 Time to Open6-12 monthsSetup window
Time to Open6-12 monthsSetup windowHow To Open A Health Clinic: 6-12 Month US Launch Roadmap

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description

Time to Open6-12 monthsSetup window  Launch Sequence7 stagesConcept first
Launch Sequence7 stagesConcept first Key BottleneckPayer credentialingProvider coverage
Key BottleneckPayer credentialingProvider coverage First Revenue StepPaid visitsClean claims
First Revenue StepPaid visitsClean claims


Key Takeaways
- Licensing and payer setup must finish before launch.
- Staffing sets capacity, so hire to demand.
- Test billing workflows early to protect cash.
- Keep runway coverage ahead of reimbursement delays.
Time to Open6-12 monthsSetup windowLaunch Sequence7 stagesConcept firstKey BottleneckPayer credentialingProvider coverageFirst Revenue StepPaid visitsClean claimsLaunch timeline
Short web summary of the launch plan; the XLSX export carries the detailed Gantt chart.
Launch scheduleMonth 1Month 2Month 3Month 4Month 5Month 6Month 7Month 8Month 9Month 10Month 11Month 12
Legal / compliance
- Form entity docs
- Apply licenses
- Write policies
- Secure insurance
Site / buildout
- Shortlist sites
- Negotiate lease
- Start buildout
- Set up rooms
Equipment / IT
- Order equipment
- Set network
- Implement records system
- Test workflows
Staffing / training
- Hire physicians
- Hire support staff
- Complete onboarding
- Train clinical team
Payer / billing
- Start credentialing
- Set fee schedule
- Build billing rules
- Set collections process
Marketing / launch
- Define service mix
- Create patient materials
- Begin outreach
- Run soft opening
- Go live
Want to test the opening month before signing?
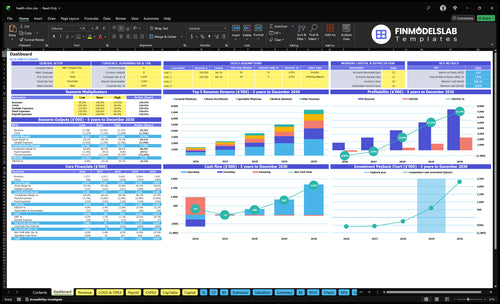
The screenshot maps dashboard and model tabs to revenue, costs, cash needs, assumptions, and break-even; open the Health Clinic Financial Model Template.
Financial model highlights
- Opening date and ramp
- 2 GPs, 1 NP
- 2 MAs, specialist, lab tech
- 55% to 75% capacity
- $114.4k run-rate
- Delayed collections, payer mix
- Fixed overhead, variable fees
- Cash runway, breakeven path
What do you need to open a health clinic?
To open a Health Clinic, form the entity, verify state corporate practice of medicine rules, line up licensed providers, get a 10-digit National Provider Identifier, enroll with payers, insure the clinic, and build HIPAA, facility, waste, medication, lab, and clinical policies before the first patient. Demand matters too: a 2022 Merritt Hawkins survey found new-patient physician wait times averaged 26 days in 15 large US metro markets, so validate access gaps with What Is The Current Growth Trend For Health Clinic's Patient Visits? before you sign a lease.
Legal setup
- Form the approved business entity
- Verify state medical ownership rules
- Secure licensed providers and supervision
- Carry malpractice and clinic insurance
Operating setup
- Get NPI and payer enrollment records
- Prepare HIPAA privacy and security workflows
- Confirm occupancy, waste, and medication handling
- Get CLIA status before lab testing
How long does it take to open a medical clinic?
For a Health Clinic, plan on 6 to 12 months to open. The real bottleneck is the critical path: lease talks, buildout, inspections, provider hiring, payer credentialing, EHR (electronic health record) setup, billing tests, and staff onboarding. Start payer work early; if hiring or payer approval slips, opening day can move even when the space is ready.
Main delay drivers
- Lease talks can set the pace.
- Buildout and inspections gate occupancy.
- Provider hiring affects opening day.
- Payer credentialing takes time.
Start early
- Begin payer work before signage.
- Set up EHR early.
- Test billing before launch.
- Onboard staff in sequence.
What common mistakes delay a health clinic launch?
Health Clinic launches get delayed when the clinic opens before payer enrollment is usable, then has no clean way to bill visits. Delays also stack up when providers are hired late, or when front desk, medical assistant, nursing, billing, scheduling, HIPAA, and clinical policies are still unfinished. Use readiness gates, a soft opening, staff drills, clean claim testing, and a cash runway check before the opening month.
Billing and staffing first
- Payer enrollment must work before opening.
- Hire providers before launch month.
- Staff front desk and billing early.
- Test claims before the first visit.
Ops and compliance checks
- Finish HIPAA and clinical policies first.
- Stress-test appointment scheduling.
- Confirm EHR, lab, waste, IT, supplies.
- Open marketing only when slots exist.
Confirm the clinic is legally, operationally, and commercially ready to open
Launch readiness checklist
Use this go-live approval checklist before opening the clinic.
Compliance
- Entity and licenses filedCritical
The clinic cannot open without the legal entity and state medical approval.
- Provider IDs confirmedCritical
Billing and payer setup depend on active provider IDs.
- Malpractice policy boundCritical
Coverage must be live before any patient visit starts.
- HIPAA workflows approvedHigh
Protected health data needs rules for access, storage, and sharing.
Site
- Lease and occupancy clearedCritical
The clinic needs legal use of the space before opening day.
- Exam rooms readyHigh
Visit flow breaks if rooms, furniture, and fixtures are not ready.
- Lab and security installedHigh
Lab access and site security need to work before patient intake starts.
Systems
- EHR configuredCritical
The record system must work before the first chart is opened.
- Billing workflow testedCritical
Claims, copays, and collections need to run without blocking cash.
- CLIA status confirmedHigh
If lab testing applies, CLIA status must be in place before testing.
Staffing
- Seven-role team staffedCritical
Year 1 needs the seven-role team in place to open cleanly.
- Coverage schedules publishedHigh
Visits stall if coverage, breaks, and handoffs are not set.
- Clinical training completedHigh
Staff need clear steps for visits, charting, and escalation.
Revenue
- Appointment booking liveCritical
Patients need a working way to book before the first revenue step.
- Payment collection testedHigh
Copays and self-pay collections support cash on day one.
- Payer enrollment liveCritical
Insurance billing cannot start until payer enrollment is active.
Cash
- Month 14 runway coveredCritical
The model hits minimum cash in Month 14, so runway must cover that gap.
- Minimum cash fundedCritical
The clinic needs about $319k at the low point to stay open.
- Go-live signoff approvedCritical
No launch should start while billing, staffing, or occupancy is blocked.
Want the six launch drivers that matter most?
1Regulatory Ready
License gateLicensing, credentialing, and payer enrollment decide whether visits get paid cleanly or turn into launch-month cash gaps.
2Site Setup
6-12 moLease, permits, and buildout control when the clinic can open and how smoothly patients move through the space.
3Staff Ready
7 rolesYear 1 staffing of seven clinical roles sets appointment capacity and keeps billing and supervision from breaking at launch.
4Systems Billing
Clean claimsTested scheduling, charting, coding, and claims flow cut rework and speed collections after the first visit.
5Patient Demand
1,528/moLocal search, referrals, and booking must fill schedules or the clinic misses its planned Year 1 volume.
6Cash Discipline
$319KAt $114.4K monthly run-rate and 17% direct load, weekly cash tracking protects payroll through Month 14.
Regulatory, Credentialing, And Payer Readiness
Credentialing Is the Go-Live Gate
This is critical path, not back-office work. A clinic can have rooms and staff ready, but if licensed providers, NPI setup, payer enrollment, malpractice coverage, HIPAA workflows, clinical policies, and state compliance are not complete, it cannot bill cleanly from day one. At the stated Year 1 run-rate of $114,410 per month, even a short reimbursement lag can strain cash.
One clean claim, meaning a claim paid without rework, is better than ten rushed visits. If the clinic opens before insurance contracts and billing rules are set, patients may be treated before revenue is predictable.
Get Paid Before First Patient Day
Build the payer file before you open: provider credential files, payer applications, insurance contracts, billing rules, and compliance training. Here’s the quick math: at 17% variable costs and $11,500 in fixed overhead before IT support, monthly cash needs stay high while reimbursements are still moving.
- Confirm every provider license.
- Verify NPI and payer IDs.
- Store malpractice documents.
- Test HIPAA and billing workflows.
- Train staff on denial handling.
If payer enrollment slips, the clinic may still see patients but collect slowly, and that is how launch-month cash gaps start.
1
Location And Facility Setup
Location And Facility Setup
The clinic can’t open on time if the space is still waiting on occupancy approval, exam room compliance, or landlord work. The readiness signal is simple: signed lease, compliant exam rooms, parking, signage, secure records areas, and safe medical waste handling are all in place, so patients can walk in and be treated on day one.
This driver also shapes the first patient experience. Good patient flow, smart equipment placement, and clear storage reduce bottlenecks at check-in and cut opening-day fixes. The risk is paying rent before the site can treat anyone, which burns cash with no offsetting revenue. That’s the real squeeze here.
Buildout Before First Patient
Start with the lease, then map the buildout sequence around inspections, vendor lead times, furniture, IT, and clinical equipment. Don’t buy or install anything before the room layout is fixed. Here’s the quick math: every day the site sits ready-but-closed pushes rent and other overhead forward without patient revenue.
Use a simple opening checklist and assign one owner for each item: landlord work, occupancy approval, parking and signage, exam rooms, records security, and waste pickup. Test the path from parking to check-in to exam room before launch. If that flow feels awkward for staff, it will feel worse for patients.
- Confirm occupancy approval first
- Verify room and storage compliance
- Place equipment around patient flow
- Lock down records and waste handling
2
Provider And Staff Readiness
Provider And Staff Readiness
Staffing sets the clinic’s day-one capacity. With 2 general physicians, 1 nurse practitioner, 2 medical assistants, 1 specialist physician, and 1 phlebotomist lab tech, the team only opens as fast as those shifts, licenses, and supervision rules are ready. If schedules or onboarding slip, the clinic can launch late or open with too few appointment slots, which creates wait times and cuts early revenue.
This driver also affects billing quality. Front desk coverage, billing support, and backup plans need to be in place before the first patient, or the clinic risks missed charges, missed intake steps, and messy handoffs. The bottleneck is simple: demand without slots. No coverage means no visits, even if the phones are ringing.
Lock Coverage Before Launch
Verify every provider has active licenses, approved schedules, and clear onboarding dates before you set an opening date. Also confirm supervision rules for the nurse practitioner and specialist coverage, plus who handles front desk, billing, and phlebotomy on each shift. If one role is missing, the clinic should not promise full hours.
Use a written staffing map for week 1, then test it against real patient flow. Build a backup plan for sick calls, no-shows, and late credentialing so the clinic can still open with a workable schedule. One uncovered shift can wipe out same-day access and delay clean billing from the start.
3
- Check licenses before scheduling visits.
- Confirm supervision for midlevel care.
- Assign front desk and billing coverage.
- Train backups for absences and delays.
- Match slots to staffed hours only.
Clinical Systems, EHR, And Billing Workflow
EHR and Billing Workflow Testing
When the clinic opens, every visit has to move from check-in to coding to claims submission without a break. If scheduling, intake, charting, patient payments, reminders, reporting, lab links, and denial tracking are not tested first, completed visits can’t be billed cleanly, which slows cash and creates rework on day one.
That matters at a $114,410 monthly revenue run-rate. Using the stated 17% variable cost load, about $19,450 a month depends on the billing engine working right, so weak setup can turn a normal first month into a cash squeeze.
Test the full claim path before opening
Run the full workflow end to end: scheduling, intake, charting, coding, claim submission, patient payment, reminders, reporting, and denial follow-up. Verify payer setup, provider records, fee schedules, and staff training before the first patient is seen. One clean test run now is cheaper than weeks of manual fixes later.
- Submit test claims and fix rejects.
- Confirm lab integration, if used.
- Train front desk on payment capture.
- Track denials from day one.
4
Patient Demand And First Appointments
Patient Demand and First Appointments
This launch driver matters because a clinic can open on time and still miss day-one revenue if patients do not turn into booked and completed visits. The readiness signal is not just awareness; it is visible demand through local search, insurance directories, referral sources, and a working booking path.
Plan the launch around the first appointment funnel: online booking, call handling, review requests, and follow-up scripts. The Year 1 patient acquisition assumption is 6% of revenue, so weak execution here creates the bottleneck of awareness without filled schedules, which delays utilization toward planned Year 1 capacity levels.
First-Visit Readiness Check
Before opening, verify that the clinic can capture, book, and confirm patients in one flow. Here’s the quick math: if search, referral, and employer outreach are live but the phone script or online scheduler fails, demand leaks before the first visit is set.
- Confirm local search and directory profiles.
- Test online booking and call handling.
- Assign review and follow-up scripts.
- Track booked, confirmed, completed visits.
- Monitor capacity fill before launch.
What this setup hides is simple: patient demand only helps if it converts into appointments the team can actually complete. If follow-up is slow or insurance visibility is weak, first-week utilization stays soft and the clinic starts with empty slots instead of active care.
5
Financial Runway And Operating Discipline
Cash Runway Discipline
If the clinic opens before cash timing is mapped, day-one care can outrun cash. At stated capacity, monthly revenue is about $114,410; direct and variable costs are 17%, so about $94,861 remains before fixed overhead. The listed fixed overhead is $11,500 per month before IT support, so the real risk is not demand — it’s payroll, rent, and reimbursement timing.
Model the revenue ramp before opening, not after. A clinic can be full on paper and still miss payments if claims settle late or staff are paid before collections land. The readiness check is simple: can cash cover payroll, rent, vendors, and a reimbursement lag buffer while weekly visits build? If not, opening on time gets fragile fast.
Build the cash buffer first
Before opening, verify the cash plan against the first weeks of billing and operating spend. Here’s the quick math: $114,410 monthly revenue at capacity, less 17% variable cost, leaves about $94,861 before the $11,500 fixed overhead line. That still does not cover unknown IT support or any delay in payer reimbursement, so the clinic needs a buffer, not just a forecast.
- Cover payroll before collections
- Cover rent on opening month
- Set vendor payment dates
- Hold a reimbursement lag buffer
- Track weekly breakeven
- Review cash and claims weekly
What this estimate hides is timing. Supplies, lab outsourcing, patient acquisition, and billing fees hit fast, but cash from insurers and patients may not. A weekly operating dashboard should show cash on hand, unpaid claims, payroll due, and open payables so the team can spot trouble before it delays care or forces rushed spending cuts.
6
Related Products
- Health Clinic Porter's Five Forces Analysis
- Health Clinic BCG Matrix
- Health Clinic Business Model Canvas
- 7 Critical KPIs to Scale Your Health Clinic
- Health Clinic Business Plan Template in Pre-Written Word
- How to Increase Health Clinic Profitability with 7 Key Strategies
- How to Manage Monthly Running Costs for a Health Clinic
- Health Clinic Startup Costs: $375K+ CAPEX Plus Launch Runway
- Health Clinic Financial Model Template in Excel
- How Much Does a Health Clinic Owner Make on $137M Year 1 Revenue
- How to Write a Health Clinic Business Plan: 7 Actionable Steps
- Health Clinic Marketing Mix
- Health Clinic Marketing Plan
- Health Clinic Business Proposal
- Health Clinic PESTEL Analysis
- Health Clinic Pitch Deck Example Editable PPTX
- Health Clinic Business SWOT Analysis
- Health Clinic Value Proposition Canvas
Frequently Asked Questions
Start with entity setup, state healthcare ownership rules, licensed providers, malpractice coverage, National Provider Identifier records, payer enrollment, and HIPAA workflows Then line up the facility, EHR, billing, and policies The researched Year 1 plan assumes 7 clinical roles and about 1,528 completed monthly services once capacity is reached