 Time to Open12-24 monthsLaunch runway
Time to Open12-24 monthsLaunch runwayStart A Helicopter Medevac Service: 12–24 Month Launch Roadmap

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description

Time to Open12-24 monthsLaunch runway  Launch Sequence7 stagesRegulatory first
Launch Sequence7 stagesRegulatory first Key BottleneckCompliance gateFAA and EMS rules
Key BottleneckCompliance gateFAA and EMS rules First Revenue StepSigned referralsHospital contracts
First Revenue StepSigned referralsHospital contracts


Key Takeaways
- No authority, no compliant helicopter missions.
- State EMS approval gates patient transport.
- Staffing, dispatch, and referrals drive safe volume.
- Cash runway turns negative by Month 6.
Time to Open12-24 monthsLaunch runwayLaunch Sequence7 stagesRegulatory firstKey BottleneckCompliance gateFAA and EMS rulesFirst Revenue StepSigned referralsHospital contractsLaunch timeline
This is a short web summary of the launch plan, and the XLSX export holds the full Gantt chart with task-level detail.
Launch scheduleMonth 1Month 2Month 3Month 4Month 5Month 6Month 7Month 8Month 9Month 10Month 11Month 12
Regulatory / compliance
- License map
- FAA filing
- State EMS file
- Insurance bind
- Approval review
Aircraft / facilities
- Helicopter order
- ICU fitout
- Hangar buildout
- Safety gear issue
- Readiness inspection
Medical operations
- Clinical protocols
- Triage workflow
- Transfer standards
- Drill scenarios
- Medical signoff
Staffing / training
- Hire chief pilot
- Recruit flight crew
- Train clinicians
- Crew coverage plan
- Recurrency schedule
Dispatch / billing
- Install dispatch
- Test satellite links
- Set billing flow
- Collections workflow
- Revenue controls
Hospital outreach / launch
- Hospital target list
- Meet referral teams
- Standby retainer offers
- Go-live drills
- Launch week coverage
Why pressure-test launch before the first mission?
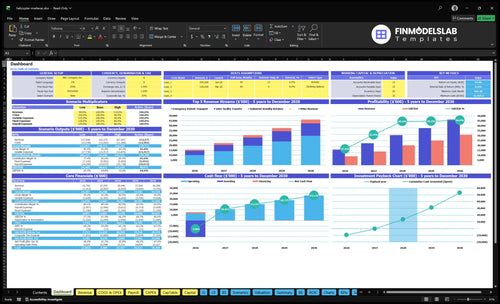
This screenshot and the Helicopter Medical Evacuation Service Financial Model Template show revenue, costs, cash needs, assumptions, and break-even logic.
Financial model highlights
- Launch timing dashboard
- Mission ramp schedule
- Cash runway chart
- Break-even path
- 400 transports at $25k
- 250 transfers at $18k
- 10 retainers at $120k
- 65% fuel, 25% consumables
- 70% maintenance, 35% billing
- Month 6 cash low
- 1 chief pilot, 4 nurses
- 4 paramedics, 4 pilots, 2 techs, 4 dispatchers
What are the biggest mistakes when launching a helicopter medevac service?
The biggest mistake in launching a Helicopter Medical Evacuation Service is buying aircraft before the FAA operating path and EMS licensure are locked, because the first six months already carry $1,545 million in capex and minimum cash falls to -$11,425 million in Month 6. With fixed costs around $99,200 per month before wages, any slip in staffing, dispatch, billing, or referral contracts should trigger a no-go call. Here’s the quick math: readiness gaps get expensive fast.
Launch traps
- Buy aircraft too early
- Treat EMS licensure as paperwork
- Understaff pilots and clinicians
- Skip dispatch coverage planning
Cash and risk gaps
- Miss billing and payer workflows
- Underinsure aviation and clinical risk
- Launch without referral pathways
- Hold go-live if approvals slip
How does a helicopter medevac service get its first customers?
First customers for a Helicopter Medical Evacuation Service come from signed referral access, not walk-in demand, so the launch focus should be hospitals, trauma centers, rural health systems, EMS agencies, event or industrial standby buyers, and interfacility transfer coordinators. A Year 1 model with 400 emergency transports at $25,000 each, 250 interfacility transfers at $18,000, and 10 standby retainers at $120,000 points to about $15.7 million in gross revenue, so the first step is building dispatchable pathways before go-live; see How Do I Launch A Helicopter Medical Evacuation Service?
Referral sources
- Target trauma centers first
- Open rural health system access
- Line up EMS agency referrals
- Secure interfacility coordinators
Revenue setup
- 400 emergency transports planned
- 250 transfer jobs planned
- 10 standby retainers planned
- Build active referral pathways
What licenses are needed to start a helicopter medevac service?
A Helicopter Medical Evacuation Service needs Federal Aviation Administration operating authority, often through 14 CFR Part 135 commercial operations or a qualified operating partner, plus a state EMS air-ambulance license before patient flights; for cost context, see What Are Operating Costs For Helicopter Medical Evacuation Service?. This is not legal advice, so verify with FAA counsel, state EMS officials, and aviation compliance specialists before go-live.
Core licenses
- FAA aviation operating authority
- 14 CFR Part 135 compliance path
- State EMS helicopter transport license
- Local medical transport rule approval
Launch blockers
- Medical director oversight not approved
- Clinical protocols not signed
- Aircraft medical configuration not ready
- Maintenance, pilots, documentation misaligned
Confirm whether the helicopter EMS service is ready for day-one missions
Launch readiness checklist
Use this go-live approval checklist before opening to confirm the helicopter medevac service is ready to start.
Regulatory
- Entity formedCritical
A legal entity must exist before permits, contracts, and insurance can bind.
- FAA authority verifiedCritical
Flights need approved operating authority or a signed operator relationship.
- State EMS path setCritical
State EMS approval gates patient transport and care scope.
- Insurance boundCritical
Aviation, liability, and medical malpractice cover must be active.
Aircraft
- Helicopters acquiredCritical
Aircraft must be secured before crew, maintenance, and dispatch can launch.
- ICU fitout completeCritical
Medical gear has to match the care scope for first patient calls.
- Maintenance program approvedCritical
A logged maintenance plan keeps aircraft airworthy from day one.
Crew
- Chief pilot hiredHigh
One accountable lead is needed for flight standards and safety.
- Flight nurses hiredHigh
Clinical coverage must match the first operating schedule.
- Flight paramedics hiredHigh
Patient care needs trained medics ready for launch month calls.
- Line pilots hiredCritical
Enough pilots must be in place for launch month coverage.
- Maintenance techs hiredHigh
Maintenance staffing protects uptime and airworthiness.
Dispatch
- 24/7 dispatch testedCritical
Calls, alerts, and handoffs must work around the clock.
- Satellite comms liveCritical
Flight crews need reliable links when ground networks fail.
- Hospital routing testedHigh
Hospitals need a clean path to request and accept flights.
- Emergency alerts drilledHigh
Drills show whether escalation works under pressure.
Revenue
- Referral contracts signedCritical
Signed referral paths drive the first patient transports.
- Payer billing readyHigh
Claims setup must support the Year 1 collection-fee rate.
- Billing workflow readyHigh
Claims, denials, and follow-up need a clear owner.
- Collection fee model setMedium
The model uses a 3.5% billing and collection fee assumption.
Finance
- Month 6 cash coveredCritical
The model bottoms at Month 6, about $11.425M below zero.
- Utilization ramp reviewedHigh
Year 1 assumes 400 transports, 250 transfers, and 10 retainers.
- Go-live signoff completeCritical
No launch until licensing, aircraft, dispatch, insurance, and referrals are signed.
- Payback window acceptedMedium
The model shows a 25-month payback, so capital must stay patient.
Which six drivers decide whether this service can launch?
1Aviation Gate
12-24 moNo compliant aircraft means no missions, so FAA authority and ready equipment gate launch timing.
2EMS License
License gateState EMS approval and medical director signoff control permission to treat, not just fly.
3Crew Staffing
21.3MCredentialed, rested crew keeps coverage safe; weak staffing forces mission delays or cancellations.
4Dispatch Comms
2-5 mo24/7 dispatch, flight following, and weather checks tighten go/no-go calls and first-mission execution.
5Referral Network
400/250/10Signed referral paths turn aircraft access into first revenue and ramp early mission volume.
6Cash Runway
-$11.4MBilling, insurance, and collection lag can drain cash fast; the model bottoms at Month 6.
Aviation Authorization And Aircraft Readiness
FAA Authority and Aircraft Readiness
This launch gate decides whether the service can fly on day one. You need FAA operating authority or a qualified Part 135 air ambulance path, plus aircraft availability, maintenance, pilot qualifications, operational control, medical configuration, and safety gear. The setup plan shows $125 million for helicopters in Months 1–6, $18 million for ICU in-flight equipment in Months 1–3, and $150,000 for crew safety gear in Months 3–6.
No compliant aircraft, no missions. If the company spends before authority, maintenance, and control are ready, cash leaves early and launch slips even if the helicopters are on site. The real bottleneck is not buying equipment; it’s proving the aircraft can fly legally, safely, and with the right medical setup from the first call.
Lock the flight path first
Start with the approval route, then match every asset to that route. Verify the aircraft is available, the maintenance program is in place, pilots meet requirements, operational control is documented, and the cabin fits the medical mission. That sequence keeps the buildout tied to launch permission, not wishful timing.
Here’s the quick test: if the aircraft, crew, and paperwork were ready today, could a mission launch without a compliance gap? If the answer is no, delay the purchase or phase the spend. The setup total here is $143.15 million, so even a short delay before authority can trap a lot of cash before first revenue.
- Confirm authority before buying aircraft.
- Match cabin gear to mission use.
- Document maintenance and control.
- Stage safety gear last.
- Test day-one dispatch readiness.
1
EMS Licensing And Medical Governance
EMS License and Medical Oversight
If you do not have state EMS approval and medical director signoff, you cannot transport patients on day one. This license controls scope-of-care, treatment protocols, patient care documentation, quality assurance, and medication or equipment controls, so it is the real launch gate for clinical work.
The timing risk is real: the model puts $18 million of advanced ICU in-flight medical equipment in Months 1–3, so the clinical setup must match the approved care plan. Aviation approval alone only allows transport; EMS licensing gives permission to provide care.
Get Clinical Signoff First
Lock the license path around the exact equipment list, care scope, and medical director review before purchase or install. Verify what the state needs for protocols, patient records, QA, and controlled meds or gear, because a mismatch can delay opening even if the helicopter is ready.
Use a simple launch gate: state EMS license first, then medical director signoff, then patient transport. If either step slips, you can still own the aircraft, but you cannot serve patients from day one.
2
Clinical And Flight Crew Staffing
Crew Staffing Readiness
For a helicopter emergency medical service, staffing is a launch gate. You can have aircraft and protocols ready, but without enough credentialed, rested crew, you can’t accept missions safely or keep coverage live from day one.
Here’s the quick math: Year 1 wages are about $2.127 million, including 1 chief pilot at $185,000, 4 flight nurses at $115,000 each, 4 flight paramedics at $98,000 each, 4 line pilots at $145,000 each, 2 maintenance technicians at $105,000 each, and 4 dispatchers at $75,000 each.
Build Coverage Before Go-Live
Before opening, verify credentialing, training, coverage schedules, fatigue management, and backup coverage. The real bottleneck is accepting missions with too few rested or qualified people, which can force cancellations, delay response, or create compliance risk. Safe, continuous coverage depends on the crew plan being locked before the first dispatch.
- Confirm credentials match flight duties.
- Map day, night, and backup shifts.
- Test fatigue and rest rules.
- Assign backups for sick calls.
- Train dispatch on crew availability.
3
Dispatch And Communications Readiness
24/7 Dispatch Control
For a helicopter medical evacuation service, dispatch is the launch gate for day-one operations. You need 24/7 call intake, mission triage, flight following, weather decision support, hospital coordination, and documented procedures before the first patient call. The setup budget includes $350,000 for dispatch and satellite communications in Months 2–5, plus $6,500 per month for systems in Year 1.
If dispatch is weak, aircraft and clinical crews may be ready but still unable to launch cleanly. The staffing plan calls for 4 dispatchers at $75,000 each, so coverage and handoffs must be built for nonstop operations. The real risk is poor operational control: slower response, bad go/no-go calls, and a messy first mission when hospitals expect immediate coordination.
Lock the call path before go-live
Before opening, verify the intake script, escalation tree, weather rules, flight-following process, and hospital contact list. Test every step, including after-hours backup and satellite failover, so the first real call does not become the process test. One missed handoff can delay launch even if the aircraft and medical crew are already in place.
Document who makes the call, who records it, and who approves launch. Use the same procedure for every mission, because consistency matters more than speed on paper. Here’s the quick check: 24/7 coverage, documented dispatch SOPs, weather decision support, and hospital coordination all working before day one.
- Test intake after hours.
- Confirm weather call authority.
- Train dispatcher handoffs.
- Back up satellite communications.
4
Hospital And EMS Referral Network
Referral Network Before First Flight
This launch driver decides whether the helicopter service has patients on day one. If signed referral pathways with hospitals, trauma centers, rural facilities, EMS agencies, transfer centers, and industrial standby buyers are not in place, you can still open the operation but not fill missions. The model assumes 400 emergency transports, 250 interfacility transfers, and 10 standby retainers, so the first revenue ramp depends on active channels, not just aircraft readiness.
Here’s the quick math: at $25,000, $18,000, and $120,000 pricing, modeled annual revenue is about $15.7 million. That only happens if outreach starts early and referral partners know when to call, who approves transfers, and what service area you cover. If aircraft and crew launch before those pathways are signed, fixed costs start first and mission volume lags.
Build the Referral Path Before Go-Live
Before opening, lock the call flow with each referral source: who can request a flight, who authorizes transfer, how fast contact gets answered, and what records are needed. Set the outreach budget at the modeled $12,000 per month and tie it to named targets, not broad marketing. Day-one readiness means the phone rings, the handoff is clear, and the dispatch team can turn interest into missions.
- Confirm signed hospital and EMS contacts.
- Document transfer and standby criteria.
- Test referral response times before launch.
- Assign one owner for outreach follow-up.
- Track leads, calls, and mission conversion.
What this estimate hides is ramp speed. If referral agreements slip by even a few weeks, you still pay outreach, staffing, and aircraft-ready costs, but you delay first missions. That creates a cash gap early, so launch timing should follow signed pathways, not the other way around.
5
Billing, Insurance, And Cash Runway
Billing, Insurance, and Cash Runway
If the helicopter is ready but billing and insurance are not, launch cash can disappear fast. This model carries $55,000 in monthly aviation and liability insurance, 35% Year 1 billing and collection fees, and about $99,200 in fixed overhead each month before wages, so the first missions must be set up to collect cleanly.
That means payer setup, claims workflow, denial handling, and medical malpractice coverage need to be in place before go-live. The model’s cash low lands in Month 6, so runway testing has to include launch timing, staffing ramp, utilization ramp, and collections lag. One bad billing setup can turn early transport volume into a cash squeeze.
Prelaunch Cash and Claims Setup
Before opening, verify every coverage line, payer enrollment step, and claim handoff. A medevac launch needs aviation insurance, liability insurance, and medical malpractice coverage active on day one, plus a defined path for coding, submission, denial review, and follow-up. If collections are slow, the service can look busy and still run short on cash.
Build the runway case with realistic lag, not best case. Test how much cash is needed if billing takes longer than planned, if denials rise, or if mission volume ramps slower than staffing. The hard rule is simple: no open date until the claims process can support first revenue and the model still survives the Month 6 cash trough.
- Enroll payers before first transport.
- Map claim steps and owners.
- Track denial reasons weekly.
- Match cash to collections lag.
- Stress test Month 6 runway.
6
Related Products
- Helicopter Medical Evacuation Service Porter's Five Forces Analysis
- Helicopter Medical Evacuation Service BCG Matrix
- Helicopter Medical Evacuation Service Business Model Canvas
- What Are The 5 KPIs For Helicopter Medical Evacuation Service Business?
- Helicopter Medical Evacuation Service Business Plan Template in Pre-Written Word
- How Increase Profits Helicopter Medical Evacuation Service?
- What Are Operating Costs For Helicopter Medical Evacuation Service?
- Helicopter Medevac Startup Costs: $1545M CAPEX Plan
- Helicopter Medical Evacuation Service Financial Model Template in Excel
- How Much Helicopter Medevac Owners Can Make At $157M Revenue
- How To Write A Business Plan For Helicopter Medical Evacuation Service?
- Helicopter Medical Evacuation Service Marketing Mix
- Helicopter Medical Evacuation Service Marketing Plan
- Helicopter Medical Evacuation Service Business Proposal
- Helicopter Medical Evacuation Service PESTEL Analysis
- Helicopter Medical Evacuation Service Pitch Deck Example Editable PPTX
- Helicopter Medical Evacuation Service Business SWOT Analysis
- Helicopter Medical Evacuation Service Value Proposition Canvas
Frequently Asked Questions
No, ownership is not the only path, but operational control and compliance must be clear You can buy, lease, or work with a compliant aviation operator The researched setup assumes $125 million for helicopter acquisition in Months 1–6, so founders should compare ownership against lease or partner models before locking cash into aircraft