 Time to Open6 monthsSetup window
Time to Open6 monthsSetup windowHow To Open A Concierge Medicine Practice In 3–9 Months

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description

Time to Open6 monthsSetup window  Launch Sequence6 stagesModel design
Launch Sequence6 stagesModel design Key BottleneckMember gapPre-open demand
Key BottleneckMember gapPre-open demand First Revenue StepFounding depositsDeposit collected
First Revenue StepFounding depositsDeposit collected


Key Takeaways
- Legal agreements and HIPAA workflows must be ready first.
- Membership promises must match provider capacity and panel limits.
- Year one marketing budget is $36k with $150 CAC.
- Breakeven lands in Month 6 with $696k cash.
Time to Open6 monthsSetup windowLaunch Sequence6 stagesModel designKey BottleneckMember gapPre-open demandFirst Revenue StepFounding depositsDeposit collectedLaunch timeline
Short web summary of the launch plan; the XLSX export contains the full Gantt chart.
Launch scheduleMonth 1Month 2Month 3Month 4Month 5Month 6Month 7Month 8Month 9Month 10
Legal / Compliance
- Scope care rules
- Draft consent forms
- Review privacy policy
- Bind liability coverage
Membership Model
- Set tier mix
- Price monthly plans
- Define billing rules
- Approve renewal terms
Facility / Telehealth
- Map clinic layout
- Install diagnostic gear
- Set telehealth rooms
- Run security setup
- Post signage
EHR / Payments
- Implement EHR
- Configure portal
- Set scheduling
- Link payments
- Test patient flows
Staffing / Training
- Confirm core staff
- Onboard support roles
- Train care process
- Run mock visits
Patient Enrollment
- Build lead list
- Start outreach
- Book intro calls
- Convert members
- Go-live checklist
- First month review
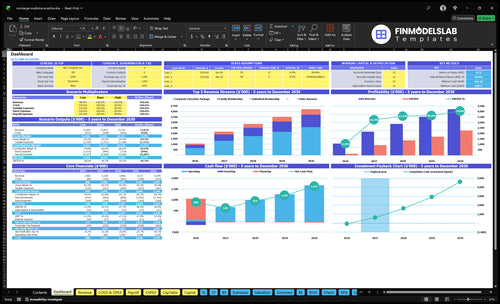
Why test the Concierge Medicine financial model before launch?
The screenshot shows launch timing, member ramp, pricing tiers, staffing schedule, cash runway, and Month 6 break-even path—open the Concierge Medicine Financial Model Template.
Key model highlights
- Overhead: $141k monthly
- Prices: $200/$500/$3,000
- Mix: 45/40/15 split
- Break-even: Month 6
- Cash floor: $696k
- Payback: 15 months
What mistakes create concierge practice launch risks?
In Concierge Medicine, the biggest launch risk is promising more access than the physician and staff can actually deliver. The most common mistakes are weak member acquisition, a vague service scope, unclear Medicare or insurance posture, and untested EHR and portal workflows. That matters because the model shows Month 6 breakeven and a minimum cash need of $696k in Month 6, so delays hit hard.
Launch risks
- Underestimate member acquisition
- Set a vague service scope
- Leave patient agreements weak
- Skip insurance and Medicare clarity
What to test first
- Test onboarding before opening
- Test payment collection flow
- Test appointment flow and capacity
- Test member communication and care protocols
How long to launch concierge medicine?
Concierge Medicine usually takes 3–9 months to launch. A telehealth-light or shared-space setup can fit the short end, while a dedicated clinic with buildout, EHR migration, security setup, and heavier patient conversion pushes you to the long end. The biggest delays are legal review, lease or facility readiness, payment setup, credentialing if insurance applies, patient notice windows, and enrollment lag before go-live.
Fast launch
- 3–4 months for lighter setups
- Use telehealth or shared space
- EHR work often starts Month 1 to Month 3
- Payment and legal setup come first
Longer launch
- 6–9 months with a clinic buildout
- IT setup often runs Month 2 to Month 4
- Security setup often runs Month 3 to Month 5
- Signage often runs Month 4 to Month 6
How to get first concierge medicine patients?
Start with compliant outreach to any existing patient panel, then move to a waitlist, referrals, employer and executive channels, and local education; for launch cost context, see What Is The Estimated Cost To Launch Your Concierge Medicine Business?. In year 1, a $36k marketing budget and $150 modeled CAC mean the bottleneck is trust-based conversion, not ad volume. First revenue should come from founding member deposits or first recurring fees, after signed agreements and working onboarding and payment workflows are in place.
Best first channels
- Reach existing patients compliantly first
- Build a waitlist next
- Use referral relationships
- Target employers and executives
Launch readiness check
- Get signed agreements in place
- Set up onboarding workflows
- Set up payment workflows
- Do not overpromise access or outcomes
Validate readiness before accepting concierge medicine members
Launch readiness checklist
Use this go-live approval checklist to confirm the practice is ready before opening.
Compliance
- State license verifiedCritical
The physician must be licensed before any patient care starts.
- Malpractice policy boundCritical
Coverage should be active before the first visit or consult.
- Patient agreements signedHigh
Unsigned terms can delay billing, access, and service delivery.
- HIPAA workflow testedCritical
Protected health data needs a working privacy workflow on day one.
Clinical setup
- EHR configuredCritical
Charts, notes, and orders must work before the first patient.
- Telehealth link testedHigh
Virtual visits need a clean connection before any remote care.
- Diagnostic tools calibratedHigh
Bad readings create clinical risk and rework during visits.
- Security controls liveCritical
Access controls and backups should protect patient records at launch.
Revenue systems
- Membership pricing loadedHigh
Plans and monthly fees must match the model before sign-up starts.
- Autopay testedCritical
Recurring fees need to collect cleanly or cash flow will slip.
- Insurance billing stance setHigh
The team needs one clear stance on insurance and Medicare billing.
- Receipt workflow testedMedium
Patients should get accurate receipts and fee records without manual fixes.
Staffing
- Physician coverage assignedCritical
Each patient promise depends on a named physician owner.
- Nurse practitioner coverage assignedHigh
Clinical access can slip fast if advanced care support is missing.
- Medical assistant coverage assignedHigh
Frontline support keeps visits, intake, and rooming on time.
- Office manager coverage assignedHigh
Billing, scheduling, and follow-up need one clear owner.
- Backfill schedule setMedium
Absences should not break patient access or same-day response times.
Onboarding
- Offer language approvedCritical
Prospects need clear terms on access, fees, and what is included.
- Intake script testedHigh
A weak intake flow can slow enrollment and create bad first calls.
- Access promise clearCritical
Members must know response times and visit access before they join.
- First consult slots openHigh
If no slots are open, the first revenue step stalls at sign-up.
- Referral path readyMedium
Referral routing keeps care moving when a case needs outside support.
Finance
- Cash runway confirmedCritical
Launch cash must cover setup, payroll, and the first revenue lag.
- Marketing budget loadedHigh
The first-year spend needs to match the acquisition plan.
- CAC target reviewedHigh
Acquisition cost must fit the membership price and payback window.
- Go-live signoff completeCritical
This signoff should confirm compliance, systems, staffing, and payments.
Want the main concierge medicine launch drivers?
1Compliance
GateCounsel-reviewed agreements and HIPAA workflows must be ready before memberships can sell.
2Membership Model
45/40/15Clear member benefits and panel limits have to match provider time, or scheduling gets overloaded.
3Patient Flow
$150 CACSigned interest and compliant outreach are the fastest path to first recurring fees.
4Clinical Ops
4 systemsEHR, portal, telehealth, and payment flows must work together before day one.
5Staffing
CoverageVisit, call, and follow-up coverage has to match the premium access promise.
6Runway
Month 6Month 6 breakeven and $696K minimum cash mean a slower ramp can strain launch.
Compliance And Contracting
Compliance and Contracting
Concierge medicine cannot open cleanly until the legal setup matches the care model. If patient agreements, HIPAA workflows, malpractice coverage, entity setup, and state medical rules are still unclear, you can’t enroll safely or explain the offer clearly on day one. That delays opening and creates avoidable patient confusion around what is included, what is billed, and how notices are handled.
The readiness signal is counsel-reviewed agreements with documented privacy steps before the first member signs. Get the membership terms, cancellation rules, included and excluded services, billing treatment, and Medicare or insurance posture locked first, so the launch doesn’t force a contract rewrite after sales start.
Lock the legal package first
Build the contract stack before any sales push. Define membership terms, cancellation rules, included services, excluded services, billing treatment, and patient notices, then check them against state medical rules and the entity setup. If the care model changes after forms go out, onboarding slows and the first patient experience gets messy.
Assign one owner to collect legal review, malpractice coverage confirmation, and HIPAA documentation. Here’s the quick test: if staff can’t explain what a member gets, what costs extra, and how privacy works in one clear pass, the launch is not ready.
- Counsel reviews all agreements
- Document HIPAA workflow steps
- Confirm malpractice coverage scope
- Check state medical rules
- Set Medicare and insurance posture
1
Membership Model And Care Offering
Lock the Care Menu
If the membership promise is vague, opening slips. Concierge medicine only works when visit availability, after-hours rules, family coverage, and panel limits are set before sales, because staff must explain exactly what a member gets on day one. The Year 1 price mix is 45% individual at $200, 40% family at $500, and 15% corporate executive at $3,000.
Pre-Sell Only What Staff Can Deliver
Build the service menu from real capacity, not wishful demand. Define who handles care coordination, what counts as same-day versus next-day, how messages get answered, and whether executive packages add extra access. That mix prices to a $740 weighted monthly fee, so weak scope control can overload scheduling fast and hurt the first member experience.
2
Patient Acquisition And Conversion
Signed Leads Beat Awareness
For a concierge medicine launch, patient acquisition matters because day-one revenue depends on signed member interest, not just attention. With a $36k Year 1 marketing budget and modeled $150 CAC, the plan supports about 240 member starts if conversion holds. If outreach is not compliant or payment setup is missing, interest stalls and the practice opens with empty onboarding slots.
The realistic sources are existing patient relationships, waitlists, local referrals, employer channels, executive networks, and pre-launch education. Those channels are more likely to produce recurring fees or founding deposits before the first visit. One clean rule: no script, no charge, no enrollments.
Build the Enrollment Path First
Before opening, verify the full path from first contact to paid member: compliant outreach scripts, payment setup, and defined onboarding slots. If the team cannot book, bill, and welcome a member in the same flow, the launch slips from a revenue event into a waiting list. That hurts cash timing and day-one staffing plans.
- Match leads to realistic channels.
- Test paid signup before launch.
- Reserve onboarding capacity early.
- Track deposits, not clicks.
What this hides: awareness alone does not fill a premium panel. The bottleneck is not attention; it is conversion speed from interest to payment, then to a booked onboarding slot. Tight execution here brings in first revenue faster through founding deposits or monthly membership fees.
3
Clinical Operations And Technology
Day-One Clinical Stack
This launch driver determines whether members can book, be seen, pay, and get follow-up on day one. Concierge medicine needs one connected flow for electronic health record (EHR), scheduling, patient portal, payment collection, telehealth, labs and referrals, documentation, messaging, security, and onboarding.
The budget and timing are tight: $45k for EHR implementation in Months 1-3, $12k for telemedicine in Months 1-3, $8k for scheduling software in Months 2-4, and $15k for security systems in Months 3-5. The readiness signal is a tested intake-to-visit-to-payment flow; if systems are disconnected, the team falls back to manual work and launch slips.
Test the Full Patient Path
Map one clean path from inquiry to cash: intake, scheduling, visit, lab order, referral, message, and payment. Then assign one owner for each handoff and test it before go-live. That keeps the first patient from becoming the system test case.
Verify three things before opening: data moves once, staff can finish tasks without rekeying, and patients can complete onboarding without help. Also confirm privacy and security setup are live before enrollment starts, not after. A slow or broken handoff here hurts access, billing, and the first-day patient experience.
- Test booking through payment.
- Confirm telehealth links work.
- Check lab and referral routing.
- Train staff on message rules.
4
Staffing And Provider Capacity
Provider Capacity Match
This launch driver decides whether the practice can open on time without overpromising. A concierge model needs enough physician, nurse practitioner, medical assistant, front desk, billing, and care coordination coverage to support same-day visits, calls, onboarding, referrals, follow-ups, and after-hours rules. If the schedule only works on paper, day-one demand will hit capacity fast and service quality slips.
The Year 1 plan includes 10 primary care physicians, 10 nurse practitioners, 10 medical assistants, and 10 office manager and billing specialist roles; the marketing and business development manager starts in Month 13. Readiness means every promised touchpoint has a real owner and a booked time slot. Here’s the quick test: can the team cover each member contact without stacking work into one person’s day?
Map Promise to Schedule
Before opening, tie each service promise to a role, shift, and response window. The readiness signal is schedule coverage for visits, calls, onboarding, referrals, and follow-ups, plus written rules for nights and weekends. If any piece is uncovered, narrow the offer or delay sales. Selling a premium access model with standard clinic capacity creates backlogs fast.
- Assign each service to one role.
- Block time for calls and follow-ups.
- Write after-hours response rules.
- Test onboarding and referral handoffs.
- Hold sales until coverage is real.
What this estimate hides is how fast support work grows when members expect personal access. If coverage is thin, the first problem is not revenue, it’s missed calls, delayed visits, and a weaker member experience from day one.
5
Revenue Ramp And Cash Runway
Revenue Ramp And Cash Runway
Opening risk here is simple: if member sign-ups lag, cash can go negative before the panel fills. The plan depends on a 45% individual mix at $200, 40% family at $500, and 15% corporate at $3,000, for a weighted fee of about $740 per month. With 17% variable load and $141k of fixed facility and admin overhead before wages, the ramp has to start on schedule.
Here’s the quick math: fixed overhead alone implies about $170k of monthly revenue before wages because $141k ÷ 0.83 is roughly $170k. The model says breakeven lands in Month 6, minimum cash hits $696k in Month 6, and payback takes 15 months. If enrollment slips, the cash trough moves out fast and full staffing becomes risky.
Validate Ramp Before Opening
Build the launch plan from signed member interest, not hopeful demand. Lock the service mix, payment setup, and provider schedule first, then test whether the team can actually onboard into the Month 1 to Month 6 ramp. The launch is ready when care slots, billing flow, and staffing can absorb the modeled mix without promising more access than the panel can serve.
- Track deposits by member type.
- Match visit slots to capacity.
- Model cash through Month 6.
- Delay hires if enrollment slips.
What this estimate hides is wage pressure, since the $141k overhead is before wages. If onboarding takes longer than planned or the corporate mix comes in lighter than 15%, revenue falls below the model and runway tightens before the practice is stable.
6
Related Products
- Concierge Medicine Porter's Five Forces Analysis
- Concierge Medicine BCG Matrix
- Concierge Medicine Business Model Canvas
- 7 Critical KPIs to Track for Concierge Medicine Success
- Concierge Medicine Business Plan Template in Pre-Written Word
- How to Boost Concierge Medicine Profitability with 7 Key Strategies
- How Much Does It Cost to Run Concierge Medicine Monthly?
- Concierge Medicine Startup Costs: $166K CAPEX Plus $696K Cash
- Concierge Medicine Financial Model Template in Excel
- How Much Concierge Medicine Owners Make: $368K-$249M
- How to Write a Concierge Medicine Business Plan in 7 Essential Steps
- Concierge Medicine Marketing Mix
- Concierge Medicine Marketing Plan
- Concierge Medicine Business Proposal
- Concierge Medicine PESTEL Analysis
- Concierge Medicine Pitch Deck Example Editable PPTX
- Concierge Medicine Business SWOT Analysis
- Concierge Medicine Value Proposition Canvas
Frequently Asked Questions
Start by defining the membership offer, care scope, legal structure, patient agreements, systems, staffing, and enrollment plan Use a 3–9 month launch window as a planning range In the model, EHR work begins in Month 1, security runs through Month 5, and breakeven is tested in Month 6