 Owner income$2.0M-$18.7M
Owner income$2.0M-$18.7MCosmetic Dermatology Clinic Owner Income: $263M Year 1 Model

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$2.0M-$18.7M  Net margin60.5%-79.8%
Net margin60.5%-79.8% Revenue for target pay≈$769K
Revenue for target pay≈$769K Business difficultyMedium
Business difficultyMedium


You’re estimating owner pay from a US cosmetic dermatology clinic, not a guaranteed physician salary This model uses a five-year planning period, starting with $377M Year 1 revenue and modeled operating profit before tax, debt, reserves, and distributions
Owner income$2.0M-$18.7MNet margin60.5%-79.8%Revenue for target pay≈$769KBusiness difficultyMediumWant to test your clinic owner pay?
Owner income calculator
Estimate owner take-home and the target-pay gap from monthly revenue, gross margin, operating costs, reserves, and target owner pay.
Planning note: Research-based planning estimate only. It is not guaranteed salary, tax advice, or owner distribution advice.
Want to check owner income in the full financial model for a Cosmetic Dermatology Clinic?
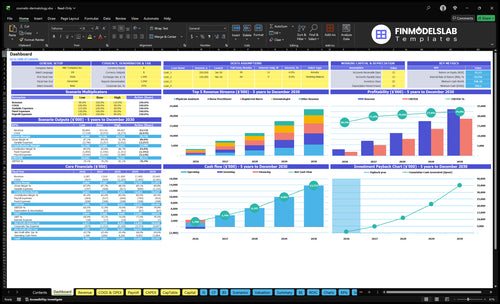
This dashboard shows revenue build-up, margin, costs, reserves, and owner income in the Cosmetic Dermatology Clinic Financial Model Template. Open it to test assumptions.
Owner-income model highlights
- $377M to $2344M revenue
- $263M to $1950M operating profit
- Provider capacity and treatment mix
- Payroll, equipment, operating expenses
- Debt, break-even, owner income
- Low, base, high scenarios
What revenue is needed for cosmetic dermatology clinic owner pay?
For a Cosmetic Dermatology Clinic, the owner pay question starts with monthly cash flow, not annual profit. With an 81% contribution margin, the model says break-even is about $44K in monthly revenue to fund $25K of owner pay before tax and reserves. A safer planning target is about $75K a month, and you should still add debt service and cash reserves before taking distributions.
Quick math
- 81% contribution margin
- $44K monthly break-even
- $25K owner pay goal
- Work backward from cash flow
Cash guardrails
- Add debt service first
- Hold reserves before distributions
- Use monthly revenue, not guesses
- Target about $75K monthly
Is a cosmetic dermatology clinic profitable?
Yes, a Cosmetic Dermatology Clinic can be highly profitable if treatment volume, pricing, and utilization cover overhead; this model shows 826 monthly treatments at a $381 blended ticket, or about $314,706/month and $3.78M/year. For the KPI that matters most, see What Is The Most Important Indicator Of Success For Your Cosmetic Dermatology Clinic?; just note that modeled $2.63M operating profit is before taxes, debt, reserves, and unlisted base clinical payroll, so it isn’t the same as owner cash.
Profit math
- 826 treatments per month
- $381 blended ticket
- $314,706 monthly revenue
- $3.78M Year 1 revenue
Profit caveats
- 19% direct and variable costs
- 81% contribution before fixed overhead
- $2.63M modeled operating profit
- Excludes taxes, debt, reserves, payroll
How does owner involvement change cosmetic dermatology clinic income?
Owner involvement changes Cosmetic Dermatology Clinic income because the owner can earn as a treating clinician, as a manager, or as the lead of a larger platform. In Year 1, the model has 1 dermatologist, 1 physician assistant, 1 nurse practitioner, 2 registered nurses, and 2 medical aestheticians; by Year 5, it scales to 3 dermatologists, 5 physician assistants, 5 nurse practitioners, 6 registered nurses, and 6 medical aestheticians. More providers raise revenue capacity, but they also raise supervision, utilization, payroll, and compliance work.
Owner role
- Treating can drive billable income.
- Managing shifts time away from visits.
- Platform adds oversight burden.
- Income follows provider time use.
Scale mix
- Year 1 has 7 providers total.
- Year 5 has 25 providers total.
- Capacity rises with each added clinician.
- Complexity rises with payroll and compliance.
Want to see the main income drivers?
1
$381Treatment Mix
A $381 blended ticket on each visit pushes more cash to owner take-home before tax and reserves, because higher-value treatments earn more on the same clinic time.
2
45%-60%Provider Utilization
Moving providers from the low end of starting capacity fills paid chair time, so more revenue lands on the same payroll and lease base.
3
826/moPatient Demand
More consults, bookings, and repeat visits lift monthly treatment volume, and that extra volume spreads fixed cost over more billable work.
4
$750Pricing Power
Small rate gains on premium services raise the blended ticket, and even modest price lift shows up fast in owner take-home.
5
13%Supply Costs
Keeping product and device costs near 13% protects gross margin, so more of each treatment survives after clinical inputs.
6
$52K/moFixed Overhead
About $52K a month in rent, staff, software, and admin costs has to be covered first, so tight overhead control protects owner cash.
Cosmetic Dermatology Clinic Core Six Income Drivers
Treatment Mix And Average Ticket
Treatment Mix And Average Ticket
Cosmetic dermatology income depends on what you sell and who delivers it. Year 1 pricing ranges from $150 for medical aesthetician treatments to $650 for dermatologist treatments, and the blended ticket is about $381. Shifting mix toward injectables, laser packages, resurfacing, body contouring, hair restoration, and premium skin care can lift revenue and gross profit if the higher price also covers product cost, provider time, and room use.
Here’s the quick math: more high-ticket visits raise monthly sales, but they don’t help owner pay if margins shrink. The key inputs are treatment count, average ticket, provider type, and service-level cost. What this hides is demand risk: a premium menu only works when patients still book at the higher price and the clinic keeps utilization strong.
Track Mix by Margin
Measure revenue by procedure and provider, not just total visits. Split services into low-ticket and high-ticket buckets, then compare each service’s gross margin after product, staff time, and room time. If the $381 blended ticket rises, watch whether contribution also rises; higher price only helps if added labor and supplies stay in line.
- Track ticket by procedure.
- Track margin by provider.
- Watch room time per visit.
- Test bundles before raising price.
Use this to set the weekly schedule. Fill the highest-margin slots first, then add lower-ticket treatments around them. If demand weakens, don’t chase volume with discounting; protect margin and keep cash available for fixed overhead and owner draws.
1
Provider Utilization
Provider Utilization
Provider utilization is the share of staffed clinical capacity that turns into booked treatments. In year 1, the model assumes 45% utilization for medical aestheticians and 60% for dermatologists, with 826 treatments per month booked across the clinic. Higher utilization lifts revenue without adding rooms, payroll, or overhead, so it directly improves owner pay.
The inputs are staffed hours, room availability, consult conversion, no-show rate, and room turnover time. The quick math is simple: if schedules sit open, fixed labor and rent stay in place while revenue lags. Idle capacity is the profit leak. Hiring before demand is steady can push cash flow down fast.
Track booked time, not just headcount
Measure utilization by provider and by room each week. Track booked treatments, no-shows, consult-to-treatment conversion, and average turnover minutes. If a dermatologist is closer to 60% booked but aestheticians are at 45%, the weak spot is usually scheduling or conversion, not demand alone.
Fill existing slots before you add staff. Push reminders to cut no-shows, tighten consult follow-up, and standardize room handoff so the next patient starts on time. More booked hours with the same fixed cost means more cash left for owner draws. If demand cannot support the schedule, delay hiring.
2
Patient Acquisition And Retention
Patient Acquisition And Retention
Marketing spend only works when it buys booked treatments. With ad spend modeled at 4% of revenue, the clinic is budgeting about $151K a year, or roughly $12.6K a month. That cost comes out of owner profit unless consults convert, average ticket holds, and patients return for injectables, laser packages, memberships, follow-up care, and referrals.
Here’s the quick math: if repeat visits and referrals lift lifetime value, the same lead can pay back more than once. If they don’t, paid leads become a drag on cash flow, because each new patient must recover acquisition cost before the owner sees real take-home income.
Track CAC and repeat rate
Measure cost per acquired patient against booked treatment value, not vanity leads. Track consult-to-book rate, repeat visit rate, referral share, and revenue from maintenance plans so you can see whether ad dollars are turning into gross profit.
- Watch booked treatments, not clicks.
- Track repeat injectables and memberships.
- Compare CAC to first-year gross margin.
- Cut spend when repeat rate drops.
If acquisition cost rises faster than retention, owner pay gets squeezed fast. The fix is simple: strengthen follow-up care, package maintenance visits, and ask for referrals at the point of highest satisfaction.
3
Pricing Power
Pricing Power
Pricing power is the ability to hold or raise fees without losing the right patients. Year 1 listed prices are $650 for a dermatologist, $450 for a physician assistant, $450 for a nurse practitioner, $300 for a registered nurse, and $150 for a medical aesthetician.
Because the blended ticket is about $381, a 5% lift adds about $19 per treatment. At 826 treatments a month, that is roughly $15.7K in monthly revenue before any cost change, which can flow into profit and owner draw if demand, staffing, and patient experience stay steady.
Track price lift by provider
Measure list price, discounting, booked treatments, and repeat visits by provider type. The key test is simple: does a higher fee raise revenue faster than it hurts conversion or reviews? Bundle follow-up care when it supports value, but do not push price if demand, competition, or compliance weakens.
- Watch close rates after each increase.
- Compare reviews before and after changes.
- Test bundles against single-visit pricing.
If consult quality slips, pricing power fades fast and cash flow gets choppy. Keep the higher fee only when the room stays filled and the extra margin reaches owner pay.
4
Product And Equipment Cost Control
Product and Equipment Cost Control
In this clinic, dermal fillers and neurotoxins run at 9% of revenue, and medical supplies plus skincare products add another 4%. That means 13% of sales goes out the door before the fixed $3K per month maintenance contract. On $100K of revenue, that’s $13K in variable product spend, so waste, over-ordering, and low treatment volume hit owner pay fast.
This driver includes product use, consumables, warranty terms, and device upkeep. The key inputs are treatment volume, product cost per case, inventory turns, and equipment uptime. One line says it plainly: idle devices still cost money. If utilization slips, cash flow tightens even when reported revenue looks fine, because the owner still funds product, maintenance, and supplies before taking any draw.
Track Waste Before You Cut Service Quality
Use treatment-level margin to see what each service really leaves behind after product and device costs. Track waste, inventory turns, consumable use, warranty claims, and lease terms by device and by provider. If a laser or injectable line is busy but margin is thin, better scheduling and higher room use often beat simple cost cuts.
- Match product orders to booked cases.
- Count stock monthly, not quarterly.
- Flag slow-moving inventory fast.
- Watch maintenance downtime by device.
- Price for the true treatment cost.
What this estimate hides: if product waste rises or devices sit idle, owner income drops twice, first through lower gross margin and again through weaker cash flow before distributions. The fix is tight ordering, clear usage logs, and enough booked treatments to spread the $3K monthly maintenance cost across more revenue.
5
Fixed Overhead Discipline
Fixed Overhead Discipline
Fixed overhead is the monthly floor the clinic must cover before owner pay starts. The model lists $257K a month in rent, utilities, equipment maintenance, insurance, software, and admin costs. It also lists a $10K clinic director salary and a $357K fixed base. That is a heavy break-even load, so cash for distributions depends on keeping volume high.
What this estimate hides is capacity risk. A cosmetic dermatology clinic can have great margins on paper, but empty rooms, slow consult conversion, or weak repeat visits make fixed costs harder to absorb. Overhead is useful only when patient volume and revenue capacity justify it. If bookings soften, owner income gets squeezed fast because the floor does not move down.
Track the break-even floor
Track fixed costs by line item each month: rent, utilities, insurance, software, maintenance, and admin salaries. Then compare them with booked treatments and revenue per visit. If fixed cost rises faster than treatment volume, the owner’s draw drops even when sales look steady.
- Watch fixed cost per booked treatment.
- Review utilization before adding staff.
- Delay leases until demand supports them.
- Reforecast before signing new contracts.
Here’s the quick math: the clinic pays these costs every month whether the schedule is full or not. So the best control is not just cutting spend, but matching overhead to real patient demand. If the clinic director salary, software stack, or admin base grows without more volume, profit and cash flow thin out.
6
Compare low, base, and high owner income scenarios
Owner income scenarios
Owner income depends on how fast the clinic fills provider time, holds pricing, and controls payroll. Fixed rent, staffing, and compliance costs make cash discipline the main swing factor.
| Scenario | Low CaseLow Case | Base CaseBase Case | High CaseHigh Case |
|---|---|---|---|
| Launch model | The low case assumes slower bookings and weaker owner take-home while the clinic protects cash. | The base case assumes modeled earnings after fixed costs, reserves, and normal operating spend. | The high case assumes stronger earnings as utilization, pricing, and scale improve. |
| Typical setup | Provider utilization runs below plan, the average ticket slips, and most cash goes to payroll, rent, supplies, and compliance. | The clinic runs near plan with steady treatment volume, balanced pricing, and enough margin to support owner distributions after payroll and overhead. | More provider time is filled, higher-value treatments lift the ticket, and margin improves while staffing, compliance, and cash controls stay tight. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | Owner draw pausedLow Case | Owner draw after reservesBase Case | Strong distribution upsideHigh Case |
| Best fit | Use this to test a slow launch, weak demand, or a longer path to stable bookings. | Use this as the working plan for lender, investor, and cash-flow modeling. | Use this to test capacity limits and whether growth still works after hiring and compliance costs. |
Planning note: Scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distribution policy.
Related Products
- Cosmetic Dermatology Clinic Porter's Five Forces Analysis
- Cosmetic Dermatology Clinic BCG Matrix
- Cosmetic Dermatology Clinic Business Model Canvas
- 7 Critical KPIs to Scale Your Cosmetic Dermatology Clinic
- Cosmetic Dermatology Clinic Business Plan Template in Pre-Written Word
- Increase Cosmetic Dermatology Clinic Profitability: 7 Proven Strategies
- Operating Costs: How Much To Run A Cosmetic Dermatology Clinic Monthly?
- Cosmetic Dermatology Clinic Startup Costs: Plan For $615K+ CAPEX
- Cosmetic Dermatology Clinic Financial Model Template in Excel
- How To Open A Cosmetic Dermatology Clinic In 4 To 9 Months
- How to Write a Cosmetic Dermatology Clinic Business Plan
- Cosmetic Dermatology Clinic Marketing Mix
- Cosmetic Dermatology Clinic Marketing Plan
- Cosmetic Dermatology Clinic Business Proposal
- Cosmetic Dermatology Clinic PESTEL Analysis
- Cosmetic Dermatology Clinic Pitch Deck Example Editable PPTX
- Cosmetic Dermatology Clinic Business SWOT Analysis
- Cosmetic Dermatology Clinic Value Proposition Canvas
Frequently Asked Questions
The model shows up to $263M in Year 1 operating profit before tax, debt service, reserves, and distributions That comes from $377M annual revenue and a roughly 70% modeled margin after listed costs Actual owner take-home can be lower if the clinic keeps cash for growth, equipment, payroll, or working capital