 Owner incomeEBITDA $25k–$4.16M
Owner incomeEBITDA $25k–$4.16MHow Much Dermal Filler Training Owners Make: $25k To $416M

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner incomeEBITDA $25k–$4.16M  Net margin2.0%–55.6%
Net margin2.0%–55.6% Revenue for target pay$7.48M
Revenue for target pay$7.48M Business difficultyHard
Business difficultyHard


A dermal filler training business owner can plan around EBITDA of about $25k in Year 1, $410k in Year 2, and $4160M by Year 5 in the researched model EBITDA is earnings before interest, taxes, depreciation, and amortization, so it is not the same as cash the owner can spend Revenue rises from $1221M to $7480M as billable days grow from 12 to 22 per month and occupancy rises from 65% to 92% Owner take-home depends on reserves, debt service, taxes, and whether the owner also fills a paid role such as Medical Director or instructor
Owner incomeEBITDA $25k–$4.16MNet margin2.0%–55.6%Revenue for target pay$7.48MBusiness difficultyHardWant to test your owner pay?
Owner income calculator
Estimate owner take-home and target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: Research-based planning estimate only. It is not guaranteed salary, tax advice, or owner distribution advice.
Want to check owner income in the Dermal Filler Injection Training model?
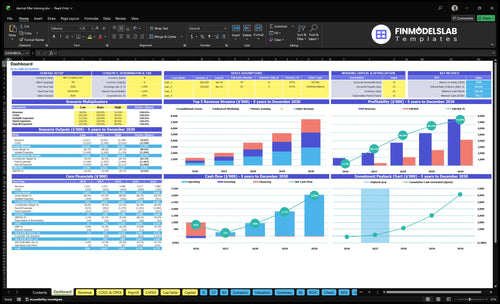
This Dermal Filler Injection Training Financial Model Template shows the dashboard, tuition, class capacity, billable days, occupancy, instructor payroll, supplies, marketing, fixed overhead, capex, cash flow, and owner income. It also charts revenue from $1221M to $7480M, EBITDA from $25k to $4160M, a $791k cash need in Month 2, break-even in Month 2, and 20-month payback. Open the model to test scenarios.
Owner-income model highlights
- Owner take-home is clear
- Revenue and EBITDA charts
- Month 2 cash need
What is the profit margin on dermal filler training courses?
The profit margin on Dermal Filler Injection Training courses is weak at launch: the direct and variable cost load starts at 220% of revenue and only improves to 160% by Year 5, so the course-level margin is still under pressure unless volume, pricing, and class utilization rise fast. For KPI context, see What Are The 5 KPIs For Dermal Filler Injection Training Business?
Cost load pressure
- 220% of revenue at start
- 160% by Year 5
- Includes product and consumables
- Includes marketing and CME fees
Fixed cost base
- $21,450 monthly fixed costs
- $12,000 clinical rent
- $2,500 liability insurance
- Payroll is the biggest leakage
Here’s the quick math: fixed costs alone total $21,450 per month from rent, insurance, utilities and waste, software, maintenance, and legal and regulatory compliance. The real margin drag is payroll, which grows from $580k to $1.435M, so profit only improves if enrollment, pricing, and utilization outrun added staff.
Revenue drivers
- More filled seats
- Higher course price
- Better room utilization
- Faster class fill rates
Watch this first
- Track payroll growth monthly
- Watch direct cost per seat
- Keep marketing efficient
- Protect class occupancy
Can a dermal filler training business scale beyond the owner?
Yes—Dermal Filler Injection Training can scale beyond the owner, but only if it swaps founder delivery for hired instructors and tighter quality control. Here’s the quick math: the lead aesthetic instructor load rises from 1 FTE at $165k in Year 1 to 4 FTEs by Year 5, while billable days grow from 12 to 22 per month, or about 83% more capacity. That means growth depends on enough models, rooms, supplies, admissions, and reviews to keep instructors busy.
Scale drivers
- Use hired instructors, not founder time
- Run foundational, advanced, private courses
- Keep instructor utilization high
- Match seats to room and model supply
Key risks
- Credentialing gaps can hurt trust
- Weak student outcomes can drive refunds
- Compliance-sensitive claims raise risk
- Margin can thin as payroll grows
How much revenue does a dermal filler training business need to pay the owner?
For Dermal Filler Injection Training, the model shows that about $1.221M in Year 1 revenue still leaves only roughly $25k EBITDA, so owner pay is very tight once you allow for taxes, debt, reserves, and reinvestment. Monthly fixed overhead is $21,450, or about $257,400 a year before payroll, and payroll rises from $580k in Year 1 to $1.435M by Year 5.
Year 1 load
- $21,450 monthly fixed overhead
- $257,400 yearly overhead before payroll
- $580k Year 1 payroll
- $1.221M Year 1 revenue
Owner pay room
- 220% direct and variable costs in Year 1
- 160% direct and variable costs by Year 5
- Only about $25k EBITDA in Year 1
- Owner pay needs more cushion
What drives owner income most?
1
65%-92%Paid Enrollment
Seat fill moves from 65% to 92%, and that is the cleanest volume lever behind the jump in owner income.
2
$3.2K-$10KTuition Mix
Foundational, advanced, and private tuition rises from $3,200 to $10,000, so a richer mix lifts revenue per learner.
3
12-22/moCourse Capacity
Billable days rise from 12 to 22 each month, so the same rooms and staff can sell more classes without new space.
4
$575K-$1.44MInstructor Payroll
Payroll grows from about $575K to $1.44M as FTEs rise, so utilization has to stay tight or margin gets squeezed.
5
22%-16%Direct Costs
Direct and variable costs ease from 22% to 16% of revenue, and every point saved drops straight to EBITDA.
6
6%-4%Lead Conversion
Digital acquisition spend falls from 6% to 4% of revenue, plus lower certification fees help keep each booked seat cheaper.
Dermal Filler Injection Training Core Six Income Drivers
Paid Enrollment And Cohort Fill Rate
Paid Enrollment And Cohort Fill Rate
Paid seats are the main revenue engine. Fill rate means paid seats ÷ total seat capacity, so revenue only grows when more of each cohort is booked and paid. Occupancy rising from 65% in Year 1 to 92% in Year 5 is about a 41.5% jump in filled seats per class, before any price change.
Here’s the quick math: Year 1 tuition is $3,200 foundational, $4,500 advanced, and $8,500 private. If class size stays capped, better fill rate lifts revenue and owner pay faster than rent, software, or insurance. The main risks are model availability, student-to-instructor ratios, refunds, eligibility screening, and poor reviews.
Track Seats, Not Just Leads
Measure paid fill rate by course type, not just inquiries. A paid seat that stays enrolled is what turns capacity into income. Watch the gap between booked, paid, and attended seats so you can catch weak screening, refund pressure, or a mismatch between demand and your class limits.
Track these each month:
- Paid seats by cohort
- Refund rate and deferrals
- Seats per instructor day
- Review score after class
If fill rate improves without a similar rise in clinical overhead, more tuition drops to profit. If occupancy rises but refunds or complaints rise too, the income gain can vanish fast.
1
Tuition Pricing And Course Mix
Tuition and Course Mix
This driver sets revenue per seat, so it has a direct line to owner pay. Here’s the quick math: foundational tuition rises from $3,200 to $3,600 (+$400, 12.5%), advanced from $4,500 to $5,200 (+$700, 15.6%), and private training from $8,500 to $10,000 (+$1,500, 17.6%). If the mix shifts toward premium seats, gross profit can rise fast.
That only works when price matches hands-on time, instructor skill, student outcomes, and clear prerequisites. If trust is weak, higher tuition can cut conversion, trigger refunds, and slow cash flow. The owner’s take-home income improves only when the seat price lift holds occupancy and does not force higher marketing spend just to fill the class.
Price by proof, not hope
Track tuition by course type, filled seats, refund rate, and lead-to-enrollment conversion. Revenue is simple: seats sold × tuition. If premium pricing lifts revenue but fill rate drops, owner income can fall even when posted prices rise.
Test price increases one course at a time and tie each higher price to something concrete: more instructor time, smaller class size, or deeper clinical practice. Keep prerequisites tight, document outcomes, and watch whether the higher-priced mix still fills before you raise the next tier.
- Track seats sold by course.
- Watch refunds after each price change.
- Compare conversion by tuition tier.
- Protect trust with clear prerequisites.
2
Course Frequency And Capacity
Course Frequency And Capacity
This driver is about how many billable days you run each month and whether each class has enough seats, staff, and clinical space to fill them. The disclosed model shows annual revenue rising from $1,221 to $7,480 as billable days move from 12 to 22, so cadence can lift owner pay fast when occupancy holds.
Here’s the catch: more cohorts only help if lead flow, instructors, models, clinical rooms, and admissions can keep up. If treatment stations, scheduling, medical waste workflows, or student support lag, you can add revenue and still hurt safety, reviews, and referrals.
Track Seats Before You Add Dates
Measure filled seats per teaching day, class utilization, and the time it takes to book a cohort. Then test one extra course date only after you know the next class can be staffed, supplied, and fully admitted.
- Track seats, not just inquiries.
- Cap class size to safe ratios.
- Match dates to instructor availability.
- Check room, model, and waste capacity.
Profit improves when each added day spreads fixed costs over more paid students. But if you rush cadence, refunds and weak reviews can erase the gain, so watch conversion, no-show rate, and post-course feedback before you scale again.
3
Instructor Model And Utilization
Instructor Utilization Drives Margin
Expert payroll is a fixed cost that can move owner pay fast. A Lead Aesthetic Instructor costs $165k per FTE, scaling from 1 FTE in Year 1 to 4 FTEs in Year 5, and the Medical Director adds $220k each year. That puts annual expert payroll at about $385k in Year 1 and $880k by Year 5 before other overhead.
The key inputs are instructor headcount, teaching days, filled seats per day, and revenue per instructor. Owner-taught courses can save cash, but not economic cost, because the owner’s time still has value. If instructors are underused, or class quality slips, margin drops, refunds rise, and the owner has less profit to draw.
Track Revenue per Teaching Day
Measure utilization, not just payroll. Track revenue per instructor, filled seats per teaching day, and the ratio of paid seats to expert payroll. If seat fill is weak, adding instructors can dilute margin fast. If owner-taught classes are used, price them as real labor, not free labor.
- Match instructors to filled cohorts.
- Watch credentialing and teaching consistency.
- Use fill rate before adding FTEs.
- Protect quality to avoid refund risk.
4
Direct Course Costs
Direct Course Costs
Hands-on dermal filler training burns real supplies, so this driver hits gross margin fast. The main inputs are filled seats, tuition per seat, and variable course cost: injectable product, medical consumables, model coordination, syringes, materials, disposal, equipment, and room setup. If injectable product supply is 100% of revenue in Year 1 and 80% by Year 5, owner pay only improves when waste falls faster than tuition growth.
This is a per-course cost problem, not a fixed-overhead problem. Keep variable costs separate from fixed rent and startup capex so you can see contribution by cohort. One line says it best: if the class looks full but product use is sloppy, the owner still feels the margin leak in cash flow and take-home profit.
Track Cost Per Seat
Track direct cost per student and direct cost per cohort every class. Benchmark medical consumables at 35% to 25% of revenue, then test whether tighter ordering, cleaner room setup, and better model coordination cut spend without hurting hands-on practice quality.
Build the calculator with seat count, tuition, product used per student, consumables, disposal, and setup labor. If gross margin per seat drops, fix purchasing and class prep first. Cutting materials too hard can protect cash short term, but it can also damage training quality, reviews, and repeat demand.
5
Lead Generation And Conversion
Lead Generation And Conversion
Empty seats hit income fast because each missed enrollment drops tuition with little offset in fixed costs. In year 1, digital acquisition marketing is 60% of revenue, then falls to 40% by year 5 as trust, reviews, and referral flow improve. One clean rule: more qualified leads and higher conversion lift EBITDA without adding clinical overhead.
This driver uses four inputs: lead volume, lead quality, conversion rate to paid seat, and refund rate. Stronger results come from reviews, instructor credentials, referral partners, clear prerequisites, and credible before-and-after education claims. The risk is bad-fit applicants, noncompliant claims, and refund pressure, which can turn paid marketing into wasted cash.
Track Qualified Leads, Not Just Clicks
Measure cost per qualified applicant, application-to-enrollment rate, and refund rate by channel. If one source brings cheap leads but poor eligibility, it will look good in marketing and bad in cash flow. Here’s the quick math: lower acquisition cost on each filled seat raises gross profit, and that flows straight to owner pay.
Control the front end hard. Use prerequisites on every ad and landing page, document clinical claims carefully, and test referral partners that send licensed, ready-to-buy practitioners. A simple goal is better seat fill with fewer refunds, because empty seats and weak-fit students drain margin faster than most owners expect.
- Track qualified leads by source
- Watch seat fill by cohort
- Review refund reasons monthly
- Screen eligibility before payment
- Protect claims compliance in ads
6
Compare lean, base, and growth owner-income cases
Owner income scenarios
Owner income moves mainly with occupancy and billable days because fixed payroll and clinical overhead stay heavy. The spread here shows how fast margin improves once lead flow and instructor capacity are stable.
| Scenario | Low CaseLow Case | Base CaseBase Case | High CaseHigh Case |
|---|---|---|---|
| Launch model | This is the tight launch path, with 65% occupancy, 12 billable days, and Year 1 EBITDA at $25k. | This is the modeled path, with 75% to 82% occupancy, 15 to 18 billable days, and EBITDA rising from $410k to $1.348M. | This is the stronger earnings path, with 88% to 92% occupancy, 20 to 22 billable days, and EBITDA scaling from $2.508M to $4.160M. |
| Typical setup | Year 1 revenue is $1.221M, direct costs start near 13.5%, variable costs run about 8.5%, and payroll plus fixed overhead absorb most of the margin. | Revenue moves from $2.037M to $3.680M as direct costs ease from 12.7% to 10.5%, and the larger course mix spreads payroll and overhead better. | Revenue reaches $5.217M to $7.480M as direct costs fall to 8.5% to 8.0%, and a trained instructor bench supports more private training. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $25kLow Case | $410k - $1.35MBase Case | $2.51M - $4.16MHigh Case |
| Best fit | Use this to stress-test a cautious launch, thin reserves, and slow lead flow. | Use this if lead flow is proven and you want a realistic planning case. | Use this to test upside when instructor capacity is built and demand stays near full. |
Planning note: Scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Dermal Filler Injection Training Porter's Five Forces Analysis
- Dermal Filler Injection Training BCG Matrix
- Dermal Filler Injection Training Business Model Canvas
- What Are The 5 KPIs For Dermal Filler Injection Training Business?
- Dermal Filler Business Plan Template in Pre-Written Word
- How Increase Dermal Filler Injection Training Profits?
- What Are Operating Costs For Dermal Filler Injection Training?
- Dermal Filler Injection Training Startup Costs: $791k Cash Need
- Dermal Filler Injection Training Financial Model Template in Excel
- How to Launch a Dermal Filler Training Business in 60–120 Days
- How To Write A Business Plan For Dermal Filler Injection Training?
- Dermal Filler Injection Training Marketing Mix
- Dermal Filler Injection Training Marketing Plan
- Dermal Filler Injection Training Business Proposal
- Dermal Filler Injection Training PESTEL Analysis
- Dermal Filler Injection Training Pitch Deck Example Editable PPTX
- Dermal Filler Injection Training Business SWOT Analysis
- Dermal Filler Injection Training Value Proposition Canvas
Frequently Asked Questions
In the researched model, EBITDA is $25k in Year 1, $410k in Year 2, and $4160M by Year 5 That is not guaranteed owner cash The owner still needs to fund reserves, taxes, debt service, capex, and any working capital gaps before taking distributions