 Owner income0 to $1.26M
Owner income0 to $1.26MHow Much Dietitian Practice Owners Make: $0 to $21M Before Tax

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description

Owner income0 to $1.26M  Net margin-223% to 397%
Net margin-223% to 397% Revenue for target pay≈$4.9M
Revenue for target pay≈$4.9M Business difficultyHard
Business difficultyHard


Key Takeaways
- Visits cap revenue, so capacity has to keep rising.
- Collected cash matters more than posted prices.
- Hiring ahead of demand turns payroll into fixed loss.
- Referrals and retention protect utilization and owner income.
Owner income0 to $1.26MNet margin-223% to 397%Revenue for target pay≈$4.9MBusiness difficultyHardWant to test your dietitian practice owner income?
Owner income calculator
Estimate owner take-home and target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: This is a researched planning estimate, not guaranteed salary, tax advice, or owner distribution advice.
Want to see the full Dietitian Practice financial model and owner income?
See the Dietitian Practice Financial Model Template for revenue, margin, costs, reserves, and owner take-home assumptions. Open the model.
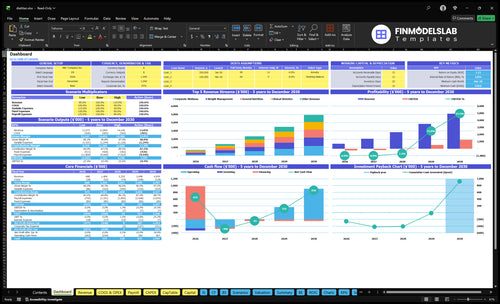
Owner-income model highlights
- Year 1 revenue: $687,600
- Year 3 revenue: $2,332,440
- Year 5 revenue: $4,934,880
- Connects appointments to capacity
- Tracks payroll, overhead, EBITDA
- Includes cash flow and reserves
Can a dietitian practice make more by hiring clinicians?
Yes, but only when utilization fills the schedule and covers payroll. In Dietitian Practice, Year 1 starts with 6 registered dietitians at $75k each, plus admin and marketing labor, and EBITDA after founder salary is -$153,554 by Year 3. By Year 5, 16 registered dietitians support 1,386 visits per month and about $378k EBITDA after founder salary, so don’t add payroll before referrals and scheduling demand are proven.
When hiring helps
- Use hiring after demand is proven.
- Cover payroll with visits.
- Watch support costs closely.
- Grow only with full schedules.
Risk to avoid
- Don’t add staff too early.
- Check referral flow first.
- Check scheduling demand first.
- Year 3 EBITDA is -$153,554.
How much revenue does a dietitian practice need?
For Dietitian Practice, a Year 2 owner-pay target of $120k needs about $1.41M in revenue, using $990k non-owner payroll, $852k fixed costs, and 152% percentage costs. Actual Year 2 revenue is $1.405M, so the practice is basically at full salary support; by Year 3, $2.332M in revenue clears the target and supports about $498k of owner pay before reserves.
Year 2 math
- $120k owner pay target
- $1.41M needed revenue
- $990k non-owner payroll
- $852k fixed costs
Year 3 view
- $1.405M actual Year 2 revenue
- $2.332M Year 3 revenue
- 152% percentage costs
- $498k owner pay capacity
How does payer mix change dietitian practice owner income?
Payer mix changes a Dietitian Practice owner’s income because it changes cash collected, admin work, no-show risk, and how many visits you need to hit the same result. If you’re sizing the business, use How Much Does It Cost To Open And Launch Your Dietitian Practice? and make payer mix editable in the model, then use collected revenue, not list price, because billed charges and cash received can differ. The average collected revenue per completed visit is $127 in Year 1, $141 in Year 3, and $151 in Year 5, so private pay can lower billing friction while insurance can support volume but adds collections work.
Income drivers
- Cash collected changes fast
- Insurance adds collections work
- Private pay cuts billing friction
- No-shows hit visit volume
Model it this way
- Make payer mix editable
- Use collected revenue only
- Track $127, $141, $151
- Base targets on completed visits
Want the six biggest dietitian practice income drivers?
1
450-2,724/moAppointment Volume
More completed visits drive most of the revenue lift, so small gains in monthly volume move owner take-home fast.
2
60%-90%Capacity Fill
Filling more of the schedule turns the same staff base into more billable visits and better margin.
3
$110-$180Service Mix
Shifting toward higher-priced services lifts revenue per slot without needing the same jump in visit count.
4
$127-$151Collected Rate
Better payer mix and cleaner collections raise realized cash per visit, not just booked revenue.
5
10%-6%Referral Engine
Stronger referrals and retention cut marketing spend from 10% to 6% of revenue as utilization improves.
6
$7.1K+11.3%-16.5%Overhead Control
Keeping fixed spend near $7.1K a month and variable costs down protects profit while the practice scales.
Dietitian Practice Core Six Income Drivers
Appointment Volume And Billable Capacity
Completed Visits and Billable Capacity
Weekly completed visits set the revenue ceiling. This practice is modeled at 450 completed visits per month in Year 1, about 104 per week, then 1,386 per month in Year 3, or 320 per week, and 2,724 per month in Year 5, or 629 per week. The key input is completed visits, not booked slots, because no-shows and cancellations shrink real billable output.
If capacity stalls, revenue stalls. Charting, follow-ups, and admin time also eat into clinician hours, so more price per visit will not fix an empty schedule. For the owner, this means take-home income only rises when the team converts more scheduled time into completed visits without breaking service quality or pushing clinicians past workable hours.
Measure Fill Rate, Not Just Bookings
Track the full visit funnel. Start with scheduled visits, then measure no-show rate, cancellation rate, completed visits, and clinician time lost to charting and admin. Here’s the quick math: completed visits = scheduled visits minus losses. If that number flattens, the revenue ceiling stays flat too, even if the calendar looks busy.
- Count completed visits weekly.
- Split losses by cause.
- Time charting and follow-ups.
- Watch admin time per clinician.
- Review capacity before hiring.
Protect billable hours first. Tight reminder systems, shorter gaps between visits, and cleaner handoffs can keep more booked time from turning into lost revenue. What this estimate hides is the real drag from non-billable work: if that load rises faster than completed visits, owner income still gets squeezed.
1
Collected Rate And Payer Mix
Collected Revenue Per Visit
Collected revenue per completed visit matters more than list price in a dietitian practice. In Year 1, service prices run $110 to $160, but the average collected amount is about $127 per completed visit. That means the owner’s income depends on what actually clears after insurance adjustments, unpaid balances, and billing delays, not on the sticker price.
Here’s the quick math: at 450 completed visits per month, collections are about $57,150 a month at $127 per visit. By Year 5, $151 collected per visit on 2,724 visits is about $411,324 monthly. If cash collection slips, profit and owner draw slip too, even when prices look higher on paper.
Track Net Collectible Revenue
Measure net collected per completed visit by payer type, not just posted rates. Break it into insurance, private-pay packages, write-offs, and delayed cash so you can see where the leak is. A practice can raise list prices and still miss target income if denials, offsets, or slow billing drag collections down.
Track collections per visit, days to collect, unpaid balance rate, and package usage each month. If one payer or package pays less than expected, adjust pricing, prepayment rules, or billing follow-up fast. The owner pays themselves from collected cash, so weak payer mix turns revenue into a paper number, not spendable income.
- Completed visits drive the base.
- Collected cash pays the owner.
- Write-offs cut real margin.
- Billing delays squeeze cash flow.
2
Clinician Staffing And Utilization
Clinician Staffing And Utilization
Staffing only helps if booked visits pay for the clinician’s wages, benefits or contractor fees, supervision, billing, and admin time. In this model, registered dietitian headcount rises from 6 FTE in Year 1 to 26 FTE in Year 5, while wage expense climbs from $642,500 to $2,335,000. If visits don’t rise with headcount, payroll turns into a fixed loss.
Utilization matters most: the range is 60% to 90%. At 60%, 40% of clinician capacity is unbilled, so the owner pays for time that does not generate revenue. At 90%, more of payroll is covered by completed visits, which supports gross margin, cash flow, and owner pay. The risk is hiring ahead of demand and locking in costs before the schedule fills.
Track FTE Against Booked Visits
Measure booked visits per clinician, completed visits, and utilization by provider each month. Compare revenue per visit to total clinician cost, not just wages. If a dietitian’s schedule stays below target, slow hiring, add more follow-up slots, or push referral volume before adding another FTE. One empty day can wipe out margin fast.
Use a simple rule: add staff only when booked visits can cover the full load. That load includes pay, benefits, billing, supervision, and admin time. Watch the gap between 60% and 90% utilization closely, because the same team can look profitable at one level and cash-draining at the other. Here’s the quick math: more filled visits, less idle payroll.
3
Service Mix And Program Design
Service Mix Drives Revenue Per Visit
Service mix changes both revenue per visit and retention. Year 5 revenue splits across General Nutrition ($954,720), Weight Management ($1,028,160), Sports Nutrition ($864,000), Clinical Dietetics ($921,600), and Corporate Wellness ($1,166,400), for total service revenue of $4,934,880. Higher-price lines help, but only if completed visits stay full; otherwise cash flow and owner pay slip.
Measure Cash, Not Just Price
Judge packages, follow-ups, group programs, telehealth, and wellness contracts by completed visits, collected cash, and repeat care. A premium offer that raises the fee but lowers utilization can cut profit. The quick test is simple: if the schedule fills and clients return, the mix is working.
- Track completed visits by service line.
- Compare collections to posted fees.
- Watch repeat visits and renewals.
4
Overhead, Admin, And Billing Costs
Overhead, Admin, and Billing Costs
This cost bucket comes out before the owner pays themselves. Fixed overhead is $7,100 per month, made up of $4,500 rent, $600 utilities, $550 insurance, $400 software, $750 accounting and legal, $200 internet and phone, and $100 website. That is $85,200 per year before any variable admin or billing load.
At low revenue, these costs can swallow the whole margin. The model says percentage costs start at 165% of revenue and fall to 113%, so the owner cannot treat top-line sales as take -home pay. Revenue must first cover rent, billing, admin, payroll, reserves, and reinvestment, or distribution stays thin or negative.
Track Cost Load by Revenue
Measure overhead as a share of collected revenue, not booked visits. Here’s the quick math: if overhead is 165% of revenue, every $1.00 collected is offset by $1.65 in overhead, admin, and billing cost before owner pay. As revenue scales, that ratio should move toward 113%, but it is still too high to confuse with profit.
- Track rent, software, and billing separately.
- Forecast cash, not just invoices.
- Watch collections lag every month.
- Keep reserves outside owner draw.
The key input is collected revenue versus the $7,100 fixed base. If billing delays rise, cash flow tightens even when visits look strong. Separate fixed costs, variable costs, payroll, reserves, and reinvestment so owner pay only comes from true surplus, not from gross revenue.
5
Referral Engine And Retention
Referral Engine and Retention
Referrals and repeat clients protect utilization, and utilization protects owner pay. In this model, marketing is 10% of revenue in Year 1 and 6% by Year 5, so the real test is whether spend turns into booked and completed appointments. If referrals slow and the schedule opens up, payroll stays fixed while revenue drops, which cuts gross profit fast.
Track the inputs that actually move cash: completed visits, repeat visit rate, cancellation and no-show rate, and source mix from physician relationships, reviews, niche positioning, recurring follow-ups, and corporate contracts. Here’s the quick math: more filled slots spread fixed staffing and admin costs across more visits; fewer slots leave the same wage base chasing less revenue.
Measure Referrals by Filled Slots
Use booked and completed appointments as the scorecard. Count how many new clients come from physicians, reviews, recurring care, and corporate contracts, then compare that to marketing spend. If a channel brings clicks but no completed visits, it doesn’t help owner income. A healthy referral engine keeps the schedule near target without pushing spend up with it.
Build simple retention rules: schedule follow-ups before the client leaves, watch rebook rates, and flag empty slots early. What this estimate hides: if retention slips, you often lose more than one visit, because every open slot also drags down staff utilization and cash flow. That is why low-cost repeat care is usually worth more than constant lead chasing.
- Track booked visits weekly.
- Track completed visits weekly.
- Separate referral sources.
- Watch repeat booking rates.
- Measure spend against fills.
6
Compare low, base, and high dietitian practice owner income scenarios
Owner income scenarios
Owner pay changes fast with visit volume, collected fees per visit, staffing, and percentage costs. The same practice can swing from no support to strong pay as utilization rises.
| Scenario | Low CaseDownside case | Base CaseCore case | High CaseUpside case |
|---|---|---|---|
| Launch model | This is the lower-income path with tight utilization and weak owner pay support. | This is the modeled middle path with steady utilization and moderate owner pay capacity. | This is the stronger-income path with higher volume, better pricing, and more owner pay room. |
| Typical setup | Year 1 runs at 450 visits per month, $127 collected per visit, $687,600 revenue, 7 clinicians, 165% percentage costs, and $7,100 monthly fixed overhead, which leaves a -223% operating margin and no operating support for owner pay. | Year 3 runs at 1,386 visits per month, $141 collected per visit, $2.332M revenue, 17 clinicians, 139% percentage costs, and a 162% margin, with $498k owner pay capacity before reserves. | Year 5 runs at 2,724 visits per month, $151 collected per visit, $4.935M revenue, 27 clinicians, 113% percentage costs, and a 397% margin, with $2.077M owner pay capacity before reserves. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $0No pay support | $498kCore pay case | $2.077MTop-end pay |
| Best fit | Use this to stress test the practice if volume stays low and margins do not cover owner pay. | Use this as the main planning case for a practice that is scaling but still watching reserves. | Use this to test upside if the practice fills schedules, keeps pricing firm, and manages staffing well. |
Planning note: Scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Dietitian Practice Porter's Five Forces Analysis
- Dietitian Practice BCG Matrix
- Dietitian Practice Business Model Canvas
- 7 Financial KPIs to Scale Your Dietitian Practice
- Dietitian Practice Business Plan Template in Pre-Written Word
- 7 Proven Strategies to Boost Dietitian Practice Profit Margins
- Quantifying the Monthly Running Costs for a Dietitian Practice
- Dietitian Practice Startup Costs: $66k Setup And $533k Runway
- Dietitian Practice Financial Model Template in Excel
- How to Open a Dietitian Practice in 4–8 Weeks or 3–6 Months
- How to Write a Dietitian Practice Business Plan: 7 Actionable Steps
- Dietitian Practice Marketing Mix
- Dietitian Practice Marketing Plan
- Dietitian Practice Business Proposal
- Dietitian Practice PESTEL Analysis
- Dietitian Practice Pitch Deck Example Editable PPTX
- Dietitian Practice Business SWOT Analysis
- Dietitian Practice Value Proposition Canvas
Frequently Asked Questions
Expect tight cash flow during the early ramp-up In the provided Year 1 model, revenue is $687,600, but EBITDA after the $120,000 founder salary is -$153,554 Fixed overhead is $7,100 per month, and total wage expense is $642,500, so the owner may need reserves or outside funding