 Time to Open8-12 weeksOpening prep
Time to Open8-12 weeksOpening prepStart a Dialysis Patient Transportation Service in 45–120 Days

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Time to Open8-12 weeksOpening prep  Launch Sequence7 stagesCompliance first
Launch Sequence7 stagesCompliance first Key BottleneckPayer accessApproval path
Key BottleneckPayer accessApproval path First Revenue StepBooked routeBooking live
First Revenue StepBooked routeBooking live


You’re opening a recurring medical ride operation, not just buying a van This guide covers the launch path for non-emergency medical transportation (NEMT) for dialysis patients, from compliance checks and vehicle readiness to dispatch, clinic outreach, and first rides in a typical 45–120 day opening window Use the Year 1 model assumptions, including $50–$90 average order values by channel, to validate launch volume before you accept patients
Time to Open8-12 weeksOpening prepLaunch Sequence7 stagesCompliance firstKey BottleneckPayer accessApproval pathFirst Revenue StepBooked routeBooking liveLaunch timeline
Short web summary; the XLSX export contains the detailed Gantt Chart and task logic.
Launch scheduleWeek 1Week 2Week 3Week 4Week 5Week 6Week 7Week 8Week 9Week 10Week 11
Compliance
- Form entity
- Check NEMT rules
- Review payer rules
- File permits
- Confirm compliance file
Insurance
- Get broker quotes
- Bind auto policy
- Set liability limits
- Issue certificates
Vehicles
- Source vehicles
- Inspect accessibility
- Install safety gear
- Set cleaning plan
Staffing
- Recruit drivers
- Run screenings
- Check licenses
- Train drivers
- Build backup roster
Dispatch
- Map schedules
- Set return trips
- Write no-show rules
- Test routing
Outreach
- Build lead list
- Visit clinics
- Meet dialysis centers
- Run test rides
Why test the launch plan with a financial model before opening?
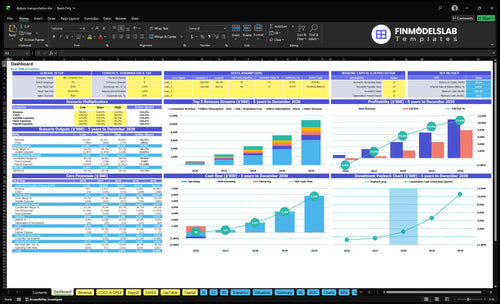
The Dialysis Patient Transportation Financial Model Template dashboard shows revenue, costs, assumptions, cash runway, staffing, utilization, and break-even logic—open the model.
Financial model highlights
- Startup costs: $80k, 200 buyers
- Revenue assumptions: $50/$70/$90 AOVs
- Channel mix: clinics, dialysis centers, hospitals
- Break-even planning: 45–120 day timing
How long does it take to start a dialysis transportation business?
Dialysis Patient Transportation usually takes 45–120 days to start, with the fastest path being a small service area and simple ambulatory rides. Most delays come from insurance underwriting, local approvals, vehicle purchase or inspection, driver screening, broker credentialing, and clinic referral development. Don’t take patients before insurance, vehicle readiness, and driver clearance are complete; if you add wheelchair service, multiple vehicles, or broader payer access, the timeline moves toward the long end.
Fastest launch path
- Start with ambulatory rides only.
- Keep one service area tight.
- Run setup tasks in parallel.
- Check progress every week.
Common delay points
- Insurance review slows launch.
- Vehicle inspection can add days.
- Driver screening must clear first.
- Broker and clinic onboarding takes longer.
What do you need to start a dialysis transportation business?
To start a Dialysis Patient Transportation business, you need business registration, a defined service area, verified non-emergency medical transportation (NEMT) rules, bound commercial auto and liability insurance, compliant vehicles, qualified drivers, patient-safety procedures, dispatch workflow, and referral access. Start by checking state, county, insurer, broker, and payer rules; in-center dialysis often means 3 treatments per week, so missed pickups can disrupt life-sustaining care—use How Much To Start Dialysis Patient Transportation Business? for startup cost planning.
Core Requirements
- Register the business entity
- Define your service area
- Verify NEMT payer rules
- Bind insurance before rides
Operational Proof
- Choose ambulatory or wheelchair service
- Document driver qualifications
- Set safe transfer procedures
- Prepare backup driver coverage
What launch mistakes hurt dialysis transportation reliability?
The biggest launch mistake in Dialysis Patient Transportation is treating it like a normal ride service. Dialysis trips repeat weekly, so one missed pickup can hit patient care and the referral channel fast; start with tested routes, clear return rules, and backup coverage.
Big launch mistakes
- Underestimate recurring schedule complexity.
- Run without backup driver coverage.
- Leave pickup and return rules vague.
- Skip insurance and clinic coordination.
First-month focus
- Test routes before full launch.
- Document no-show and late-treatment contacts.
- Save caregiver and after-hours contacts.
- Do fewer routes well, not maximum coverage.
Confirm what must be ready before accepting dialysis rides
Launch readiness checklist
Use this go-live approval checklist before opening to confirm the service is ready to start.
Compliance
- Business registration filedCritical
Needed before permits, banking, and contracts move ahead.
- Transport rules confirmedCritical
City, county, and state rules can block service if missed.
- HIPAA-safe message rules setHigh
Protect patient details in texts, calls, and dispatch notes.
Vehicles
- Commercial auto boundCritical
No ride should start before auto coverage is active.
- Service scope chosenCritical
Ambulatory and wheelchair work need different equipment and training.
- Vehicles inspectedHigh
Check brakes, belts, lifts, and clean condition before first trip.
- Safety equipment installedHigh
First-aid kits, signs, and restraints should be in place.
Dispatch
- Dispatch software testedCritical
You need live booking, tracking, and trip logging on day one.
- Pickup-return rules setHigh
Clear trip rules cut missed rides and late returns.
- No-show escalation setHigh
Staff need one process when a patient doesn't appear.
- Late-treatment protocol setHigh
Clinics need a plan when dialysis runs late.
- Caregiver handoff rules setMedium
Define who can release and receive each rider.
Training
- Driver background checks passedCritical
Screening lowers risk before riders get in the vehicle.
- Patient-assist training completedHigh
Drivers must know safe boarding and patient support steps.
- Wheelchair securement trainedHigh
Only needed if you launch wheelchair service.
- Backup driver coverage plannedCritical
Trips fail fast when one driver calls out.
Referrals
- Clinic contact list verifiedHigh
Use one clean list for schedulers, nurses, and transport leads.
- Referral path confirmedCritical
Know how the first rides will come in.
- Service hours alignedHigh
Hours must match dialysis appointment windows.
- First revenue routes mappedMedium
Pick the first clinics, centers, or hospitals to open with.
Finance
- Cash runway covers Month 14Critical
Core metrics show minimum cash at Month 14.
- Year 1 AOV model checkedHigh
Test $50, $70, and $90 ride values against the plan.
- Go-live signoff completedCritical
Launch is not ready if insurance, backup coverage, dispatch, or referral path is missing.
Which launch drivers matter most?
1Compliance
Insurance gateBind commercial auto and liability first; without active coverage, patient rides cannot start.
2Vehicle Setup
45-120 daysChoose ambulatory or wheelchair vans, and keep backups ready to reduce cancellations.
3Driver Training
Backup crewScreen, train, and backfill drivers so one callout doesn't break the route.
4Dispatch
Recurring routesSet recurring ride schedules and backup rules before go-live to protect on-time service.
5Referral Access
50/30/20 mixYear 1 mix is 50% clinics, 30% dialysis centers, 20% hospitals.
6Cash Runway
$28KModel the $50/$70/$90 order value mix and protect runway until the $28K cash trough.
Compliance and insurance readiness
Compliance and insurance readiness
For dialysis patient transportation, this is a go or no-go gate. You can have vehicles, drivers, and clinic interest, but if state and local rules, city permits, or payer and broker credentialing are still open, you cannot legally start patient rides on day one.
The main bottleneck is usually insurance underwriting or missing broker paperwork. Bind commercial auto and general liability before the first trip, and confirm workers compensation where it applies. A clinic-ready operator still cannot move patients if coverage is not active.
Bind coverage before bookings
Build the launch file set first: permits, insurer conditions, vehicle documents, driver files, and broker or payer credentials. That keeps the opening plan realistic and avoids false starts that burn cash and strain clinic trust.
- Verify state and city rules first.
- Bind coverage before patient rides.
- Check vehicle and driver records.
- Track broker approvals in one file.
- Escalate underwriting delays early.
Here’s the key test: if the first ride is booked, can the full file prove the service is insurable, credentialed, and cleared to operate? If not, delay the start date rather than risk a failed first week and unsafe launches.
1
Vehicle and accessibility setup
Vehicle Setup
Your first fleet choice decides whether you can serve patients on day one. Pick ambulatory or wheelchair-accessible service based on target patients, referral channels, and driver training. Not every launch needs wheelchair vans, but the vehicle mix must match the trips you expect to book.
This matters most for recurring dialysis runs. Early-morning clinic routes need reliable heating, safe entry, and predictable turnaround. If a vehicle fails inspection or you have no backup vehicle, rides get canceled and referral trust drops fast.
Inspect Before First Pickup
Before opening, check each vehicle for safety equipment, cleanliness, maintenance plan, route fit, and recurring schedule fit. Match the vehicle to the patients you will actually serve, not the fleet you wish you had. If your first referrals include wheelchair users, confirm secure entry and handling before you accept those trips.
Set backup coverage before launch and test the full route flow. One clean one-liner: no backup means no dependable launch. The goal is simple—fewer cancellations, safer first rides, and enough reliability for clinics to trust repeat bookings.
- Inspect every vehicle before accepting rides.
- Match vehicle type to patient needs.
- Confirm heating and safe entry.
- Document maintenance and cleaning steps.
- Keep backup capacity ready.
- Test early-morning route turnaround.
2
Driver hiring and training
Driver Hiring and Training
If the driver file is weak, you do not have a patient-ready business. For dialysis transport, driving record checks, background checks, and drug screening where required protect safety and clinic trust, and they need to be finished before the first ride. Training also has to cover patient help, punctual pick-up, clinic communication, safe transfers, and wheelchair securement if you serve wheelchair riders.
The launch risk is simple: one driver handling every ride. If a return trip runs late after treatment and no backup is ready, the next appointment slips too, and that can trigger missed dialysis sessions. Strong hiring and training support on-time performance from day one, which is what clinics notice first.
Build Backup Coverage Before Routes Start
Before you accept recurring routes, verify each driver’s file, assign route coverage, and document who steps in if a trip runs long. Keep the training checklist tied to the work: patient assistance, punctuality, clinic communication, safe transfer, and securement steps. That keeps the launch plan real, not hopeful.
Test the handoff on a live-style schedule. If the first driver is delayed after treatment, the backup should still be able to cover the return ride without scrambling. That single test shows whether the business can operate from day one without missed appointments or service gaps.
- Check driving records first
- Run background checks
- Complete drug screening if required
- Train on patient support
- Document backup driver coverage
3
Dispatch and recurring scheduling systems
Dispatch and recurring scheduling
Dialysis rides live or die on fixed appointment cadence, early-morning pickups, and return-trip coordination. If dispatch is built like a one-off taxi board, you can open with vehicles and drivers ready on paper but still fail on day one when standing routes, caregiver calls, and clinic timing do not line up.
The launch risk is simple: treatment runs late, and the assigned driver is already booked elsewhere. That creates missed returns, no-shows, and clinic distrust fast. Build route batching, no-show rules, and backup plans before taking live patients so the first week proves you can handle recurring medical rides, not just single trips.
Test dispatch before live patients
Map each recurring route by clinic, pickup window, return window, and caregiver contact. Test the dispatch board with early-morning pickups and same-day changes before go-live. The system needs a clean handoff for delays, and staff need one rule for when a ride shifts or drops.
Assign backup coverage to every standing route and document the no-show process. If one driver or one vehicle is the only plan, launch risk jumps. A clean dispatch setup should let you update the clinic, the patient, and the caregiver without breaking the rest of the day.
4
Referral, broker, clinic, and payer access
Referral Access
This driver decides if a ready fleet gets paid trips on day one. The business needs named referral paths through dialysis centers, clinic social workers, case managers, hospitals, local providers, brokers, and Medicaid transportation channels where they apply; otherwise the vans can sit idle after launch. Referral relationships help start demand, but they are not the same as guaranteed contracts.
The Year 1 buyer mix assumes 50% clinics, 30% dialysis centers, and 20% hospitals. The bottleneck is vehicle-ready operation with no payer or referral channel, because the fleet can be ready and the schedule can still be empty. Private-pay families can fill gaps, but repeatable revenue usually comes from clinical referral flow.
Map the booking path first
Before opening, document who can send a patient, how each source books, and what each one needs to release a trip. Separate referral contact, non-emergency medical transport (NEMT) broker onboarding, and contract approval in your tracker so you know which channel can produce rides now and which only creates pipeline. That keeps launch timing realistic.
Your launch inputs are the referral list, booking rules, broker documents, and patient handoff steps. If one hospital or dialysis center needs a different form or contact chain, the first rides can slip and the team may waste time chasing missing details instead of dispatching trips.
- List every target clinic and dialysis center.
- Confirm hospital discharge contacts.
- Verify broker onboarding requirements.
- Track first-trip source and repeat use.
5
Cash runway and utilization planning
Cash runway and utilization planning
Opening on time depends on cash covering the gap between launch costs and first collections. With $80,000 for buyer acquisition and $400 CAC, the plan assumes 200 acquired buyers; that only works if ride volume and reimbursement timing are modeled before day one. Fuel, insurance start date, vehicle payments, and driver hours all hit cash before the $111,500 Year 1 commission flow shows up.
Here’s the quick math: first-month ride volume and vehicle utilization decide whether each route pays its own way. The mix matters too, because Year 1 AOV is $50 for clinics, $70 for dialysis centers, and $90 for hospitals. If private-pay collections lag or reimbursement lands late, a full schedule can still create a cash shortfall.
Build the cash map before first rides
Model when cash leaves, when cash returns, and how many rides each vehicle must run to cover fixed bills. Use the Year 1 repeat order assumptions of 20 clinics, 60 dialysis centers, and 150 hospitals to test whether dispatch, staffing, and route density can support day-one service. No route should launch without a cash plan tied to actual ride timing.
Also verify reimbursement timing, private-pay collection days, and the start date for insurance and vehicle payments. If driver hours are set before volume is real, runway gets tight fast. A practical test is simple: can the first 30 days of booked rides cover fuel, driver pay, and scheduled fixed costs without new funding?
- Map first-month ride volume by route.
- Track reimbursement and cash delay days.
- Match driver hours to booked rides.
- Start insurance before patient pickups.
- Test breakeven utilization by vehicle.
6
Related Products
- Dialysis Patient Transportation Porter's Five Forces Analysis
- Dialysis Patient Transportation BCG Matrix
- Dialysis Patient Transportation Business Model Canvas
- What Are The Five KPIs For Dialysis Patient Transportation Business?
- Dialysis Patient Transportation Business Plan Template in Pre-Written Word
- How Increase Dialysis Patient Transportation Profits?
- What Are Dialysis Patient Transportation Operating Costs?
- Dialysis Patient Transportation Startup Costs With $200k Year 1 Marketing
- Dialysis Patient Transportation Financial Model Template in Excel
- How Much Dialysis Transportation Owners Make At A 125% Take Rate
- How To Write A Business Plan For Dialysis Patient Transportation?
- Dialysis Patient Transportation Marketing Mix
- Dialysis Patient Transportation Marketing Plan
- Dialysis Patient Transportation Business Proposal
- Dialysis Patient Transportation PESTEL Analysis
- Dialysis Patient Transportation Pitch Deck Example Editable PPTX
- Dialysis Patient Transportation Business SWOT Analysis
- Dialysis Patient Transportation Value Proposition Canvas
Frequently Asked Questions
Start by defining your service area, patient type, and referral channel Then verify local NEMT rules, secure commercial auto and liability insurance, prepare vehicles, screen drivers, and test dispatch Plan for a 45–120 day launch window Use Year 1 AOV assumptions of $50, $70, and $90 only to validate route economics