 Owner income$20.9k/mo
Owner income$20.9k/moComplete Decongestive Therapy Owner Income: $59k/Month Year 1

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description

Owner income$20.9k/mo  Net margin41%-68%
Net margin41%-68% Revenue for target pay$605k/yr
Revenue for target pay$605k/yr Business difficultyMedium
Business difficultyMedium


Key Takeaways
- More completed visits pay only when documented and collected.
- Revenue averages about $190 per visit in Year 1.
- Fixed overhead needs about 66 visits monthly to break even.
- Owner take-home depends on cash and reserves, not profit.
Owner income$20.9k/moNet margin41%-68%Revenue for target pay$605k/yrBusiness difficultyMediumWant to test your CDT clinic owner pay?
Owner income calculator
Estimate owner take-home and the target-pay gap from monthly revenue, gross margin, staffing, fixed overhead, reserves, and target pay.
Planning note: This is a researched planning estimate, not guaranteed salary, tax advice, or owner distribution advice. Actual owner income depends on collections, payer mix, staffing, taxes, debt, and reinvestment.
Want to check owner income in the Complete Decongestive Therapy Service model?
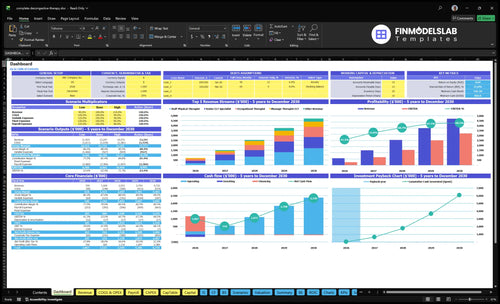
The Complete Decongestive Therapy Service Financial Model Template shows dashboard tabs, revenue, margin, overhead, reserves, break-even, and owner pay before taxes. Open the model.
Owner-income model highlights
- Revenue: $59,075 to $393,525
- Overhead: $9,550 monthly fixed
- Scenarios: Year 1 to Year 5
How much revenue does a lymphedema clinic need to pay the owner?
For a Complete Decongestive Therapy Service, the owner pay target starts with the math: Year 1 contribution is about $146 per collected visit from $59,075 in revenue across 311 visits. With fixed overhead plus core payroll at about $24,633/month, the clinic needs roughly $34,633/month of contribution to fund a $10,000/month owner draw before taxes and reserves. Break-even is about 169 visits/month, so keep salary, draw, and profit distribution separate.
Owner pay math
- $146 contribution per visit
- $59,075 Year 1 revenue
- 311 collected visits
- 77% contribution margin implied
What the owner needs
- $24,633 monthly overhead plus payroll
- $10,000 owner draw target
- $34,633 monthly contribution need
- 169 visits/month to break even
What complete decongestive therapy clinic operating costs most affect margin?
Therapist utilization, denied claims, and fixed overhead hit margin first in a Complete Decongestive Therapy Service; the monthly floor is $9,550 before labor, supplies, and billing drag. For the cost frame, see How Much To Start Complete Decongestive Therapy Service? — Year 1 pressure shows up fast in 85% medical bandaging and clinical supplies, 55% garment inventory, 50% billing and claims processing, and 40% physician referral marketing.
Biggest Leaks
- Therapist labor sets capacity.
- Utilization drives room math.
- Claims denials cut cash fast.
- Documentation load slows visits.
Fixed Cost Floor
- $6,500 rent anchors overhead.
- $1,200 malpractice insurance adds load.
- $450 software and $850 utilities stack up.
- $300 dues and $250 liability stay fixed.
How does solo versus staffed lymphedema clinic income change?
A solo Complete Decongestive Therapy Service can protect margin because the owner keeps the care revenue, but income usually tops out at the owner’s hands-on hours, documentation, patient education, and referral follow-up. A staffed clinic can earn more only if the team stays booked enough to cover payroll, supervision, billing, and room use; Year 1 starts with 4 clinicians and Year 5 grows to 15 clinicians, so scale helps only when utilization and collections keep pace.
Solo model
- Owner-delivered care keeps margin
- Capacity is hands-on limited
- Documentation cuts into clinic time
- Follow-up adds unpaid work
Staffed model
- Year 1: 4 clinicians total
- Year 5: 15 clinicians total
- Payroll must stay covered
- Utilization must stay high
Want to see the main CDT clinic income drivers?
1
311-1,913/moPatient Volume
Year 1 runs at 311 visits a month and Year 5 reaches 1,913, so referral growth is the biggest swing in owner income.
2
$190/visitCollected Yield
At about $190 collected per visit in Year 1, better payer mix and cleaner billing raise revenue without adding many visits.
3
65%-90%Therapist Utilization
Higher therapist use spreads salary over more visits, so full schedules protect margin and empty slots cut take-home fast.
4
4%-5%Collections
Billing and claims run at 5.0% of sales in Year 1 and 4.0% by Year 5, so weak collections leak cash.
5
$9.6K/moFixed Overhead
About $9,550 a month in rent, software, insurance, and overhead means the clinic needs steady volume to stay profitable.
6
$115KOwner Pay
The Clinic Director line is $115,000 a year, and the model also needs $865,000 of minimum cash, so owner pay and reserves both press take-home.
Complete Decongestive Therapy Service Core Six Income Drivers
Patient Volume And Visit Frequency
Visit Volume
The owner only gets paid when visits are completed, documented, and collected. In Year 1, the model uses 311 monthly visits made up of 91 senior CLT, 80 staff physical therapist, 80 occupational therapist, and 60 massage therapist CLT visits; at about $190 per visit, that is roughly $59.1k in monthly revenue.
This driver is fragile: missed visits, authorization delays, or incomplete care plans cut revenue before costs fall. By Year 5, volume rises to 1,913 monthly visits, so room time, charting, and scheduling must scale together. A 10% drop at Year 1 volume is about 31 visits, or roughly $5.9k less cash each month.
Track Completed Visits
Measure scheduled, completed, and documented visits by provider each week. That shows where revenue leaks out, whether from no-shows, slow authorizations, or charting gaps. If the calendar is full but claims are not ready, the clinic is busy without cash, and owner draw gets squeezed.
Watch room use and rebooking speed before adding more referrals. Higher qualified referrals only help if treatment rooms and documentation can keep pace. One clean rule: if completed visits stay below plan for two weeks, fix scheduling, follow-up, and care-plan closeout first, then add staff hours.
1
Average Collected Revenue Per Visit
Collected Revenue Per Visit
This driver is the cash collected per completed visit, not the billed charge. At Year 1 volume, 311 visits and $59,075 in revenue imply about $190 per visit, so payer contracts, patient responsibility, denied claims, and note quality directly shape owner income.
Here’s the quick math: a $10 change in collected revenue per visit moves monthly revenue by about $3,110 at Year 1 volume (311 × $10). Year 1 prices range from $150 for Massage Therapist CLT to $225 for Senior CLT Specialist, and Year 5 ranges from $135 to $250. Lower collections hit cash flow before fixed costs change.
Improve Net Collection Per Visit
Estimate this with visit count, contracted rate, patient copay or coinsurance, denial rate, and documentation quality. Track billed vs. collected by therapist and payer each month so you can see where cash leaks out.
- Watch denial rate by payer.
- Check patient balance collection speed.
- Audit notes before claims go out.
If documentation is weak, the visit is delivered but the cash may never arrive, which cuts owner pay even when the schedule looks full.
2
Therapist Utilization And Labor Model
Therapist Utilization
Utilization is how fully therapist hours and treatment room time turn into collected complete decongestive therapy revenue. In this model, Year 1 utilization ranges from 400% for Massage Therapist CLT to 650% for Senior CLT Specialist, and Year 5 reaches 800% for Junior Clinical Resident and 900% for Senior CLT Specialist. If booked visits do not cover payroll and billing lag, income looks busy but cash stays tight.
Owner-delivered care can protect margin early, but it also caps the owner’s time. Employee therapists raise capacity, yet they add supervision, credentialing, and payroll risk; contractors can lower fixed burn, but they usually add admin load and less control. If referrals are thin, hiring ahead of demand raises fixed burn before revenue catches up.
Measure booked hours, not hope
Track utilization by therapist type, booked visit count, collected revenue per visit, and days from visit to cash. Use one simple rule: only add staff when scheduled visits consistently cover labor burden and claim lag. Here’s the quick math: more therapists help only if the added visits land fast enough to pay wages, supervision, and room time.
- Watch utilization by role weekly
- Compare collected visits to payroll
- Flag billing lag early
- Hire after referrals hold steady
For planning, separate owner clinical hours, employee hours, and contractor hours. That split shows where gross margin is strongest and where admin time is rising. If a role needs more supervision or credentialing than it fills in bookable slots, it can still hurt owner pay even when top-line revenue grows.
3
Payer Mix And Collections
Payer Mix And Collections
For this clinic, owner pay follows collected cash, not scheduled visits. The key inputs are payer mix, authorization rate, claim denial rate, collection lag, patient responsibility, cash-pay share, and billing cost. In Year 1, billing and claims processing are 50% of revenue, or about $29,538 on $59,075 of revenue, so poor collections can absorb a big share of margin fast.
Here’s the quick math: better collections lift cash flow without adding rooms, but delayed authorizations can leave therapists idle while payroll and rent keep running. By Year 5, billing and claims processing fall to 40% of revenue, so cash discipline matters less each month, but the timing gap still drives whether the owner can take a draw on time.
Track the cash, not the schedule
Measure this driver by service line and payer, then compare scheduled visits to collected revenue. Watch days to collect, denial rate, and the share of patient balances paid at checkout. If denials or auth delays rise, cash slows before costs do, so forecast owner draw from collected cash only.
- Track payer mix by visit.
- Track auths before booking.
- Track denials by payer.
- Track patient pay at visit.
- Track billing cost as % revenue.
4
Fixed Overhead And Space Efficiency
Fixed Overhead Sets the Floor
Fixed overhead is $9,550/month, made up of $6,500 rent, $450 for EHR and practice management software, $1,200 malpractice insurance, $850 utilities and maintenance, $300 licensing and dues, and $250 general liability insurance. At a Year 1 contribution of about $146 per visit, t he clinic needs about 66 visits per month just to cover fixed overhead, before payroll, reserves, or owner pay.
This driver includes rent, software, insurance, and other fixed bills, plus room count and how well those rooms stay booked. Extra rooms only help if they’re filled; empty space just raises the cash needed to reach breakeven. Better room use lowers the revenue needed for each owner dollar, but weak scheduling pushes take-home income down fast.
Fill Rooms Before Adding Space
Track visits per month, room utilization, and the gap between scheduled and completed care. If one room stays open, you’re paying for unused square footage. Here’s the quick math: every added fixed dollar must be covered by more visits, so protect schedule density before signing for more space.
- Measure visits per room weekly.
- Watch unused room hours.
- Open space only with demand.
- Forecast overhead before hiring.
Use the 66-visit breakeven floor as the first checkpoint, then test whether higher room fill reduces the revenue needed to support owner pay. If bookings slip, fixed overhead keeps hitting cash flow even when treatment demand looks strong on paper.
5
Owner Role And Cash Reserves
Owner Pay and Cash Reserves
Owner take-home is what’s left after operating needs and reserves, not just net profit. The Clinic Director salary of $115,000/year should be booked separately from profit distributions or owner draw, so the owner can see what work is paid versus what cash is truly free.
Here’s the quick math: early owner clinical hours can lift margin, but admin time grows as staffing and payer work grow. That means cash can tighten even when visits are strong, especially with claim lag and payroll timing. The owner pays themselves from collected cash, not from projected revenue.
Protect Take-Home Cash
Track cash by week, then set aside money for claim lag, payroll timing, equipment replacement, marketing, continuing education, and expansion risk. If collections slow, taking every dollar out weakens the clinic fast. Keep the director salary separate, then decide on any draw only after reserve needs are covered.
- Track collected cash, not billed visits.
- Separate salary from owner draw.
- Watch claims aging each week.
- Flag payroll dates before distributions.
- Review reserve use by category.
When owner clinical hours rise, margin can improve first, but admin load usually follows. So the right test is simple: if the clinic can cover salary, overhead, and reserves after collections settle, then owner pay is sustainable.
6
Scenario objective: compare low, base, and high complete decongestive therapy service owner income assumptions
Owner income scenarios
Owner income moves with visit volume, collection quality, pricing, and staffing load. In this clinic, higher utilization can lift profit fast, but billing friction and added payroll can pull it back just as fast.
| Scenario | Low CaseLean launch | Base CaseStaffed ramp | High CaseHigh utilization |
|---|---|---|---|
| Launch model | Owner income stays light because utilization is lower and more time goes to clinical delivery. | Owner income follows the model's Year 1 ramp with steady visits and healthy unit economics. | Owner income climbs when the clinic reaches mature utilization and keeps collection quality high. |
| Typical setup | Fewer collected visits, weaker billing capture, and a tighter staff mix keep operating income below the base path. | At 311 visits per month, $59,075 revenue, 770% contribution margin, and $9,550 fixed overhead, operating profit is about $20,854 per month before taxes, reserves, debt, and added payroll. | At 1,913 visits per month and $393,525 revenue, the clinic can support strong contribution before fixed overhead, but full staffing load still matters. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | Lower income bandDownside case | $20,854 per monthModelled base | High income bandUpside case |
| Best fit | Use this to stress-test a slow start or weak referral flow. | Use this as the working case for planning pay, cash, and owner draws. | Use this to test upside from dense referrals and strong therapist utilization. |
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Complete Decongestive Therapy Service Porter's Five Forces Analysis
- Complete Decongestive Therapy Service BCG Matrix
- Complete Decongestive Therapy Service Business Model Canvas
- What Are The 5 KPIs For Complete Decongestive Therapy?
- Complete Decongestive Therapy Business Plan Template in Pre-Written Word
- How Increase Profits For Complete Decongestive Therapy Service?
- What Are The Operating Costs Of Complete Decongestive Therapy Service?
- Complete Decongestive Therapy Service Startup Costs: $865K Plan
- Complete Decongestive Therapy Financial Model Template in Excel
- How to Open a Complete Decongestive Therapy Service in 3–6 Months
- How To Write A Business Plan For Complete Decongestive Therapy Service?
- Complete Decongestive Therapy Service Marketing Mix
- Complete Decongestive Therapy Service Marketing Plan
- Complete Decongestive Therapy Service Business Proposal
- Complete Decongestive Therapy Service PESTEL Analysis
- Complete Decongestive Therapy Service Pitch Deck Example Editable PPTX
- Complete Decongestive Therapy Service Business SWOT Analysis
- Complete Decongestive Therapy Service Value Proposition Canvas
Frequently Asked Questions
The first-year model shows $59,075/month in service revenue and about $20,854/month in operating profit before taxes, reserves, debt, and any additional staffing If the owner also fills the $115,000 Clinic Director role, that salary is separate compensation Actual take-home depends on collections, payroll, and cash kept in the business