 Owner income$12.5k
Owner income$12.5kHow Much Corporate Health Screening Owners Make At $123M Year 1 Revenue

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$12.5k  Net margin85%→88%
Net margin85%→88% Revenue for target pay≈$37.3k
Revenue for target pay≈$37.3k Business difficultyMedium
Business difficultyMedium


You’re selling employer-paid screenings before owner pay feels safe, so the key question is cash left after clinical labor, supplies, overhead, reserves, and your own role This first-year planning model shows $123M in revenue, 85% gross margin, $628k operating profit before taxes and reserves, and a $150k CEO salary assumption It excludes income taxes, financing terms, legal compliance costs beyond listed software and professional fees, and any guaranteed medical reimbursement assumptions
Owner income$12.5kNet margin85%→88%Revenue for target pay≈$37.3kBusiness difficultyMediumWant to test your owner income?
Owner income calculator
Estimate owner take-home and target-pay gap from revenue, gross margin, operating costs, reserves, and target pay.
Planning note: This is a researched planning estimate only. It is not guaranteed salary, tax advice, or owner distribution advice.
Want to check owner income in the model?
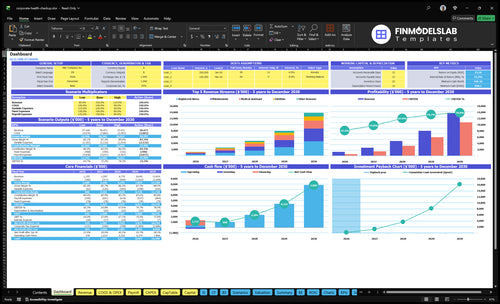
The Corporate Health Screening Financial Model Template dashboard shows revenue, gross margin, operating profit, cash flow, and owner income. Charts compare Year 1 $123M, Year 3 $478M, and mature-year $1,382M revenue. Open it.
Owner-income model highlights
- $150k CEO salary
- Profit before reserves
- Distributions after reserves
- Staff, treatments, pricing inputs
- COGS, overhead, payroll inputs
- Employee-count revenue logic
What is the profit margin for a corporate health screening business?
Corporate Health Screening can show an 85% gross margin in Year 1 and 88% in a mature year, but that is before overhead and owner pay. If you're sizing startup costs, see What Is The Estimated Cost To Open And Launch Your Corporate Health Screening Business? The real profit squeeze is the $6,500 monthly overhead and $280k Year 1 payroll.
Year 1 margin math
- 8% medical supplies
- 7% practitioner wages
- 85% gross margin
- 5% tech and sales costs
What cuts profit fast
- $6,500 monthly overhead
- $280k Year 1 payroll
- Lab panels raise direct costs
- No-shows and travel hurt margin
How much revenue does a corporate health screening contract generate?
For Corporate Health Screening, revenue per contract isn’t a fixed number; it depends on how many employees are screened, the package price, minimum event fees, add-on tests, repeat annual screenings, and multi-location rollout. Here’s the quick math: Year 1 average billed service price is about $102, based on $102,735 monthly revenue and 1,011 billable services. So a 100-service event would model about $10,200 in revenue before direct costs if all 100 services are billable.
What drives contract value
- Employees screened sets volume
- Package price sets base revenue
- Minimum event fees protect small jobs
- Annual repeats raise lifetime value
What can raise or cut margin
- Add-on tests lift revenue
- Lab costs can rise with add-ons
- Compliance adds process cost
- Staffing limits event capacity
Can a corporate health screening business scale?
Yes—Corporate Health Screening can scale, but the model shifts from hands-on events to staffing, sales, scheduling reliability, and quality control. In the plan, clinical and advisory staff rise from 9 in Year 1 to 54 at maturity, revenue climbs from $123M to $1,382M, and capacity improves from about 55% to 65% in Year 1 toward 85% to 88% later. Admin payroll also grows from $280k to $620k, so compliance, missed events, clinician availability, data handling, employer billing delays, and thin reserves are the real pressure points.
Scale drivers
- 9 staff in Year 1
- 54 staff at maturity
- $123M to $1,382M revenue
- 55% to 85%+ capacity
Key risks
- Compliance can slow growth
- Missed events hit revenue fast
- Clinician availability limits capacity
- Billing delays strain cash flow
Want the six main income drivers?
1
840/moEmployer Volume
More employer contracts add billable screenings fast, and the model counts billable services, not unique employees, so volume drives the whole income line.
2
65%-88%Event Size
Bigger on-site events spread setup and labor across more screenings, so each contract earns more without a matching jump in fixed cost.
3
$102Price Mix
A higher share of nurse and dietitian screenings lifts the Year 1 average billed price and pushes revenue up per visit.
4
85%Direct Costs
Clinical supplies and practitioner wages eat into gross margin, which starts near 85%, so small cost swings flow straight to owner take-home.
5
$150KStaffing Model
The mix of salaried staff, including the $150k CEO role, decides how much revenue stays after payroll and how much can reach the owner.
6
$6.5K/moOverhead Buffer
Fixed overhead runs about $6,500 a month, and the $848k minimum cash need in Month 2 shows how much cushion you need before payouts stay safe.
Corporate Health Screening Core Six Income Drivers
Employer contract volume
Employer contract volume
More employer contracts mean steadier screening volume, and that matters because the model needs 1,011 billable services per month in Year 1. If renewals are weak, clinical staff sit idle and the $6,500 monthly fixed overhead comes out of a thinner margin, which cuts owner pay. One gap in contracts can turn a full calendar into a cash squeeze.
Track employers served, renewal frequency, minimum event fees, and employer size. Bigger accounts can improve route planning, but they also raise scheduling, reporting, and service-level risk, so a few large clients should not replace a balanced book. Predictable contracts are what keep staffing clean and cash flow steady.
Keep the contract book full
Forecast by employer, not just by screening count. Build a pipeline that covers the gap to 1,011 monthly billable services, then test how many services each contract contributes at its minimum fee and renewal rate. One line that matters: if renewals fall, income falls fast.
- Contracts active
- Renewal rate
- Services per employer
- Scheduled event count
Use those four numbers to match staffing to demand. That keeps the owner paid from repeat volume instead of one-off spikes, and it helps spot when a large account is adding profit versus just adding stress.
1
Employees screened per event
Employees Screened per Event
This driver is the number of employees who actually complete screening at one onsite event. The inputs are registered employees, participation rate, completed screenings, and no-show rate. If turnout is thin, the same travel, setup, staffing, supplies, and admin time gets spread over fewer billed services, so owner income drops even when the client looks good on paper.
Here’s the quick math: the model needs about 1,011 monthly billable services in Year 1, and break-even is about 367 billable screenings per month if one screening equals one billed employee service. Below that, fixed work starts eating margin fast. More screenings per event push more cash to owner pay; low turnout can turn a profitable employer into a busy, low-margin account.
Track Turnout Before You Staff
Track turnout by event, not just by client. Compare registered employees vs. completed screenings, then watch the no-show rate and participation rate by site, shift, and reminder method. If a site stays below the level needed to spread setup and travel costs, raise minimums or reschedule.
Use a simple gate: only confirm events that can clear the revenue needed for the day’s labor and travel. One clean rule: more screened employees per stop means better gross margin and steadier owner draw. What this estimate hides is staffing mix; if the team is overbooked or underbooked, cash flow gets choppy even when monthly volume looks fine.
2
Price and package mix
Price and package mix
Price is a direct income lever because every billed screening changes revenue and margin. In Year 1, service prices range from $75 for phlebotomist services to $180 for dietitian services, with a weighted average billed service price of about $102. If volume holds at 1,011 billable services a month, that mix implies about $103,122 in monthly revenue before direct costs.
Higher-value packages can lift take-home income, but they also bring lab fees, staff credential needs, data work, and employer approval steps. A richer package only helps if the added price beats the added cost. Here’s the quick math: the same 1,011 services would produce about $75,825 at $75 pricing or $181,980 at $180 pricing, so mix has a big effect on cash flow.
Track price by service line
Measure service mix, gross margin, and approval time for each package. Track how many jobs are billed at $75, $102, and $180, plus add-ons like biometrics, blood panels, flu shots, coaching, or reporting. One clean rule: if a package adds work but not margin, don’t expand it.
Test pricing against employer willingness to pay and the real cost to deliver. Watch these inputs each month:
- Price per billed service
- Direct cost per package
- Add-on attach rate
- Employer approval cycle
- Revenue per event
If the higher-price mix slows approvals, cash can lag even when revenue looks strong.
3
Direct clinical and lab costs
Direct clinical and lab cost control
Direct costs set gross margin before overhead and owner pay. In Year 1, this model assumes 15% total COGS: 8% medical supplies and consumables plus 7% practitioner hourly wages. If mature-year direct costs fall to 12%, every $100 of service revenue keeps $3 more for fixed overhead, debt, and owner draw.
What moves this line: lab fees, licensed nurse time, phlebotomy supplies, PPE, equipment depreciation, and travel. The inputs are billable screenings, event mix, staff hours, and supply use. Here’s the quick math: if direct cost rises from 15% to 18%, gross margin drops by 3 points. Don’t cut medically necessary steps or compliance-driven quality controls.
Track cost per screening
Measure direct cost per event and per billed screening, not just monthly spend. Use a simple check: supplies, lab fees, clinical wages, travel, and depreciation divided by completed screenings. If a site has weak turnout, the same travel and setup cost hits each screening harder, so owner income falls even when revenue looks fine.
- Track cost per completed screening.
- Schedule fuller events and routes.
- Watch lab and travel spikes.
- Keep required clinical steps intact.
Control waste in inventory and scheduling, and match staff to booked volume. If practitioner idle time stays high, gross margin gets squeezed fast. The goal is lower cost per service, not lower care quality, because owner pay depends on what’s left after direct clinical and lab spend.
4
Staffing model and owner involvement
Owner Involvement and Staffing Load
Owner-run delivery can lift early cash flow because the founder can skip some admin and event labor, but it also steals time from selling and closing contracts. In Year 1, the model already carries $150k CEO pay, $85k operations manager pay, and a $90k sales director at 0.5 FTE. If the founder also sells, coordinates, bills, and works events, burnout risk rises and owner take-home income gets capped.
Clinical capacity depends on registered nurses, phlebotomists, medical assistants, dietitians, and health coaches. Hiring more of them improves coverage and service quality, but it also adds payroll risk. The key inputs are billable screenings, staff hours, owner hours, and utilization. If labor grows faster than monthly services, profit slips before the owner can pay themselves well.
Track Owner Hours Before You Hire
Measure billable services per staff hour, owner sales hours, and event hours each month. The goal is simple: keep the founder focused on sales and keep clinical work on scheduled staff. If owner time is buried in billing or setup, the business may look busy but still miss cash flow targets.
- Track screenings per event
- Watch owner non-sales hours
- Cap overtime before hiring
- Match staffing to booked volume
5
Overhead, sales expense, and reserves
Overhead, sales expense, and reserves
Even with strong gross margin, this business still gives up cash to $6,500 per month in fixed overhead: rent, general liability insurance, compliance software, accounting and legal fees, utilities, and website costs. Add 3% technology fees and 2% sales commissions, and owner pay comes after those layers, not before.
Here’s the quick math: operating profit is not fully spendable income. If you pull distributions before reserves, you can miss equipment replacement, billing delays, proposal work, travel, and compliance support costs that show up in cash, not just in the P&L.
Track reserves before owner draws
Measure monthly overhead, tech fees, commissions, and reserve needs separately. One clean rule: set aside cash before distributions.
- Track fixed overhead at $6,500.
- Track variable sales costs at 5%.
- Hold cash for billing delays.
- Hold cash for equipment replacement.
- Keep compliance support funded.
If owner draws follow reserves, take-home pay stays tied to actual cash, not just reported profit.
6
Compare lean, base, and high owner-income scenarios
Owner income scenarios
Owner income rises as staffing fills up and employer accounts get bigger. Utilization, compliance, and payroll timing drive the gap between a lean launch and a scaled model.
| Scenario | Low CaseFounder-led | Base CaseManaged team | High CaseScaled employer model |
|---|---|---|---|
| Launch model | A founder-led launch keeps income tied to early client volume and tight staffing. | A managed team model supports steady employer demand and more predictable owner income. | A scaled employer-account model lifts owner income fast, but only if staffing and utilization stay tight. |
| Typical setup | Year 1 style setup runs about $1.23M revenue at 85% gross margin with $280k payroll, $78k fixed overhead, a $150k CEO salary, and about $628k operating profit before taxes and reserves. | Year 3 style setup reaches about $4.78M revenue at 86.5% gross margin with $460k payroll and about $3.339M operating profit before taxes and reserves. | Mature-year setup reaches about $13.82M revenue at 88% gross margin with $620k payroll and about $11.102M operating profit before taxes and reserves. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $628kFounder-led income | $3.339MManaged team income | $11.102MScaled income model |
| Best fit | Use this as a downside check when the owner still handles sales, scheduling, and delivery. | Use this for a normal operating plan with a staffed sales process and repeat client flow. | Use this to test upside when the business wins larger employer contracts and keeps service lines full. |
Planning note: These ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Corporate Health Screening Porter's Five Forces Analysis
- Corporate Health Screening BCG Matrix
- Corporate Health Screening Business Model Canvas
- 7 Critical KPIs for Corporate Health Screening Success
- Corporate Health Screening Business Plan Template in Pre-Written Word
- 7 Strategies to Increase Corporate Health Screening Profitability
- How Much Does It Cost To Operate Corporate Health Screening Services?
- Corporate Health Screening Startup Costs With $65K Monthly Overhead
- Corporate Health Screening Financial Model Template in Excel
- How To Open A Corporate Health Screening Business In 8–16 Weeks
- How to Write a Corporate Health Screening Business Plan: 7 Steps
- Corporate Health Screening Marketing Mix
- Corporate Health Screening Marketing Plan
- Corporate Health Screening Business Proposal
- Corporate Health Screening PESTEL Analysis
- Corporate Health Screening Pitch Deck Example Editable PPTX
- Corporate Health Screening Business SWOT Analysis
- Corporate Health Screening Value Proposition Canvas
Frequently Asked Questions
The source model includes a $150k CEO salary and about $628k Year 1 operating profit before taxes and reserves That does not mean the owner should take all cash out A safer view separates salary, reserve funding, equipment needs, billing delays, and any profit distributions approved after the company stays liquid