost per booked session monthly.
- Stress test slower months and empty rooms.
- Renegotiate rent before adding capacity.
If bookings lag, cut costs fast or pause expansion. Utilities and water at $18K a month are a big swing factor, so usage controls matter. The owner’s income improves when fixed costs stay stable while session volume rises, because more gross profit reaches the bottom line instead of being swallowed by the same monthly bill.
6
Compare low, base, and high owner-income scenarios
Owner income scenarios
Capacity drives owner income here. At 60% to 85% utilization, revenue rises from $501K in Year 1 to $2.847M in Year 5, while EBITDA moves from -$40K to $2.042M.
| Scenario | Low CaseDownside case | Base CaseCore case | High CaseUpside case |
|---|---|---|---|
| Launch model | This is the ramp case: Year 1 runs at 60% capacity and stays cash tight. | This is the modeled case: Year 2 reaches 70% capacity with positive EBITDA. | This is the upside case: Year 5 reaches 85% capacity and breakeven lands in Month 13. |
| Typical setup | The clinic runs about 324 sessions a month, with $501K revenue, -$40K EBITDA, and no assumed owner distribution after reserves. | The clinic runs about 633 sessions a month, with $1.028M revenue and $396K EBITDA, so owner pay depends on reserves and debt terms. | The clinic reaches about 1,590 sessions a month, with $2.847M revenue and $2.042M EBITDA, so it can support stronger draws after reinvestment. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $0Cash tight | $0 - $396KBreak-even zone | $2.0MScale upside |
| Best fit | Use this to test a slow ramp and protect cash if bookings start below plan. | Use this as the main operating plan if you expect steady demand and normal hiring. | Use this to test what strong utilization can support once the clinic is mature. |
Planning note: Scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions; they sit before debt service, reinvestment, and personal taxes.
Related Products
- Colon Hydrotherapy Clinic Porter's Five Forces Analysis
- Colon Hydrotherapy Clinic BCG Matrix
- Colon Hydrotherapy Clinic Business Model Canvas
- What Five Core KPIs For Colon Hydrotherapy Clinic Business?
- Colon Hydrotherapy Clinic Business Plan Template in Pre-Written Word
- How Increase Profits For Colon Hydrotherapy Clinic?
- What Are Operating Costs For Colon Hydrotherapy Clinic?
- How Much It Costs To Open A Colon Hydrotherapy Clinic: $761K Cash Plan
- Colon Hydrotherapy Clinic Financial Model Template in Excel
- How To Open A Colon Hydrotherapy Clinic In 8–16 Weeks
- How To Write A Business Plan For Colon Hydrotherapy Clinic?
- Colon Hydrotherapy Clinic Marketing Mix
- Colon Hydrotherapy Clinic Marketing Plan
- Colon Hydrotherapy Clinic Business Proposal
- Colon Hydrotherapy Clinic PESTEL Analysis
- Colon Hydrotherapy Clinic Pitch Deck Example Editable PPTX
- Colon Hydrotherapy Clinic Business SWOT Analysis
- Colon Hydrotherapy Clinic Value Proposition Canvas
Frequently Asked Questions
The researched model shows a minimum cash need of $761K in Month 12 That reflects the first-year ramp, $163K of capex, and negative Year 1 EBITDA of -$40K It’s a planning figure, not a funding guarantee, because lease terms, financing, and buildout scope can change the cash gap