 Time to Open8-16 weeksSetup window
Time to Open8-16 weeksSetup windowOpen a Corn and Callus Removal Service in 8 to 16 Weeks

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Time to Open8-16 weeksSetup window  Launch Sequence5 stagesCompliance first
Launch Sequence5 stagesCompliance first Key BottleneckLicense gateState rules
Key BottleneckLicense gateState rules First Revenue StepBooked evalsBooking live
First Revenue StepBooked evalsBooking live


You’re opening a medical foot care service, so launch readiness comes before marketing This guide covers the first operating month through Year 5, with 8 to 16 weeks as the planning window, Year 1 staffing of 1 lead podiatrist, 1 staff podiatrist, 1 junior podiatrist, and 2 podiatry assistants, and a practical next step: validate licensing, room setup, scheduling, and first-patient flow before opening
Time to Open8-16 weeksSetup windowLaunch Sequence5 stagesCompliance firstKey BottleneckLicense gateState rulesFirst Revenue StepBooked evalsBooking liveLaunch timeline
This is a short web summary of the launch plan; the XLSX export holds the detailed Gantt chart.
Launch scheduleWeek 1Week 2Week 3Week 4Week 5Week 6Week 7Week 8Week 9Week 10Week 11Week 12
Legal / compliance
- File entity
- Secure licenses
- Set consent forms
- Draft care policies
Clinic setup
- Plan room layout
- Start renovation
- Install treatment chairs
- Set waiting room
Equipment / supplies
- Order supplies
- Buy sterilizer
- Stock PPE
- Set disinfection flow
Staffing / training
- Confirm hiring plan
- Train intake steps
- Train treatment team
- Run dry cases
Marketing / referrals
- Set pricing
- Build referral list
- Launch outreach
- Open booking channel
Finance / operations
- Build launch budget
- Set billing flow
- Configure scheduling
- Go live review
Why test the launch plan before opening month?
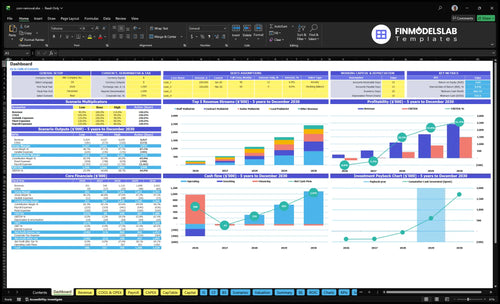
This Corn and Callus Removal Service Financial Model Template shows launch timing, 60% capacity, cash needs, assumptions, and break-even logic—open the model.
Financial model highlights
- Launch timing and ramp
- Pricing from $80-$160
- Hiring and break-even triggers
How long does it take to open a corn removal clinic?
A Corn and Callus Removal Service usually takes 8 to 16 weeks to open. If an existing podiatry office already has the room, instruments, staff, and documentation, it can launch faster. The main delays are lease work, provider licensing, malpractice coverage, sterilization workflow, payer credentialing, and room turnover.
Fast path
- 8 to 16 weeks is the usual range.
- Parallelize room, supplies, and intake setup.
- Use an existing office to move faster.
- Start outreach while forms are built.
Common delays
- Wait on provider licensing.
- Secure malpractice coverage early.
- Finish payer credentialing before billing insurance.
- Fix lease work and room turnover first.
Do you need a license to open a corn removal service?
Yes, a Corn and Callus Removal Service needs the right medical license when it diagnoses, debrides, or treats painful corns and calluses; state scope-of-practice rules decide whether that must be a licensed podiatrist or another legally permitted provider. Cosmetic foot smoothing is different, so use How Increase Profits For Corn And Callus Removal Service? only after the legal scope, billing, and documentation model is clear.
License Gate
- Check 50-state scope rules first
- Define diagnosis versus cosmetic foot care
- Confirm who can treat lesions
- Document authority before appointment 1
Launch Ready
- Use the correct medical practice structure
- Carry malpractice coverage before marketing
- Write sterile clinical protocols
- Keep compliant records for 100% of visits
What mistakes should you avoid when opening a corn removal service?
Avoid opening the Corn and Callus Removal Service before you’ve locked down scope, sterilization, and the front-desk flow; the biggest launch mistakes are unclear scope of practice, weak sterilization, missing consent and intake forms, and no referral pipeline. You’re serving people with painful foot problems, so if scheduling or intake runs slow, capacity and patient experience drop fast, and readiness beats speed.
Clinical setup
- Define scope of practice early
- Test sterilization every visit
- Use consent forms before care
- Keep clinical notes complete
Front desk flow
- Mock appointments before launch
- Check scheduling and billing
- Confirm eligibility and collections
- Set follow-up scripts and referral paths
Confirm what must be ready before the first patient appointment
Launch readiness checklist
Use this go-live approval checklist to confirm the clinic is ready before opening.
Licensing
- State license and scope confirmedCritical
State podiatry license and scope limits must be clear before any treatment.
- Medical entity structure setHigh
The clinic needs a legal home before contracts and billing start.
- Malpractice and HIPAA boundCritical
Coverage and privacy rules must be active before first patient contact.
Clinic setup
- Treatment chairs installedHigh
Patients need usable chairs before booking opens.
- Sterilizer passed test cycleCritical
Sterilization failures can stop launch fast.
- Sharps and disinfection readyCritical
Clean handling keeps room turnover safe and consistent.
Intake
- Consent forms signed offCritical
Consent protects the clinic and the patient.
- Intake forms capture risk historyHigh
Foot health, meds, and risk history shape safe treatment.
- Charting workflow testedHigh
Notes must be complete before billing and follow-up.
Staffing
- Year one roster matches planCritical
The launch model needs 1 lead, 1 staff, 1 junior, 2 assistants.
- Credentialing and onboarding completeHigh
Untested staff can delay launch and create risk.
- Coverage fits 60% capacityHigh
Year 1 assumes 60% capacity, so coverage must match demand.
Booking
- Booking flow accepted test appointmentsCritical
Patients need a working path to book without friction.
- Pricing sheet covers $80-$160Critical
Prices must stay inside the model range to protect margin.
- Payment processing and billing testedCritical
Cash collection and claims can't wait until after opening.
Go-live
- Referral outreach list is readyHigh
Referrals can fill the first appointment book faster than ads.
- Local search profile is liveHigh
Local search helps nearby patients find the clinic.
- Runway and signoff approvedCritical
The model shows month 24 minimum cash and month 14 breakeven.
Want to see the six drivers that decide launch readiness?
1Licensing Scope
License gateExpect 8-16 weeks to clear scope, entity, and coverage before promotion.
2Treatment Room
Sterile roomA ready room and clean tool flow reduce idle time and protect patient safety.
3Staffing Workflow
5 rolesFive starting clinical roles need tested handoffs so admin work doesn't steal chair time.
4Payer Readiness
$80-$160Prices run $80-$160, so billing rules and documentation must work before first appointments.
5Local Demand
Inquiry flowLocal search and referrals must fill the book to reach 60% Year 1 use.
6Capacity Follow-Up
60%-90%Book follow-ups before patients leave, or full calendars will cap growth before 90% use.
Licensing and Scope Readiness
Licensing and Scope Readiness
This is the gate for opening on time. Before you book the first corns and calluses visit, confirm who in the target state can legally diagnose, treat, and remove corns and calluses. If you market a medical service before scope is clear, you can stall launch, change the service model, and delay first revenue.
The setup has to match the care model: medical entity setup, malpractice coverage, supervision rules, and documentation. Even the Year 1 staffing plan of 1 lead podiatrist, 1 staff podiatrist, 1 junior podiatrist, and 2 assistants depends on the licensed role being clear first. No scope clarity, no safe opening.
Verify scope before promotion
Start with one written scope decision and use it across licensing, insurance, and records. That keeps the treatment plan, consent forms, and supervision lines aligned before the first appointment. If the provider cannot legally do the work, every booked slot becomes rework.
- Confirm state scope rules first.
- Attach a licensed provider before ads.
- Match entity, coverage, and supervision.
- Test intake, consent, charting, payment.
Run a dry test from intake to chart to payment before you advertise. The go/no-go line is simple: the service needs a licensed clinician, the right coverage, and the right records on day one.
1
Treatment Room and Sterilization Setup
Treatment Room and Sterilization Setup
A callus removal clinic cannot open safely if the room is not ready before the first appointment. The core setup is the treatment chair, podiatry instruments, PPE, sharps disposal, disinfection, sterilization, supply inventory, and room turnover steps. The readiness signal is a documented instrument flow from use → cleaning → storage.
When this step slips, the bottleneck is idle provider time because the room or tools are not ready. That slows day-one capacity and raises patient safety risk. For a service built on immediate relief, a clean, fully stocked room is not optional; it is the opening gate.
Verify room flow before booking visits
Map the full turn process before launch: set the chair, stage instruments, stock PPE and sharps containers, and test disinfection and sterilization steps. Then run one full room turnover with a checklist so the team can prove the space resets fast and in the same order every time.
- Confirm treatment chair placement
- Count clean instruments daily
- Separate dirty and sterile items
- Test sharps disposal access
- Set minimum supply par levels
- Document room reset ownership
If turnover is not standard, the clinic can open with staff waiting on tools instead of treating patients. That hurts the first-day schedule, slows revenue from day one, and creates avoidable safety and compliance gaps. A simple written flow is the fix.
2
Provider Staffing and Appointment Workflow
Provider Staffing and Workflow
This launch gate decides whether the clinic can see patients on day one. With 1 lead podiatrist, 1 staff podiatrist, 1 junior podiatrist, and 2 podiatry assistants, the schedule has to cover intake, treatment, charting, room turnover, follow-up booking, and patient education without pulling the provider into admin work.
At the stated assumptions of 80, 70, 60, and 40 monthly treatments by role type, Year 1 capacity is about 290 treatments per month. If the handoff between front desk, assistant, and provider is weak, the clinic opens with slow visits, delayed follow-ups, and lost chair time even when staffing is in place.
Test the day-one handoff
Before opening, run one full patient flow from booking to checkout and confirm who does each step. The goal is a clean handoff where the front desk, assistant, and provider each know their part and the podiatrist stays on clinical work.
Map intake to checkout.
Assign charting before launch.
Book follow-ups before discharge.
Time one mock visit end to end.
3
Payer, Pricing, and Documentation Readiness
Payer, Pricing, and Documentation
Opening on time depends on picking the cash-pay, insurance-based, or hybrid model before the first visit. If insurance is central, credentialing and claim setup can slow launch, so the clinic needs a clear path for eligibility checks, coding support, consent, collections, and claim timing before it books patients. The day-one test is simple: a full visit that moves from scheduling to payment or claim submission without a break.
Pricing also has to match the service mix. Year 1 assumptions run from $80 for assistant-supported treatments to $160 for lead podiatrist treatments, so billing rules, visit notes, and payment steps must be set for each visit type. If documentation is weak, cash can stall, claims can reject, and staff will spend clinic time fixing paperwork instead of treating patients.
Set the billing path first
Before opening, lock the payer model, then build the workflow around it. Confirm what each visit type needs for eligibility, consent, coding, and collection, and make sure the front desk and clinical team use the same script and forms. One clean test visit should show the full path from booking to paid-in-full or submitted claim.
- Choose cash-pay, insurance, or hybrid.
- Map $80 to $160 visit types.
- Verify coding and note templates.
- Test collections before first appointments.
- Block launch until claim timing works.
If the service depends on insurance, do not promote start dates until credentialing is done or the cash-pay fallback is ready. That keeps first-day operations clean and avoids opening with patients, staff, and revenue all waiting on unfinished billing work.
4
Referral and Local Demand Activation
Local Demand and Referrals
Opening a corn and callus clinic with treatment rooms ready but no bookings is a launch risk, not a sales problem. The first appointments depend on local demand channels that turn searches and referrals into evaluations, so the clinic needs live local SEO, service pages, reviews, and a Google Business Profile before day one.
The referral side matters just as much. Target primary care offices, diabetes educators, senior communities, assisted living contacts, and other foot-care referral sources so inquiries can convert into booked visits. The readiness signal is a working inquiry-to-appointment workflow; without it, the clinic can open on time and still sit below the Year 1 60% utilization goal.
Build the booking path first
Before opening, verify that every lead source lands in one clear path: search, call, text, or referral request to scheduled evaluation. Set up service pages for the treatment, collect reviews early, and make sure the front desk can book fast and track source by channel. That is what turns local demand into revenue-ready visits.
Document the handoff from referral to appointment, then test it with a live inquiry. If staff can’t answer, book, and confirm without delay, the clinic risks opening with empty capacity and weak early cash flow. One clean booking process is better than five marketing ideas that don’t convert.
- Publish local service pages.
- Complete Google Business Profile.
- Collect early patient reviews.
- Track every inquiry source.
- Test referral-to-booking handoff.
5
Capacity Planning and Follow-Up Retention
Capacity Planning and Follow-Up Retention
Opening on time depends on knowing how many visits each clinician can handle and how fast patients come back. Year 1 capacity is 80 monthly treatments for the lead podiatrist, 70 for a staff podiatrist, 60 for a junior podiatrist, and 40 per podiatry assistant, or 250 planned treatments across the core team. The readiness check is simple: follow-up booking before the patient leaves.
If repeat care is not booked on the spot, calendars can swing from open to full with no room for extra hours or added assistant support. Capacity is expected to rise from 60% in Year 1 to 90% in Year 5, so the clinic needs a clear rebook rule, a live provider calendar, and a tight handoff that protects treatment time.
Test the rebook flow before day one
Map one full visit from check-in to discharge and confirm the next appointment is set before the patient walks out. Verify who handles scheduling, who watches provider load, and how assistant support covers turnover gaps. That keeps first-month capacity real and lowers the risk of opening with a schedule that looks busy but cannot absorb demand.
- Set monthly slot targets by role.
- Book follow-ups before checkout.
- Test assistant coverage for turnover.
- Watch for full calendars early.
6
Related Products
- Corn and Callus Removal Service Porter's Five Forces Analysis
- Corn and Callus Removal Service BCG Matrix
- Corn and Callus Removal Service Business Model Canvas
- What Are 5 KPIs For Corn And Callus Removal Service Business?
- Corn And Callus Removal Service Business Plan Template in Pre-Written Word
- How Increase Profits For Corn And Callus Removal Service?
- What Are Operating Costs For Corn And Callus Removal Service?
- Corn and Callus Removal Service Startup Costs: $537K Plan
- Corn and Callus Removal Financial Model Template in Excel
- How Much Corn And Callus Removal Owners Make: -$123K To $101M
- How To Write A Business Plan For Corn And Callus Removal Service?
- Corn and Callus Removal Service Marketing Mix
- Corn and Callus Removal Service Marketing Plan
- Corn and Callus Removal Service Business Proposal
- Corn and Callus Removal Service PESTEL Analysis
- Corn and Callus Removal Service Pitch Deck Example Editable PPTX
- Corn and Callus Removal Service Business SWOT Analysis
- Corn and Callus Removal Service Value Proposition Canvas
Frequently Asked Questions
It can be mobile only if state scope rules, malpractice coverage, infection control, documentation, and equipment transport support it A clinic is usually easier to control because sterilization, sharps handling, treatment chair setup, and room turnover stay in one place If mobile visits slow provider flow, the Year 1 60% capacity target may be harder to reach