 Owner income$797k
Owner income$797kHow Much Does a Drugstore Owner Make? Year 1 Cash Flow at $135M

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$797k  Net margin65%
Net margin65% Revenue for target pay$1.69M
Revenue for target pay$1.69M Business difficultyHard
Business difficultyHard


In the researched base case, a drugstore owner has about $797k of first-year operating cash flow capacity on $135M in modeled revenue That is not a guaranteed independent pharmacy owner salary it is cash flow before personal taxes, debt service, reserves, reinvestment, and owner distributions The model assumes 550 weekly visitors, 45% buyer conversion, 18 units per order, a 60% prescription mix, and 110% modeled variable costs What this estimate hides is important: the data lists pharmacy supply costs and shrink, but not a separate prescription drug acquisition cost line
Owner income$797kNet margin65%Revenue for target pay$1.69MBusiness difficultyHardWant to test your drugstore owner income?
Owner income calculator
Estimate owner take-home and target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: Research-based planning estimate only. It is not guaranteed salary, tax advice, or owner distribution advice.
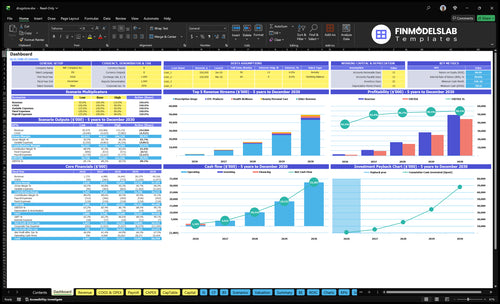
How do you check owner income in the Drugstore model?
This screenshot shows Drugstore Financial Model Template revenue, margin, costs, reserves, and owner pay—open the model.
Owner-income model highlights
- Owner pay scenarios
- Revenue and margin
- Drivers and assumptions
How many prescriptions does a drugstore need to be profitable?
Drugstore needs about 15 prescriptions per day to break even on prescriptions alone, based on $404k in annual payroll plus fixed costs, an $85 prescription price, and 89% contribution after listed variable costs; for metric tracking, start with What Is The Most Critical Metric To Measure The Success Of Drugstore?. Here’s the quick math: $404,000 / ($85 × 89% × 365) = 14.6 prescriptions per day.
Break-even math
- Fixed costs: $404k annually
- Prescription price: $85
- Contribution: 89% after variable costs
- Break-even: about 15 scripts/day
What changes it
- Watch reimbursement margin closely
- Improve generic prescription mix
- Control prescription drug cost
- Add front-end retail sales
Is owning a drugstore profitable despite reimbursement pressure?
A Drugstore can be profitable, but only if reimbursements land fast and costs stay inside plan. Here’s the quick math: $135M first-year revenue, $270k payroll, $1.344M fixed expenses, and 110% variable costs make cash flow very sensitive. So the safe move is sensitivity planning, because owner take-home can fall before the income statement shows the pain.
Cash flow math
- $135M first-year revenue
- $270k payroll load
- $1.344M fixed expenses
- 110% variable-cost risk
Main risks
- Payer mix can crush margin
- Delayed reimbursements trap cash
- Inventory and wholesaler terms squeeze working capital
- Reserves matter if margins tighten
How do prescription and OTC margins affect drugstore owner income?
Prescription-heavy sales can look strong, but Drugstore owner income depends on reimbursement spread, payer fees, and drug acquisition cost, not just top-line revenue. In this mix, 60% prescription, 20% OTC, 10% health and wellness, and 10% beauty and personal care at listed prices of $85, $15, $25, and $18 create a $58.30 weighted unit price and a modeled $104.94 order value; see How Much Does It Cost To Open And Launch Your Drugstore Business?
Sales mix
- 60% prescription revenue drives volume.
- 20% OTC adds higher visible retail margin.
- 10% health and wellness lifts basket size.
- 10% beauty and personal care diversifies sales.
Margin reality
- Model gross margin is 94.5%.
- COGS here includes supply cost and shrink only.
- Prescription income depends on payer reimbursement.
- Actual take-home drops with fees and acquisition costs.
Want the six drugstore income drivers?
1
60%Rx Mix
About 45% of visitors buy, and prescriptions make up 60% of sales at about $85 each, so fill count and reimbursement set the take-home ceiling.
2
40%-45%Front End
OTC, health, and beauty lift non-Rx mix from 40% to 45%, and that helps margin because those items are less tied to reimbursement.
3
$270KLabor Mix
Year 1 payroll is about $270K, so staffing tightness and how much the owner works the floor have a big effect on profit left to draw.
4
3%-4%Supply Terms
Pharmacy supply cost drops from 4.0% to 3.0% and shrinkage from 1.5% to 1.0%, so better buying terms keep more cash.
5
24-48 moRepeat Care
Longer repeat life turns one patient into more refill trips and add-on sales, which lifts lifetime margin.
6
$11.2K/moOverhead Base
Rent, software, insurance, and the rest of the fixed base run about $11.2K a month, so owner pay only shows up after the store clears that floor.
Drugstore Core Six Income Drivers
Prescription Volume And Reimbursement Margin
Prescription Volume and Reimbursement Margin
This driver is the gap between what the payer pays and what it costs to fill the script. In the first-year model, the store uses $85 per prescription-priced unit and a 60% prescription sales mix. At about 15 units per day, the model is near break-even before debt, taxes, reserves, and any unlisted acquisition costs.
The real swing is reimbursement spread, not raw volume. Payer mix, generic dispensing, DIR fees, and cost of goods can turn busy traffic into weak cash flow if the spread is thin. When the spread holds, scripts also bring repeat visits, so this driver has a high effect on owner pay.
Protect the spread
Track net margin per prescription by payer and drug type, not just script count. Measure reimbursement, acquisition cost, direct and indirect remuneration fees, and the labor minutes tied to each fill. If the spread falls below fill cost plus workflow labor, more volume lowers profit instead of raising it.
Use the break-even mark as a daily control: 15 prescription-priced units/day is the model floor before debt, taxes, and reserves. Push generic dispensing where allowed, watch payer mix weekly, and flag low-margin scripts fast. Fill more of the right scripts, not just more scripts.
1
Drugstore Product Mix And Front-End Sales
Front-End Mix And Basket Size
When 60% of first-year sales come from prescriptions, the store depends on thin pharmacy economics. The front end matters because OTC, health and wellness, and beauty and personal care lift blended margin and can add cash for owner pay.
Here’s the quick math: the model uses a weighted unit price of $58.30, order value of $104.94, and 18 units per order. By Year 5, prescriptions fall to 55% and OTC plus health wellness rise to 35%, so profit improves only if stock turns stay fast and shrink stays controlled.
Track Mix, Turns, And Shrink
Measure mix by category each week: prescriptions, OTC, health wellness, and beauty personal care. Also track units per order, average order value, inventory turns, and shrink. The goal is simple: front-end sales should raise gross margin faster than they tie up cash in inventory.
- Watch category mix weekly.
- Compare turns against shrink.
- Test add-on items at checkout.
- Reorder only fast-moving SKUs.
If front-end sales rise but shrink stays high, owner income can drop even with better revenue. Build the forecast around the 60% to 55% prescription shift, then check whether extra OTC and wellness sales actually improve cash after inventory buys and spoilage.
2
Labor Model And Owner Role
Payroll and Owner Labor
Payroll is the biggest listed operating cost after variable costs. In Year 1, staffing totals $270k a year: pharmacist $130k, technician $45k, retail associate $30k, and store manager $65k. That works out to about $22.5k per month before owner pay, taxes, or debt service. One line matters most: if labor is too heavy for the sales base, owner take-home gets squeezed fast.
By Year 5, payroll rises to $425k as pharmacist FTE reaches 15 and retail associate FTE reaches 25. An owner who covers licensed hours can protect cash, but that is labor substitution, not free profit. If the store moves to a manager-led model, volume has to rise enough to cover that salary stack and still leave room for owner draw.
Track Labor Per Dollar Sold
Watch payroll as a share of sales, labor hours by role, and scripts per pharmacist hour. The key inputs are pharmacist FTE, technician hours, retail coverage, and store manager pay. If licensed hours are being covered by the owner, log those hours as an operating input so the real margin picture stays clear.
- Year 1 payroll: $270k total
- Year 5 payroll: $425k total
- Owner coverage: cash saver, not margin
- Manager-led model: needs higher volume
Here’s the quick test: if added sales do not cover the extra pharmacist, retail, and manager labor, the store is buying growth with thinner owner income. Keep staffing tied to prescription volume and front-end traffic, or the wage bill will outrun cash flow.
3
Inventory Purchasing And Wholesaler Terms
Inventory Purchasing And Wholesaler Terms
Inventory changes owner pay in two ways: it shapes gross margin and it traps cash. In year 1, inventory-related costs are modeled at 40% for pharmacy supply costs and 15% for shrinkage. By Year 5, those improve to 30% and 10%, so better buying and tighter control can lift take-home income.
The key inputs are purchase cost, shrink, inventory turns, and reimbursement timing. High-cost medications can sit on shelves before cash comes back, and poor turns can force bigger reserves even when accounting profit looks strong. That means the store may look profitable on paper, but the owner still can’t draw much cash.
Track Turns and Cash Lag
Measure inventory turns, shrink, and days between buying a drug and getting paid. Here’s the quick math: if supply cost is 40% and shrink is 15%, then almost 55% of inventory value is leaking from margin or loss before other fixed costs. Better wholesaler terms matter most when reimbursement is slow.
- Track days on hand weekly.
- Order to sales mix.
- Review shrink by category.
- Match payment terms to reimbursement.
Cut overbuying on expensive items, then reserve cash for fast-moving drugs and core front-end items. If turns stay weak, cash sits in stock instead of reaching the owner as a draw. That is the real risk: profit can look fine while distributable cash stays locked up.
4
Clinical Services And Patient-Care Add-Ons
Clinical Service Margin
Clinical add-ons like immunizations, medication therapy management, testing, delivery, medication synchronization, and adherence programs can raise revenue quality, but only if each visit pays for the extra time. This model gives no separate service revenue, reimbursement, staffing, or compliance cost, so do not book extra income without a case-specific scenario.
Here’s the quick math: if services use existing pharmacist capacity and bring repeat visits, the margin can be medium to high. If payer limits, documentation time, or unpaid work stack up, the gain can disappear fast. One clean rule: a service that does not cover its own labor and admin cost hurts owner pay, even if it looks busy.
Measure Service Profit Before You Scale
Track service count, reimbursement per service, minutes per visit, and repeat-patient rate. Compare that to pharmacist wage cost and any extra support time. If a service takes 20 minutes and creates no repeat fill or follow-up, it may add work without adding profit.
Start with services that fit open pharmacist hours and already bring patients back. Watch payer rules, charting time, and no-pay visits. If you cannot show positive margin after labor and admin time, keep the service as a retention tool, not a profit line. Busy is not the same as profitable.
- Track reimbursed vs. unpaid visits
- Measure time per service
- Test repeat-fill lift
- Limit low-paying payer contracts
5
Fixed Costs, Debt Service, And Cash Reserves
Fixed Costs And Cash Floor
Fixed costs set the monthly floor the store must clear before owner pay. Here, first-year fixed expenses are $112k per month or $1.344M per year, including $75k rent, $800 utilities, $500 insurance, $600 software, $1k marketing, and smaller operating lines. If operating profit stays below that floor, there is no clean path to owner distributions.
Debt service means loan principal and interest, and cash reserves mean money held back for taxes, reinvestment, and lean months. Those amounts are not provided, so owner income has to be modeled after operating profit, then reduced again for debt payments and reserves. One simple rule: every extra $10k per month in fixed costs adds $120k a year that has to come from store earnings.
Track The Cash Gap First
Start with a monthly cash forecast that shows operating profit, debt service, taxes, and reserve transfers. That tells you what is actually left for the owner. Don’t use profit alone; profit can look fine while cash is tight because loan payments and inventory timing still have to be funded.
- Track fixed costs monthly.
- Separate debt from operating profit.
- Set a reserve target.
- Watch rent as the anchor cost.
- Review owner draw after cash buffers.
To improve owner pay, keep fixed lines flat unless sales clearly support them. Test whether staffing, software, and marketing spend are tied to store traffic or just habit. If the business can’t cover $112k per month plus debt and reserves, owner pay must wait until the cash gap closes.
6
Compare low, base, and strong drugstore owner income scenarios
Owner income scenarios
Owner income moves with traffic, conversion, basket size, staffing, and inventory flow. These scenarios show the spread from a weak opening to a mature store.
| Scenario | Low CaseLow Case | Base CaseBase Case | High CaseHigh Case |
|---|---|---|---|
| Launch model | Owner income stays muted when traffic, conversion, and margin all run below plan. | Owner income tracks the first-year model when traffic, conversion, and costs land near plan. | Owner income rises fast when traffic, conversion, and basket size reach the Year 5 path. |
| Typical setup | Weekly visitors come in below the Year 1 plan, prescription margin weakens, front-end sales lag, staffing runs heavy, and debt service trims cash. | Weekly visitors average 550, conversion holds at 45%, orders average 1.8 units, revenue lands near $1.35M, and payroll and fixed costs stay on model. | Weekly visitors reach 1,200, conversion hits 55%, orders average 2.5 units, revenue reaches about $5.27M, and variable costs ease to 85%. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $0 - $0.8MLow Range | $1.1M - $1.3MBase Range | $25.1M - $44.4MHigh Range |
| Best fit | Use this to stress-test a slow start, thin margins, and tighter cash. | Use this as the core operating case for planning and lender discussions. | Use this to test upside if the store scales cleanly and inventory turns stay strong. |
Planning note: Scenario ranges are researched planning assumptions from the model, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Drugstore Porter's Five Forces Analysis
- Drugstore BCG Matrix
- Drugstore Business Model Canvas
- 7 Essential Financial KPIs for Drugstore Success
- Drugstore Business Plan Template in Pre-Written Word
- 7 Strategies to Increase Drugstore Profitability and Cash Flow
- What Are the Monthly Running Costs for a Drugstore in 2026?
- Drugstore Startup Costs: Plan For $785K Minimum Cash Need
- Drugstore Financial Model Template in Excel
- How To Open A Drugstore In 6 To 12 Months In The US
- How to Write a Drugstore Business Plan: 7 Actionable Steps
- Drugstore Marketing Mix
- Drugstore Marketing Plan
- Drugstore Business Proposal
- Drugstore PESTEL Analysis
- Drugstore Pitch Deck Example Editable PPTX
- Drugstore Business SWOT Analysis
- Drugstore Value Proposition Canvas
Frequently Asked Questions
In the base model, first-year operating cash flow capacity is about $797k on $135M revenue That is before owner draw, personal taxes, debt service, reserves, and reinvestment It also depends on payer mix, prescription margins, inventory cost, and staffing The data does not list a separate drug acquisition cost beyond supply and shrink lines